THE ROLE OF INTRAOPERATIVE PARATHYROID HORMONE ASSAY IN
















 + Test turn around")
 + Timing (preincisional, preexcision, 5 min, 10 min +/-")













 21 (2. 9%) 702 (97. 1%) Successful Failed 16(2. 3%)")

 conventional approach +")



- Slides: 42
THE ROLE OF INTRAOPERATIVE PARATHYROID HORMONE ASSAY IN FOCUSED PARATHYROIDECTOMY Ian Wong Queen Mary Hospital
1849 The glands of Owen – “last major organ to be recognized” J R Soc Med. 2004 October; 97(10): 494– 495.
AGENDA + Conventional vs Focused approach + Focused parathyroidectomy + Intraoperative PTH assay + Selective approach + Importance of an experienced surgeon
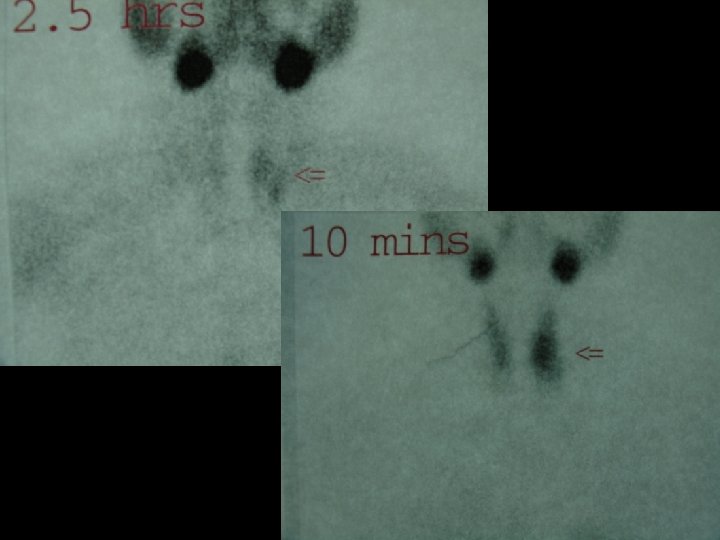
CONVENTIONAL VS FOCUSED + Conventional - bilateral neck exploration – Identify all parathyroid glands – Excision of all abnormal glands + Focused parathyroidectomy – Primary hyperparathyroidism: 90% adenoma – Preoperative imaging: Sestamibi, Surgeon performed ultrasound (94 -99% sensitive in concordant scans) – Intraoperative parathyroid hormone assay (PTH) Endo Prac. Volume 17, Supp 1 , March-April 2011 Pg 75 -82
CONVENTIONAL VS FOCUSED + Benefits: – Cosmetic – Postoperative pain – Shorter operating time – Ambulatory surgery – Lower risk of recurrent laryngeal nerve injury – Decrease postoperative hypocalcaemia Endo Prac. Volume 17, Supp 1 , March-April 2011 Pg 75 -82
CONVENTIONAL VS FOCUSED Minimally invasive Conventional P-value parathyroidectomy bilateral neck exploration Cure Rate 99. 4% 97. 1% P <0. 001 Complication Rate 1. 45% 3. 10% P=0. 02 Annals of Surgery Volume 253, Number 3, March 2011
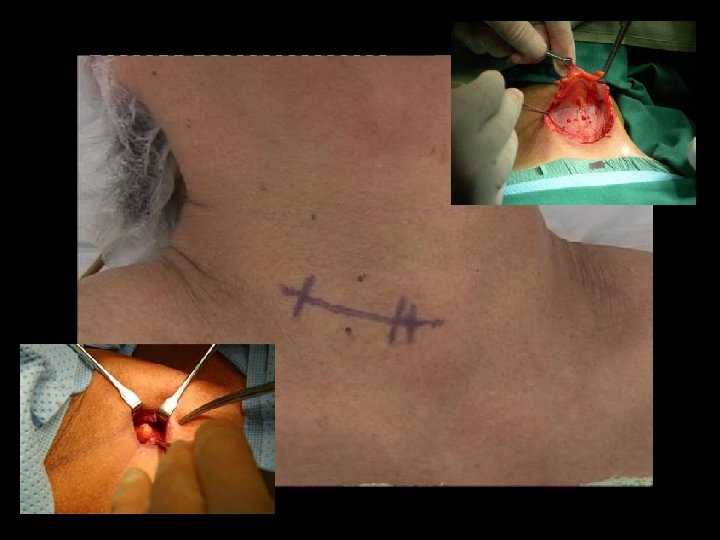
FOCUSED PARATHYROIDECTOMY
INTRAOPERATIVE PARATHYROID HORMONE ASSAY
INTRAOPERATIVE PTH + Mechanism, physiology + Protocol + Pitfalls + Other roles + Selective approach to intraoperative PTH >50% general surgeons; >90% endocrine surgeons in US adopt intraoperative PTH monitoring J Am Coll Surg. 2009 Sep; 209(3): 332 -43.
MECHANISM & PHYSIOLOGY + Short half life (3 -5 min) + Test turn around time: 8 -20 minutes + Antibodies: sandwich complex technique Endo Prac. Volume 17, Supp 1 , March-April 2011. Pg 44 -53
PROTOCOLS + Venous access (jugular/peripheral) + Timing (preincisional, preexcision, 5 min, 10 min +/- 20 min) + Interpretation – Miami criteria (>50% PTH drop in 10 min) – Charleston criteria (>50% PTH drop and return to normal in 20 min) Accuracy (sensitivity 97%, specificity 98%) ü Decrease false positive from 0. 9% to 0. 3% ü Surgery. 2003 Dec; 134(6): 973 -9; discussion 979 -81. Endo Prac. Volume 17, Supp 1 , March-April 2011. Pg 44 -53
PITFALLS + Collection site – Jugular veins: higher absolute PTH, longer to reach normal or significant level + Renal Dysfunction: – lesser/slower degree of PTH drop + Laboratory error + Haemolysis + Timing of blood sampling – PTH hormone dynamic Endo Prac. Volume 17, Supp 1 , March-April 2011. Pg 44 -53
PITFALLS Endo Prac. Volume 17, Supp 1 , March-April 2011. Pg 44 -53
PITFALLS Endo Prac. Volume 17, Supp 1 , March-April 2011. Pg 44 -53
PITFALLS Endo Prac. Volume 17, Supp 1 , March-April 2011. Pg 44 -53
PITFALLS Endo Prac. Volume 17, Supp 1 , March-April 2011. Pg 44 -53
ROLES + Confirm complete excision + Additional hypersecreting tissue + Differentiating parathyroid from non parathyroid tissues + ? Identifying the side of neck with hypersecreting parathyroid gland (differential jugular venous sampling)
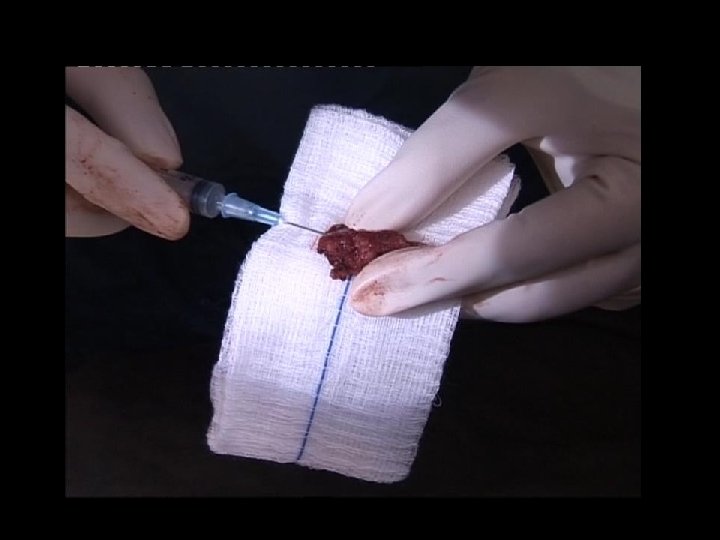
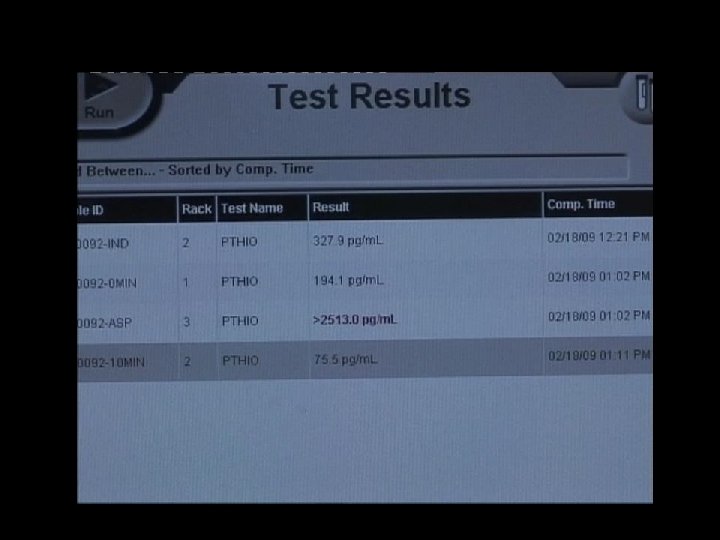
CONFIRMATION OF PARATHYROID GLAND + Biochemical fine needle aspiration – Differentiate parathyroid gland – PTH levels in tissue sample – Rapid assay value > 1500 pg/ml – Specificity 100% World J Surg. 2000 Nov; 24(11): 1319 -22.
INTERNAL JUGULAR VENOUS SAMPLING + Differential internal jugular venous sampling – ? 10% higher PTH in hypersecreting side in 70 -80% – ? Useful in negative or equivocal preoperative localization Group A: Negative sestamibi scan undergoing bilateral neck exploration Group B: Positve Sestamibi scan undergoing focused parathyroidectomy World J Surg (2010) 34: 1299– 1303
SELECTIVE APPROACH TO INTRAOPERATIVE PTH
SELECTIVE APPROACH TO INTRAOPERATIVE PTH + Add little value in selected group – Changed operative management 74% of imaging discordant group Ø 2% of imaging concordant group Ø + Cost; Operation time + False negative in selected groups – Unnecessary conversions Surgery. 2008 Aug; 144(2): 299 -306.
SELECTIVE APPROACH TO INTRAOPERATIVE PTH Ann Surg 2010; 251: 1122– 1126
RECOMMENDATION + Intraoperative PTH add little value + Concordant “MIBI” and Ultrasound scan + Intraoperative PTH recommended + Single preoperative localization imaging + Discordant “MIBI” and Ultrasound scan + Reoperative surgery Recommendation Level Ib-III, Grade A/B Langenbecks Arch Surg (2009) 394: 799– 809
IMPORTANCE OF AN EXPERIENCED SURGEON
723 (FU >6 months) 21 (2. 9%) 702 (97. 1%) Successful Failed 16(2. 3%) Successful localization in subsequent operation 5(0. 7%) Intraoperative PTH False Negative
1849 The glands of Owen - last major organ to be recognized” J R Soc Med. 2004 October; 97(10): 494– 495.
CONCLUSION + Focused parathyroidectomy is comparable to (if not superior than) conventional approach + Practitioners need to understand the roles and interpretation of intraoperative PTH + Cost effectiveness of intraoperative PTH in selected groups is debatable + Surgeons’ experience is very important
THANK YOU
O Results Complication rate 0. 4% Conversion rate 3. 9 % Overall success rate 98. 6% IPM sensitivity 99. 6% IPM accuracy 92. 9% Operative time (34 vs 60 mins) P<0. 001 Ann Surg 2010; 251: 1122– 1126
+ Bayes' theorem shows how to determine inverse probabilities: – knowing the conditional probability of B given A, what is the conditional probability of A given B?