The Role of PSMA PET Imaging in Prostate





























 • Started on ADT • +/-")










 (11/19)")

















- Slides: 61
The Role of PSMA PET Imaging in Prostate Cancer A/Prof Jeremy Grummet UAA Congress Singapore 2016
Disclosures • Urologist in private and public practice • UAA Congress attendance sponsored by Biobot (i. S’Robot Mona Lisa)
We transform lives
We can cure
But we can harm SEX LIFE SOCIAL LIFE
Sometimes we do both • If we know we we’re going to risk harming our patient, we’d better be sure there’s a good reason • Accurate diagnosis - MRI • Accurate staging
Staging • Knowledge of extent of disease is cornerstone of decision-making William Halsted in: The Emperor of All Maladies
Staging in prostate cancer • For “high risk” disease
“High risk” of inappropriate treatment OVERTREATMENT UNDERTREATMENT
Staging in prostate cancer • Current standard is hopelessly inadequate • Local treatment with curative intent for high risk clinically localised disease, by definition, often fails • Sometimes due to positive margin • Often due to distant metastases already there
Re-staging • Same problem • Current imaging at early PSA recurrence postlocal treatment is useless • If initial treatment was radical prostatectomy, decision re early salvage radiotherapy is no more than educated guesswork
Salvage radiotherapy
We desperately need something better
68 Ga-PSMA PET imaging
68 Ga-PSMA PET imaging • Developed at Heidelberg University • PSMA is a membrane-bound enzyme – Catalytic site in extracellular domain (cf. Prostascint) • 68 Ga-PSMA is a PSMA inhibitor – Ligand binds to PSMA and is internalised Maurer et al
Normal • Lacrimal glands • Salivary glands • Liver • Spleen • Small bowel • Urinary tract
Pitfalls • Ureters • Coeliac ganglia • Thyroid and adrenal adenoma • Paget’s disease • Other solid organ cancers: colon, kidney, lung…
Real cases
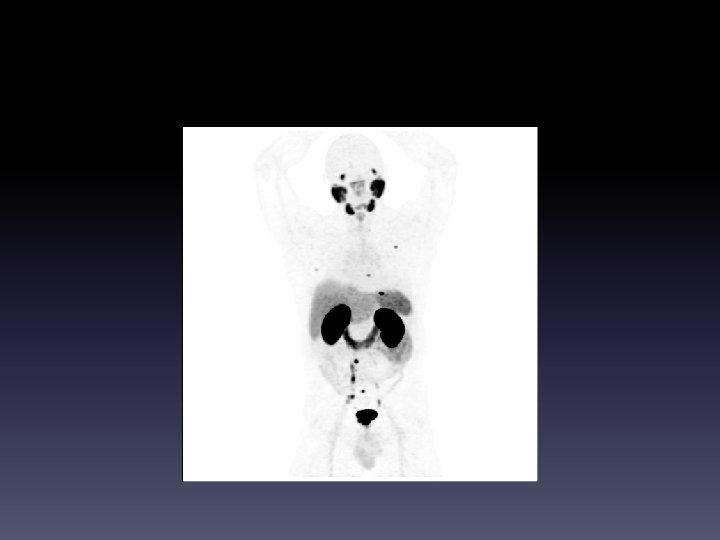
Initial staging – nodal mets • 68 yo man • PSA 110 • Biopsy GG 4 (Gleason 8) • Bone scan negative • CT negative
Primary
Pelvic LN
Retroperitoneal LN
Mediastinal LN
Supraclavicular LN
Initial staging – clinically localised • 50 yo man • PSA 10. 9 • DRE benign
Initial staging – pelvic LN • 75 yo man • PSA 12 • GG 5 (Gleason 9)
Avid in prostate, single LN
1 positive right sided LN
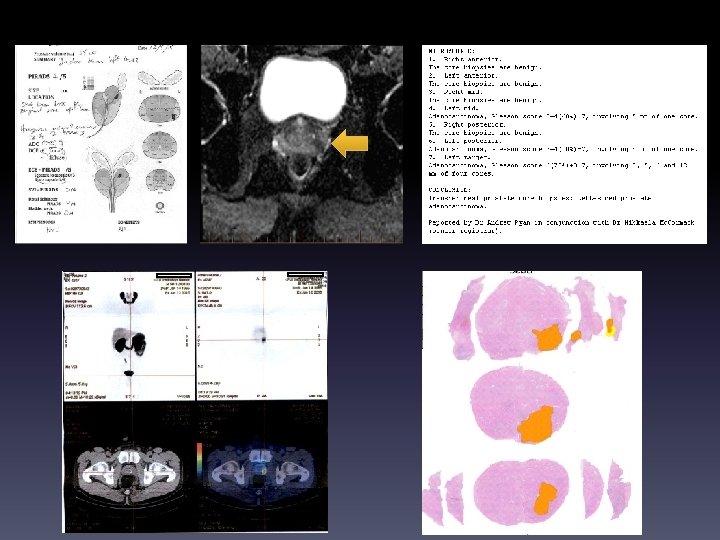
Initial staging – bone and LN mets • 58 yo man • GP watching rising PSA, now 8. 8 • PHI 175 (norm < 45) • MRI PIRADS 5/5, pelvic LNs up to 2 cm • Skipped to PSMA PET before biopsy
• Biopsy showed GG 5 (Gleason 9) • Started on ADT • +/- chemo • Offered enzalutamide RCT (ENZAMET) • ? Role of treatment of primary
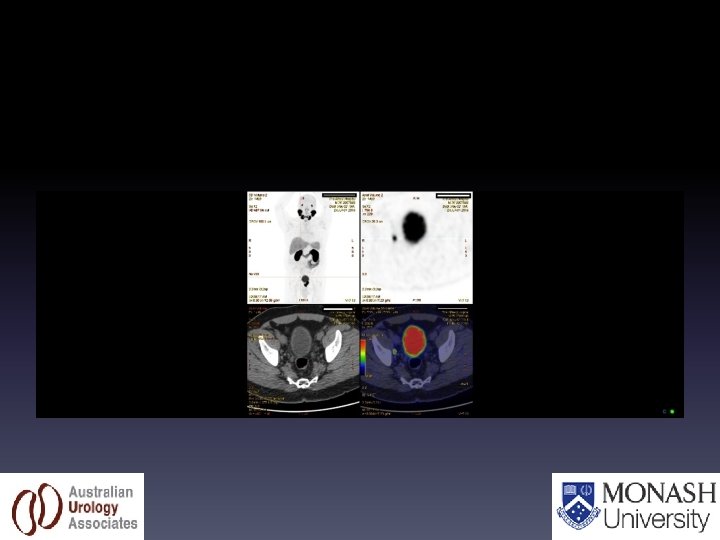
Re-staging after XRT • 70 yo man • XRT 2005, PSA dropped to 1. 0 • PSA now 15 • BS, CT negative
0/18 LYMPH NODES
Data
Literature TO JUNE !!
Re-staging • Current EAU guidelines recommend restaging imaging when symptomatic or PSA > 10
Re-staging - Heidelberg 319 pts, 83% PSMA PET positive, 901 lesions
Re-staging - Heidelberg • 42 patients had lesion histology • Of 446 lesions, only 30 missed – All other lesions true positive or true negative • Lesion based sensitivity 77% – 98 TP / 128 (98 TP + 30 FN) • Specificity 100% (no false positives)
Re-staging PSMA PET: Heidelberg
Re-staging PSMA PET: Munich 248 pts, 90% PSMA PET positive
Re-staging PSMA PET: Munich • Only 12 pts had histology confirmation • 35 pts had PSA decrease after stereotactic XRT to PSMA PET positive lesions • 45 pts follow-up imaging showed PSMA PET positive lesions were mets • 37% (92/248) had reference, all showing true positives
Re-staging PSMA PET: Munich (24/33) (11/19)
Re-staging PSMA PET: Munich • PSA < 1 • PSMA PET positive rate of 67% • Compared to choline PET positive rates of 1936%
Re-staging PSMA PET – Our data 70% 88% 31% 0% 58%
Initial staging - Munich 130 pts intermediate or high risk prostate cancer 95 had PSMA PET/MRI, 35 had PSMA PET/CT
Initial staging - Munich • >90% primary tumour PSMA avid
• 18 F-choline vs 68 Ga-PSMA PET comparison • 37 pts, 78 lesions • Choline PET detected 26, PSMA PET detected 56 (incl all Choline PET lesions), p = 0. 04 • PSMA PET tumour: background ratio clearly higher in 95% Prospective trial needed to prove
? Initial diagnosis • 53 pts, biopsy proven intermed-high risk prostate cancer
? Initial diagnosis • PSMA PET/MRI vs mp. MRI vs PSMA PET • AUC: 0. 88 vs 0. 73 vs 0. 83 (p = 0. 002) • Methodological issues – Selected cohort only positive for cancer – Sextant system led to potential for wrong assignment of location – Used only PIRADS v. 1
Systematic review
Review • Nature Reviews Urology April 2016
Review
Future directions • Due to its high sensitivity and specificity, 68 Ga PSMA PET promises to replace CT and bone scan for staging of intermediate to high risk prostate cancer and restaging of recurrent cancer after local treatment of the primary • Current data on small numbers but very compelling • Law of small numbers would predict regression to mean as more data come in, but likely to remain far superior to current standard
Future directions • Superior to choline PET, however prospective studies needed to prove this • About 10% of prostate cancers are not PSMA avid • Combination of optimal molecular, functional and anatomical imaging using PSMA PET /MRI is likely to provide the most accuracy for diagnosis and staging in a single test • More accurate knowledge reframes our clinical decision-making – ? Should men with mets seen only on PSMA PET still undergo local treatment to the primary
Future directions • Will enable more appropriate use of salvage radiotherapy • May allow effective use of stereotactic radiotherapy to oligometastases (trials ongoing) • PSMA PET’s accuracy could be utilised for radiopharmaceutical treatment as well, e. g. 177 Lutetium
Future directions • Data on PSMA PET’s impact on patient outcome remains years away • Prospective studies needed • Meanwhile centres using PSMA PET should report their experience to help determine its optimal role in prostate cancer
First do no harm • With MRI for diagnosis and PSMA PET for staging, we are finally on our way to maximising cure while minimising harm in prostate cancer
Acknowledgments • Prof Boris Hadaschik – Heidelberg, Germany • A/Prof Declan Murphy – Peter Mac • A/Prof Nathan Lawrentschuk – Peter Mac • Dr Martin Cherk – Alfred • Dr Paul Beech – Alfred • Prof Mark Frydenberg – AUA • Mr Daniel Moon – AUA • Mr Ross Snow – AUA • Mr Uri Hanegbi – AUA • Mr Adam Landau – AUA • Dr Lana Pepdjonovic – AUA Research Fellow
Thank you