THE ROLE ANATOMY PHYSIOLOGY BIOMECHANICS OF THE SPINE

THE ROLE ANATOMY, PHYSIOLOGY, BIOMECHANICS OF THE SPINE IN THE MANAGEMENT OF SPINAL DISORSERS

Introduction : Anatomy, physiology & spine biomechanics are basic science in among medical science Understanding of spinal anatomy physiology & spine biomechanics are crucial for a comprehensive evaluation of a patient with spinal disorders (Moore, 1999, An 1998, Frymoyer 2001, Rothman 1999, Hoppenfeld et al 1994) Nowadays in modern era of spine management basic science is still useful Exp : - Scoliosis surgery using pedicles- screw instrumentation - Minimal Invasive Surgery (MIS) 2

Anatomy, physiology, spine biomechanics and its application : The primary roles of the spine are: Maintaining stability Protecting neural element Allowing range of motion (mobility) Transmitting upper and lower extremity movement The vertebral column are consist of: 33 vertebra were divided by: 7 cervical 12 thoracic 5 lumbar 5 sacral 4 coccygeal 3

Ad/ cervival vertebra 7 cervical vertebral were divided 2 type : typical C 3 -C 4 -C 5 -C 6 atypical vertebral C 1/C 2 - C 7 4

Ad/ Typical vertebra C 1 -C 2 complex C 1= atlas C 2= axis =epistropheus C 1 = Atlas Lack of body and spinous process Consist of four ring structure + lateral mass Steel’s rule 3 rd: Anterior 3 rd – odontoid process Middle 3 rd – spinal cord Posterior 3 rd – epidural fat Articulation C 1 - Occiput atlanto - occipital Articulation C 1 -C 2 atlanto-axial 5

C 2 = axis epistropheus C 2 are consist of: Odontoid process/ body projection of C 2 Spinal process-bifid C 1 -C 2 articulation C 2 -C 3 articulation Typical vertebra C 3/C 4/C 5/C 6 Middle cervical segment are comprised with: Vertebral body –anterior part Vertebral arch –posterior part Lateral mass – facet joint (zygoapophyseal joint) Spinous process – bifid Joint of Luschka (uncovertebral joint) C 6 - Chassaignac’s tubercle - anterior tubercle - carotid tubercle 6

• C 7 prominent cervical vertebra Large spinal process Bifid single of spinous process same as thoracic Facet (t) same as cervical = lateral mass Cervical vertebra was suspended by ligaments Anterior longitudinal ligament Posterior longitudinal ligament Flavum ligament Interspinous ligament Supraspinous ligament Ligament to hold C 1 -C 2 Apical ligament Alar ligament Anterior atlanto - axial ligament Posterior atlanto - axial ligament Transverse ligament cruciform ligament 7
 Thoracicvertebra. Were divided by typical vertebra T 2 -T 9 typical")
Ad/ thoracic F) Thoracicvertebra. Were divided by typical vertebra T 2 -T 9 typical vertebra T 1/T 10/Th 12 Vertebral body (anterior) Vertebral arch (posterior) Supported by 7 process 1 spinous process 2 transverse process 2 superior facet 2 inferior facet Vertebral body Heart shaped (cross -section) Posterir vertebral height > anterior height kyphosis Which consist of : Costo vertebral articulation Costo transverse articulation 8
 - very prominent")
Ad/atypical vertebra T 1 - resembles with cervical vertebra (vertebral body) - very prominent of spinous process (largest than C 7) 1 st rib articulate with T 1 vertebral body VIA COSTAL FACET Process uncinate => uncovertebral joint Superior vertebral notch => connect with T 2 T 10 –TXI – TXII Costo transverse articulation (-) Rib articulate -> vertebral body – don’t over Lie the disc space Vertebral body resembles with lumbar body (kidney shaped) Facet transition thoracic lumbar 9

How to determined anatomy of pedicles thoracic vertebral ? Vertebra thoracic pedicles posterior –superior direction S – I > M-L T 4 pedicle narrowest (width) compared with A/B level Medial wall 2 -3 times thicker Medial angulation –decreased T 1 -Th. XII Entry point of P. S, facet joint intersect with transverse process varies slighthy 10

How to determined level of vertebral ? 1 st Rib – attached 2 nd Rib – attached 3 rd Rib – attached T 10 – TII – Rib Space to VB T 1 to VB T 2 and T 3 (overlie T 2 & T 3 ) attached to VB don’t cross to disk How to determined level of vertebral ? Thoracic facet joint oriented: 600 sagittal plane 200 cervical plane Vertebra thoracic vertebra stable (they were holding by Rib) 11

Ad/ Lumbar vertebra Typical lumbar vertebra VB – kidney shaped Diameter AP < Transverse VB was divided by 2 part : A & B a) - superior facet - transverse process - pedicle b) - lamina - inferior facet - spinous process Pedicle orientation Connect posterior element to vertebral body (Lamina, transverse process, facets) Width = L 5 = 18 mm L 1 = 9 mm L 1 –L 5 horizontal ± 1, 5 cm L 1 –L 5 vertical ± 1, 5 cm Slight medial inclination L 1= 120 , L 5 = 300 12

Ad/ sacrum Sacrum – triangular shaped Fused – 5 vertebra Anterior – superior promontory vertebra body S 1 Lateral – ala sacrum process transverse of ST Sacral Crest median fused ST 4 sacral vertebra Sacral Cornu pedicles S 5 – landmark of sacral hiatus Sacral hiatus – Opening at dorsal site of sacrum - S 4/S 5 sacral lamina absence Ad/ coccyx • Coccyx – triangle shaped • Fused coccyx 3/4/5 vertebra

Anatomic structure provide articulation L-L, L-S VB articulation ALL PLL Disk Posterior Element articulation Articular capsules flavum ligament Supra spinous ligament Intertransverse ligament L-S articulation Upper lumbar ligament Lumbar sacral ligament

Vascular structure cervical vertebra : Major blood supply – Vertebral artery V. atery – branch of subclavian artery Anterior C 7 – entry C 6 - exit C 1 – Foramen magnum – Basilar artery Feeding spinal cord, vertebra, n root Vertebra artery – branch – anterior spinal artery 60% spinal cord anterior Posterior spiral artery 30 % spinal cord posterior Lower portion of spinal cord was feeding by radicular artery branch of : V. Artery A. Cervical Artery Deep Cervical Artery Radicular artery vertebral artery anterior radicular artery + posterior radicular artery Thoracic Artery 1. 2. 3. Radicular artery – feed superior middle thoracic Branch of posterior intercostal artery Branch of radicular artery – anastomose with anterior spinal artery – feeding spinal cord

Thoracic Lumbar artery Great anterior radicular arteri = Arteria radicularis Magna = Adamkiwiecz artery 85% Left side intercostal artery – Intervertebral foramina T 9 – T 12 Superior lumbar artery – spinal canal – mean artery supply 2/3 anterior cord inferior 1. 2. 3. Sacral artery • Internal Iliac artery – lateral sacral artery Venous drainage 1. 2. 3. 4. Anterior spinal vein + posterior spinal vein Radicular vein Intercostal vein Batson’s plexus = Basivertebral vein

Special Condition were correlated with anatomy T 4 - T 9 – spinal canal narrowest – has the least profuse blood supply = vascular zone of the spinal cord. critical The region where the zone meet posterior spinal artery and anterior spinal artery – blood supply is poor = watershed region v Dissection in the region of intervertebral foramen and costo transverse joint should be limited , electrocautery should not be use in the area.

Biomechanic Of The Spine Definition Biomechanic : is study about mechanism activity of locomotion Locomotion = Locomotorius system = muskuloskeletal = Axial + Non Axial = Spine Biomechanic of spine : Is study mechanism activity of the spine Biomechanics Of Spine And Its Application Principle of spine biomechanics Biomechanics of the spine in the trauma management Biomechanics of the spine in the instrumentation

Ad/ Principle spine biomechanics FSU part of spinal column had affinity move/coupling unit FSU are consist of: Intervertebral disk Adjacent bodies Facet joints ligaments Spinal stability Under physiologic loading There is neither abnormal strain no excessive motion In the FSU In which neurologic structure are protected

Spinal stability are comprised 3 components: Physiologic load Integrity of spinal collumn Neurologic status Physiologic load normal limit can be resorbed and absorbed transmitted physiologically by disk and posterior element Integrity of spinal collumn no previous injury and disorders to the spinal collumn, et all Neurologic status intact

Segment vertebra Anterior collumn are consist of: Anterior longitudinal ligament Vertebral body Disk Posterior longitudinal ligament 80 % axial load come and through this part Compressive site Posterior collumn are consist of: Lamina Facets Osseus ligamentum complex posterior Tension site 20% axial load through this site Statement : The motion segment (FSU) is the smallest unit & it responsible for over all spinal function.

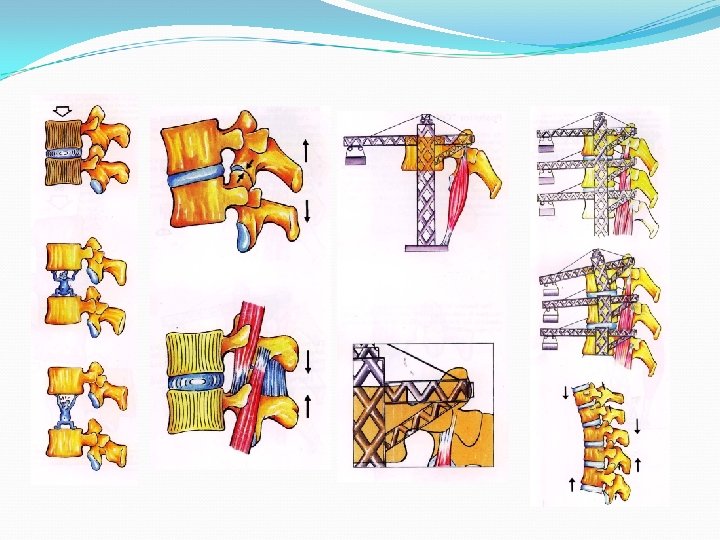
Spinal Collumn & FSU = analog with crane = Gravity of body/ centre line of gravity anterior to the tower of the crane anterior to the vertebral body or disk Odontoid S 1 Axial load is distribute as an axial compression load & bending moment Load sharing capacity = Anterior Collumn = 80% (absorbed 80%) principle = Posterior Collumn = 20% Compressiom force = 80% which resorbed/absorbed by : Disk – material & structural of Disk (AF & NP) ALL PLL VB Tensile force = 20% which hold by : Muscle action Facet joint/fulcrum of muscle action (Impedance)
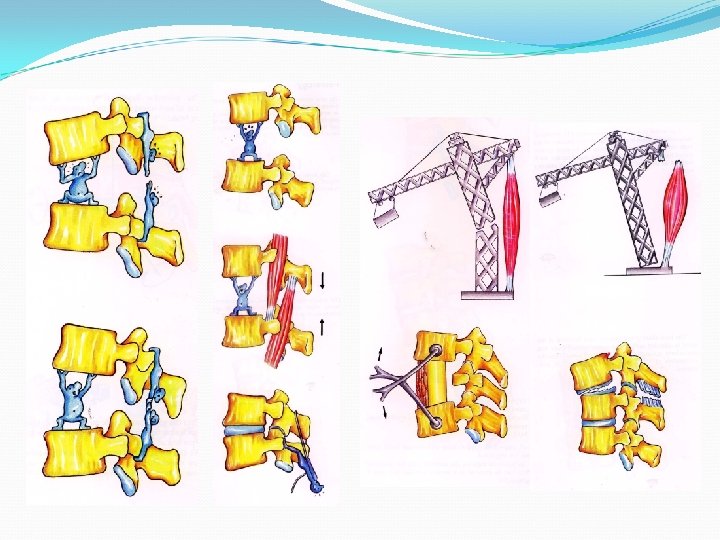
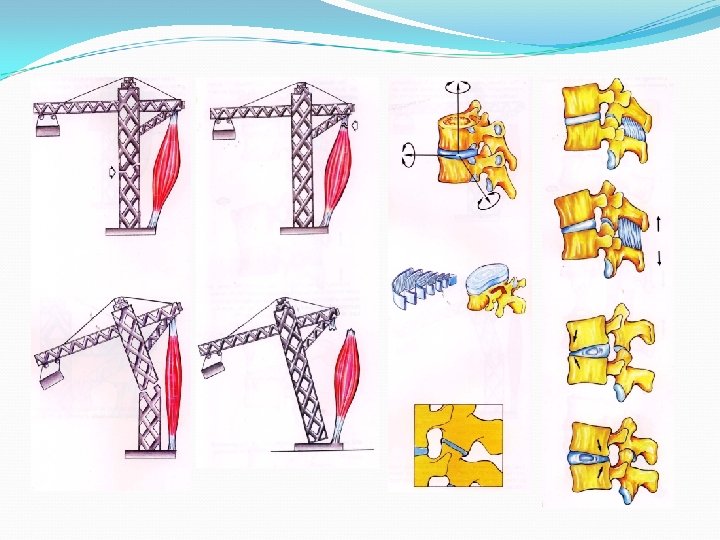

Biomechanical relationship between anterior collumn and posterior collumn 1. 2. 3. Anterior collumn is compression site Posterior collumn is tension site Anterior collumn are consist of: 4. Disk Vertebral body Anterior longitudinal ligament posterior longitudinal ligament Posterior collumn are consist of: Facet joint complex Lamina Flavum Process spinous + supra spinous + interspinous ligament Intertransverse ligament

Compression force was act by - Disk Lord carrying capacity - Vertebral body 80% - ALL principle - PLL 6. Tensile force was act by 20% - Osseous ligamentum complex posterior - Tension band principle 7. Tensile force (+) act if anterior collumn intact 8. Tension band principle (+) act if anterior collumn intact 9. TBP (+) act anterior collumn broken/damage restored 1 ST 10. TBP (+) act if tensile force (+) Osseous ligamentum complex (+) intact if tensile force (-) Osseous damage restored 5.

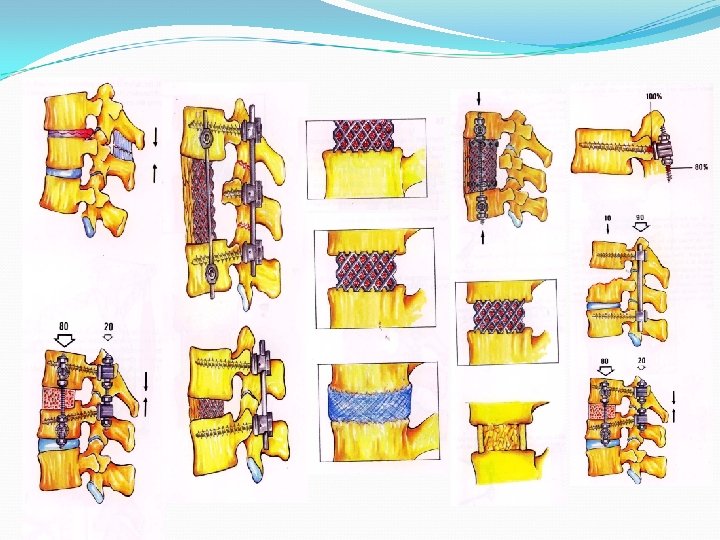
Biomechanic of Spinal Recontruction 1. Anterior collumn damage/broken 1 ST reconstruction aterior ( anterior collumn intact) 2. 3. Anterior – should be followed by posterior Osseous ligamentum complex posterior broken + anterior collumn intact Suggested stabilization / reconstruction Probable reconstruction 4. Anterior collumn + posterior collumn broken Possible reconstruction Middle collum is part of anterior collumn stabilizer Broken middle collumn – reconstruction ? - stable – no reconstruction (stable? ) - unstable - reconstruction

7. Reconstruction – short segment - long segment Indicator short segment : - Instruments – stronger - V. segment – stronger pedicle screw - Compression fx PSSW 8. - Degenerative stenosis - Spondylolisthesis Indicator long segment : - Instrumentation – less stronger - V. segments – integrity need > segment vertebra fixed reconstruction good enough Deformity need reconstruction kyphosis : - Trauma - Infection Anterior collumn deficiency - Tumor - Vertebral osteoporotic fx

9. Last but not least spinal reconstruction closed with spinal biomechanics aim of these : - Provide stability - Provide mobility - Protected spinal cord - Transmitted movement + to upper extremity & lower extremely Summary 1. Have been presented anatomy, physiology, and spine biomechanics. 2. Study anatomy, physiology, and spine biomechanics to give understand spinal disorder 3. Understanding spinal disorder are crucial for a comprehensive diagnosis and treatment to give optimal result and less complication. Thank you for your attention 31
- Slides: 31