The Role of Microbiology Laboratory Improving the laboratory

The Role of Microbiology Laboratory Improving the laboratory diagnosis of Infectious Disease Gunturu Revathi Aga Khan University Hospital Nairobi KPA Pre Congress Symposium Infectious Diseases 9 th April 2019 White sands, Mombasa








Antimicrobial usage in humans, animals and agriculture, and resulting dispersion of antimicrobial residues into aquatic and terrestrial environments (Berkner et al. , 2014)

Complex problem

Some preventable infections are more preventable than others




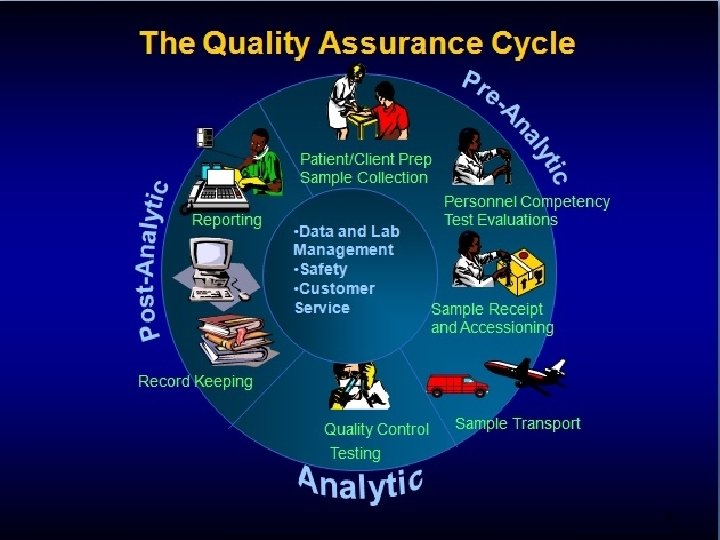
The quality of health services is founded on a good education and training and continued maintenance of such competencies

Role of Microbiology Lab 1. Diagnostic lab work 2. Advice to clinicians - treatment of infected patients 3. Infection control 4. Surveillance of Infectious diseases Close personal contact with clinicians in daily treatment of patients ensures rational AM use

ASP: Antimicrobial Stewardship Program; DSP: Diagnostic Stewardship Program; ISP: Infection Prevention Stewardship Program.

Scope of infection control Offices Shops Factories Hotels Eateries Farms Agricultural Poultry Diary farms Community Hospital Special settings Schools Colleges Day care centers Hostels Play grounds Churches Temples


Factory of Superbugs

Human microbiome research has shown that the use of antibiotics can disrupt the normal array of microbes that live in and on our bodies. Suspected etiology for Childhood Obesity Autoimmune conditions Chronic inflammatory conditions

HOSPITAL MICROBIOME A new hypothesis says that hospitalacquired infections are being driven not only by the existence of harmful microbes but also by the absence of helpful species in the environment due to disinfectant use


I AM CONCERNED ABOUT THE HIGH LAVELS OF BLOOD WE FOUND IN YOUR BLOOD TEST

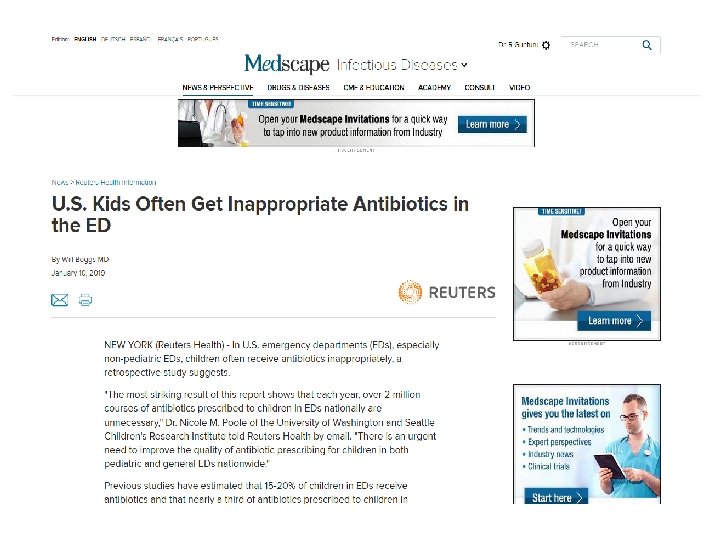
Optimal laboratory test utilization is. important for Providing high quality clinical care and Efficiently using limited health care resources • Microbiologists - the earliest advocates for the appropriate use of laboratory studies • There is an urgent need for laboratory leaders to partner with clinical colleagues to implement effective laboratory testing stewardship protocols.
 with an ability to support computerized")
Recent widespread adoption of electronic medical records (EMRs) with an ability to support computerized provider order entry (CPOE) and CDSTs has provided effective new avenues for implementation of sustainable automated test utilization programs in developed countries.

COST SAVING MEASURES Unnecessary and wasteful practices • Routine – Microbiological Swabbing of environment – Disinfectants for environmental cleaning e. g. floors & walls – Fumigation of isolation room with formaldehyde • Unnecessary – Use of overshoes and dust attracting matt – Personal Protective Equipment in the Intensive Care, & Neonatal Unit • Excessive/unnecessary use of – IM/IV injections – Insertion of indwelling devices e. g. IV lines, urinary catheters, nasogastric tube – Antibiotics both for prophylaxis and treatment Damani NN. Journal of Hospital infection 2007; 65(S 1): 151 -154.

The critical nature of the microbiology laboratory in infectious disease diagnosis calls for a close, positive working relationship between the physician/advanced practice provider and the microbiologists who provide enormous value to the healthcare team.

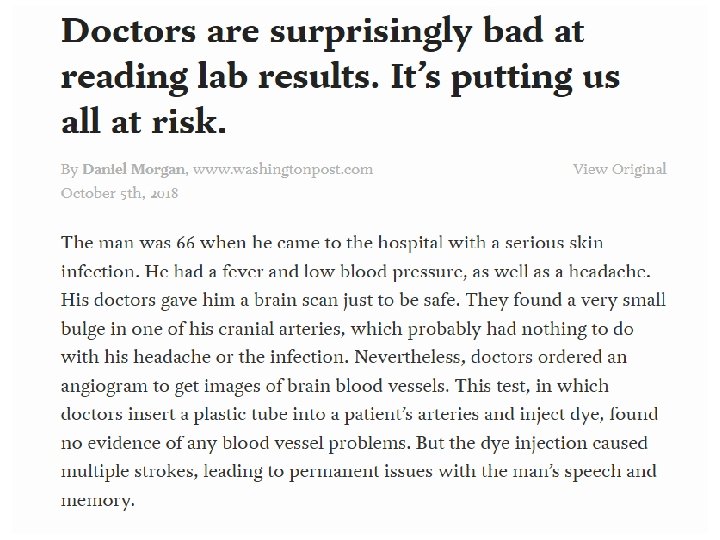
Unlike other areas of the diagnostic laboratory, clinical microbiology is a science of interpretive judgment that is becoming more and more complex,
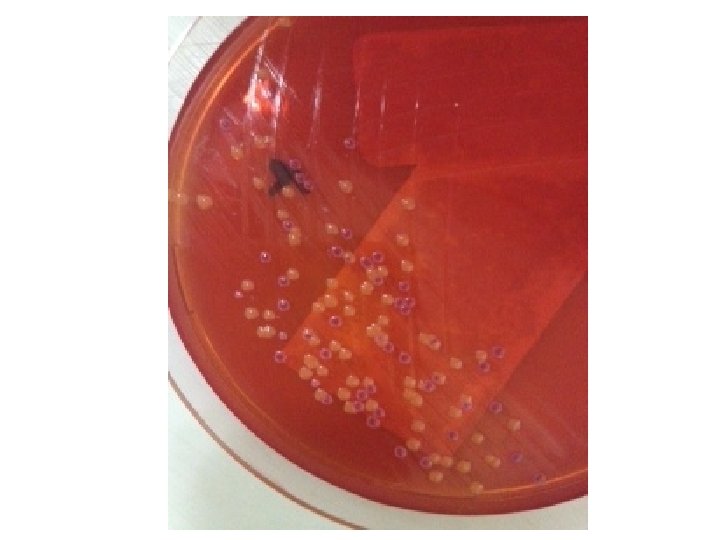

HEAVY MIXED GROWTH OF THREE TYPES OF COLONIES

At an elementary level, the physician needs answers to 3 very basic questions from the laboratory: Is my patient’s illness caused by a microbe? If so, what is it? What is the susceptibility profile of the organism so therapy can be targeted?

To meet those needs, the laboratory requires a specimen that has been appropriately selected, collected, and transported to the laboratory for analysis

Caught in the middle, between the physician and laboratory requirements, are the medical personnel who actually select and collect the specimen and who may not know or understand what the physician or the laboratory needs to do their work

Enhancing the quality of the specimen is everyone’s job, so communication between the physicians, nurses, and laboratory staff should be encouraged and open with no punitive motive or consequences

The diagnosis of infectious disease is best achieved by applying in-depth knowledge of both medical and laboratory science along with principles of epidemiology and pharmacokinetics of antibiotics and by integrating a strategic view of host–parasite interactions.

One of the most valuable laboratory partners in infectious disease diagnosis is the certified clinical microbiology specialist Clinicians should recommend and medical institutions should provide this kind of leadership for the microbiology laboratory or provide formal access to this level of laboratory expertise through consultation.

Clearly, the best outcomes for patients are the result of strong partnerships between the clinician and the microbiology specialist

TEN POINTS OF IMPORTANCE 1. Specimens of poor quality must be rejected 2. Physicians should not demand that the laboratory report“everything that grows 3. Background noise” of commensal microbiota 4. The laboratory requires a specimen, not a swab of a specimen.

Swabs are expected from the nasopharynx and to diagnose most viral respiratory infections Flocked swabs have become a valuable tool for specimen collection 5. The laboratory must follow its procedure manual or face legal challenges The procedures in the manuals should be supported by the literature, especially evidence-based literature. To request the laboratory to provide testing apart from the procedure manual places everyone at legal risk. 6. A specimen should be collected prior to administration of Antibiotics 7. Susceptibility testing should be done only on clinically significant isolates, not on all microorganisms recovered in culture.

8. Microbiology laboratory results that are reported should be accurate, significant, and clinically relevant. 9. The laboratory should set technical policy; this is not the purview of the medical staff. Good communication and mutual respect will lead to collaborative policies. 10. Specimens must be labeled accurately and completely so that interpretation of results will be reliable. Labels such as eye” and “wound” are not helpful to the interpretation of results without more specific site and clinical information (eg, dog bite wound right forefinger).


This is not an official guideline of the IDSA but rather an authoritative guide with recommendations for utilizing the microbiology laboratory in infectious disease diagnosis.

It is a collaborative effort between clinicians and laboratory experts focusing on optimum use of the laboratory for positive patient outcomes. When the term “recommended” is used in this document, it is not a “graded” recommendation as would be found in a guideline, but rather the preferred or indicated approach for

Clean Hands are Safe Hands Thank you for your kind attention! !
- Slides: 60