The rationale for monitoring the fetal heart rate
 is that FHR patterns are")


 monitoring")

















, based on their extensive review, proposed adoption of a strict")


. �The sinusoidal pattern has been reported")




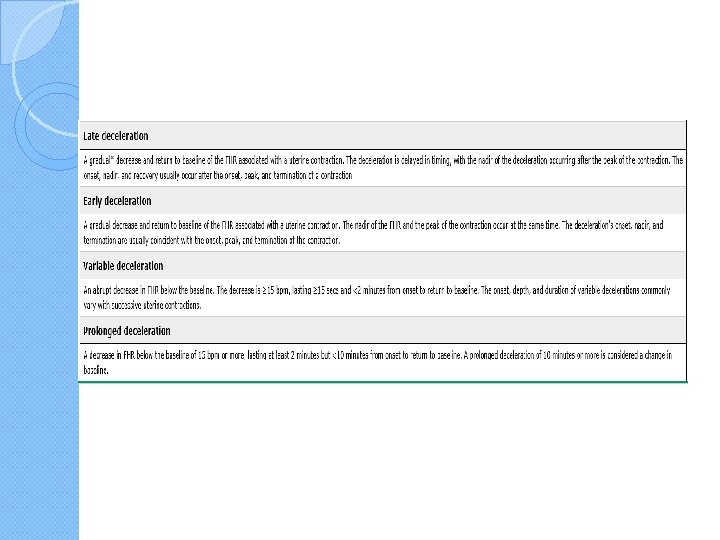
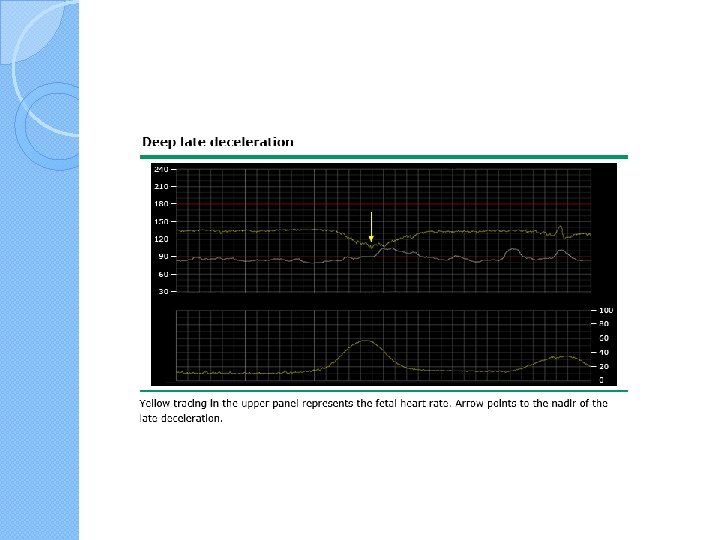
: � • Recurrent late decelerations")
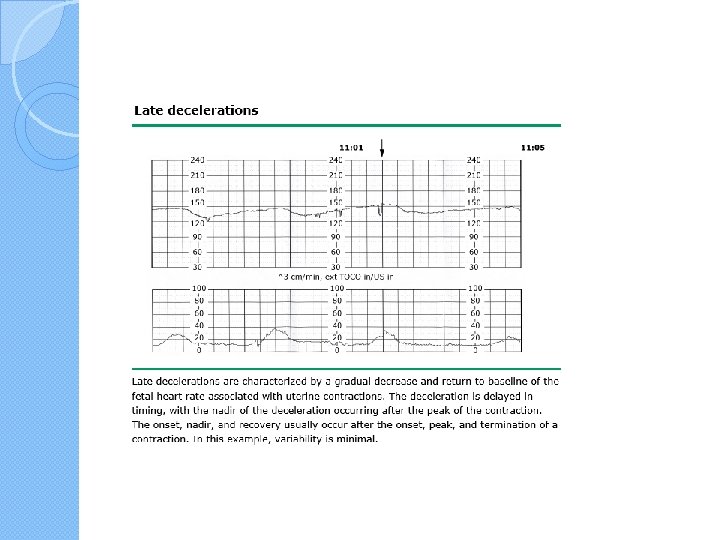




, slow return to")







- Slides: 60
�The rationale for monitoring the fetal heart rate (FHR) is that FHR patterns are indirect markers of the fetal cardiac and medullary responses to blood volume changes, acidemia, and hypoxemia, since the brain modulates heart rate
�The lack of a correlation between use of intrapartum monitoring and improvement in neurologic outcome is likely related to the observation that most FHR abnormalities are not associated with fetal acidosis or hypoxemia and most fetal acidosis and hypoxemia does not result in neurologic disability.
� 99. 8 percent of nonreassuring FHR tracings are not associated with development of cerebral palsy �the degree of hypoxemia and acidosis that leads to long-term neurologic damage is close to that causing fetal death, thus most severely depressed term fetuses either survive intact or die, rather than survive disabled
EVALUATION OF THE FETAL HEART RATE �Continuous intrapartum electronic fetal heart rate (FHR) monitoring is generally recommended for pregnancies that are at least 23 weeks of gestation
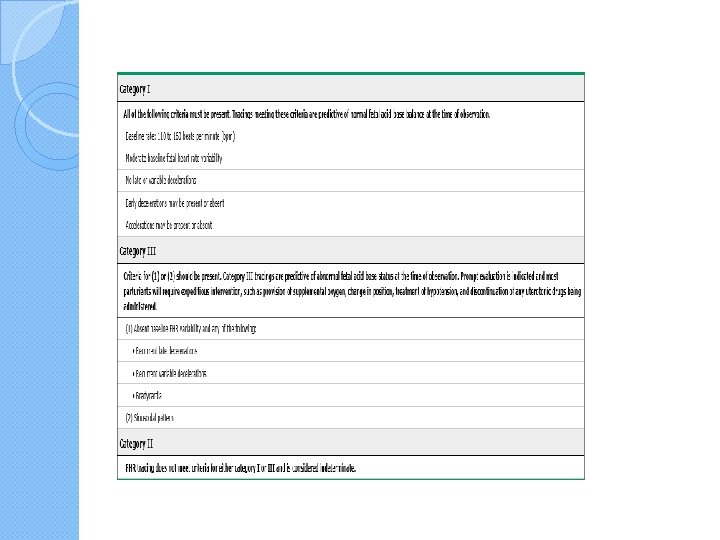
�The NICHD subsequently created a three-tier FHR interpretation system, in which �category I represents a normal tracing (predictive of normal fetal acid-base balance at the time of observation) �category II represents an indeterminate tracing, �category III represents an abnormal tracing (predictive of a significant incidence of abnormal fetal acid-base status at the time of observation)
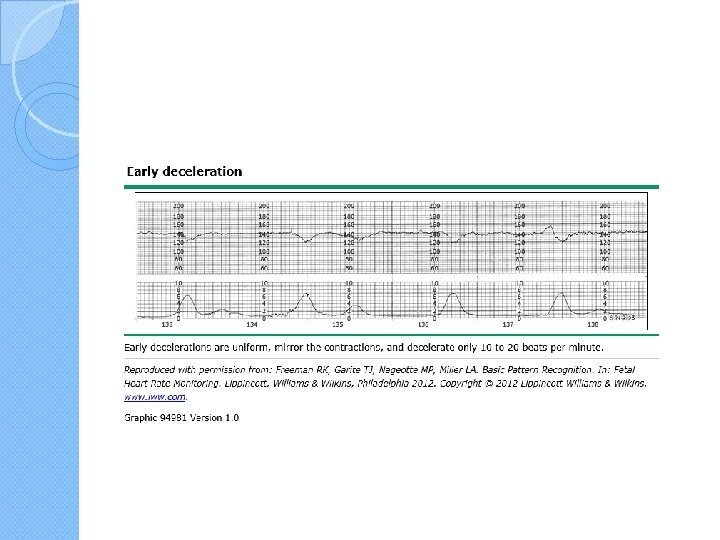
Category I tracings The presence of a category I tracing is reassuring as it indicates there is minimal likelihood of acidemia at that point in time; it is not predictive of future status, as tracing patterns can change. A category I tracing has all of the following components �●A baseline fetal heart rate of 110 to 160 bpm �●Absence of late or variable FHR decelerations �●Moderate FHR variability (6 to 25 bpm) �●Early decelerations and accelerations may be present or absent
�FHR accelerations are an important finding when present because their presence, especially in the presence of moderate variability, almost always indicates that the fetus is not acidotic
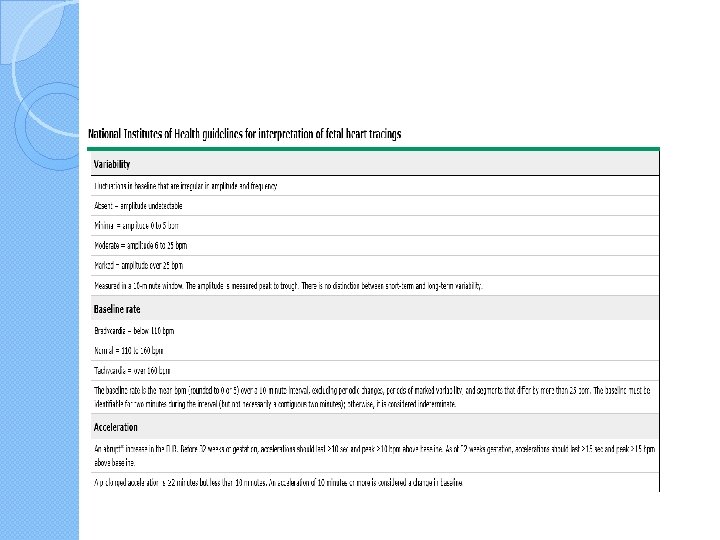
Decreased Variability. �Diminished beat-to-beat variability can be an ominous sign indicating a seriously compromised fetus �mean fetal scalp p. H of approximately 7. 10 was found when severe decelerations were combined with 5 bpm or less variability, compared with a p. H of approximately 7. 20 when greater variability was associated with similarly severe decelerations. �Severe maternal acidemia also can cause decreased fetal beat-to-beat
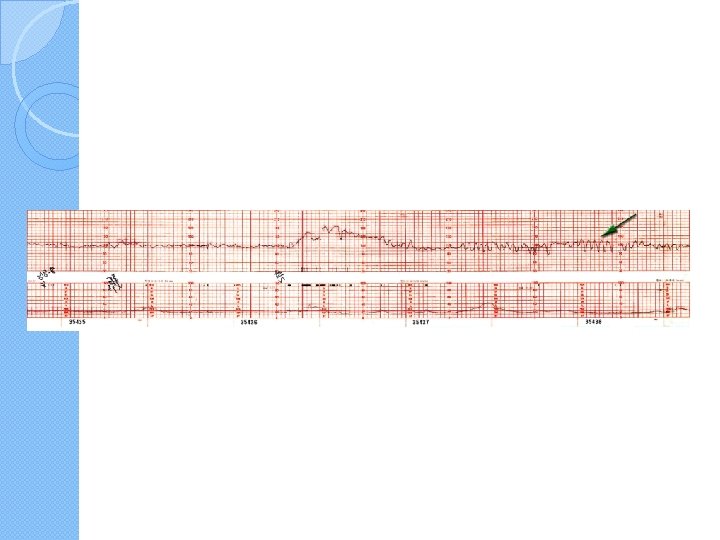
External fetal heart recording showing lack of long-term variability at 31 weeks during maternal diabetic ketoacidosis (p. H 7. 09).
Recovery of fetal long-term variability after correction of maternal acidemia.
A common cause of diminished beat-to-beat variability is administration of analgesic drugs during labor � Various central nervous system depressant drugs can cause transient diminished beat-to-beat variability. Included are narcotics, barbiturates, phenothiazines, tranquilizers, and general anesthetics. � Variability regularly diminishes within 5 to 10 minutes following intravenous meperidine administration, and the effects may last up to 60 minutes or longer depending on the dosage given � Butorphanol given intravenously diminishes fetal heart � rate reactivity � In a study performed at Parkland Hospital, Hill and colleagues � (2003) found that 5 bpm or less variability occurred in 30 percent of women given continuous intravenous meperidine compared with 7 percent in those given continuous labor epidural analgesia �
�Magnesium sulfate, for tocolysis as well as management of hypertensive women, has been arguably associated with diminished beat-to-beat variability. �Magnesium sulfate was associated with statistically decreased variability only in the third hour of the infusion. �the mean variability was 2. 7 bpm in the third hour of magnesium infusion compared with 2. 8 bpm at baseline. �Magnesium sulfate also blunted the frequency of accelerations.
�It is generally believed that reduced baseline heart rate variability is the single most reliable sign of fetal compromise. �variability by itself could not be used as the only indicator of fetal well-being.
�beat-to-beat variability is affected by various pathological and physiological mechanisms. �A persistently flat fetal heart rate baseline—absent variability—within the normal baseline rate range and without decelerations may reflect a previous insult to the fetus that has resulted in neurological damage
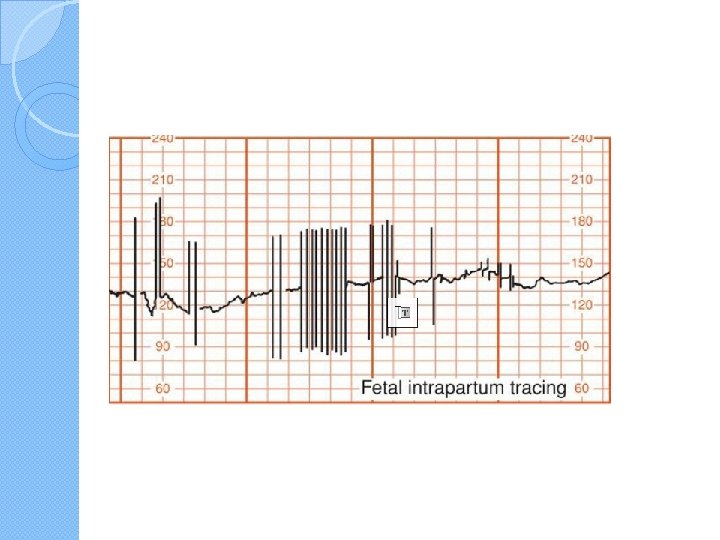
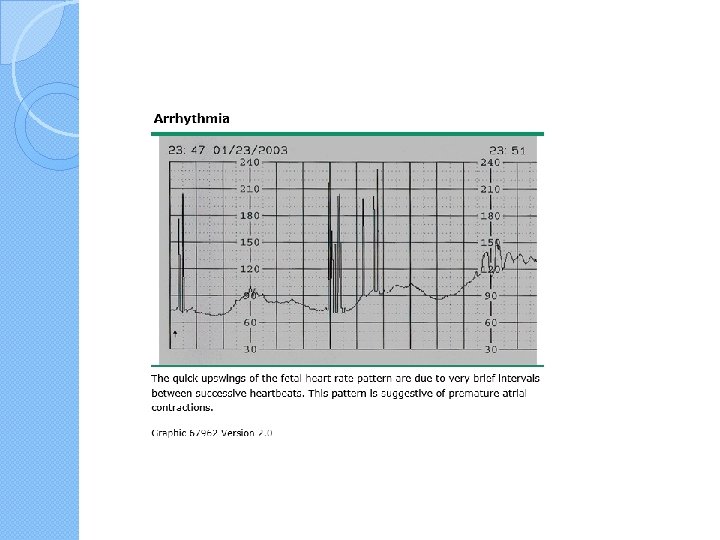
Cardiac Arrhythmia �When fetal cardiac arrhythmias are first suspected using electronic monitoring, findings can include baseline bradycardia, tachycardia, or most commonly in our experience, abrupt baseline spiking
�Intermittent baseline bradycardia is frequently due to congenital heart block. �conduction defects, most commonly complete atrioventricular (AV) block, usually are found in association with maternal connective-tissue diseases. � Some fetal monitors can be adapted to output the scalp electrode signals into an electrocardiographic recorder. Because only a single lead is obtained, analysis and interpretation of rhythm and rate disturbances are severely limited.
�Arrhythmias, episodes of bradycardia < 100 bpm, or tachycardia > 180 bpm were encountered in 3 percent. �Most supraventricular arrhythmias are of little significance during labor unless there is coexistent heart failure as evidenced by fetal hydrops. �Many supra-ventricular arrhythmias disappear in the immediate neonatal period, although some are associated with structural cardiac defects
�Sonographic evaluation of fetal anatomy and echocardiography may be useful. �Some clinicians use fetal scalp sampling as an adjunct. Generally, in the absence of fetal hydrops, neonatal outcome is not measurably improved by pregnancy intervention. � At Parkland Hospital, intrapartum fetal cardiac arrhythmias, especially those associate with clear amnionic fluid, are managed conservatively.
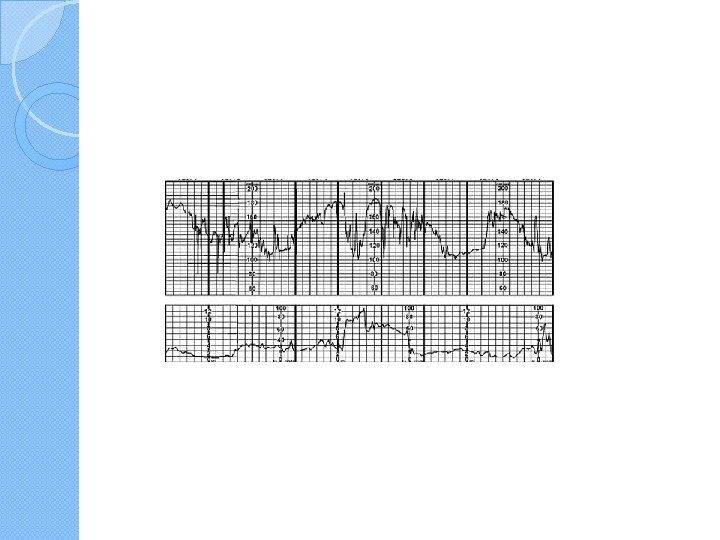
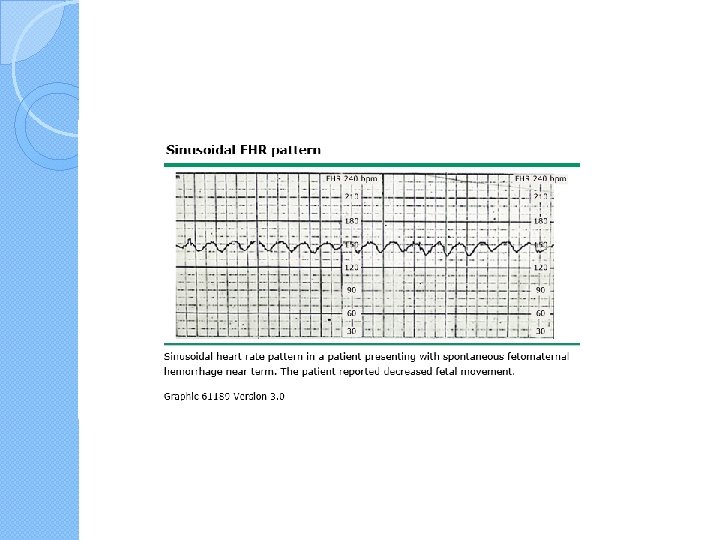
Sinusoidal Heart Rate �A true sinusoidal pattern intracranial hemorrhage, with severe fetal asphyxia, and with severe fetal anemia from Rh alloimmunization, fetomaternal hemorrhage, twin-twin transfusion syndrome, or vasa previa with bleeding �Insignificant sinusoidal patterns have been reported following �administration of meperidine, morphine, alphaprodine, and butorphanol
�An important characteristic of this pattern when due to narcotics is the sine frequency of 6 cycles per minute. � A sinusoidal pattern also has been described with chorioamnionitis, fetal distress, and umbilical cord occlusion �intrapartum sinusoidal fetal heart patterns were not generally associated with fetal compromise.
Sinusoidal fetal heart rate pattern associated with maternal intravenous meperidine administration. Sine waves are occurring at a rate of 6 cycles per minute
Modanlou and Freeman (1982), based on their extensive review, proposed adoption of a strict definition � 1. Stable baseline heart rate of 120 to 160 bpm with regular oscillations, � 2. Amplitude of 5 to 15 bpm (rarely greater), � 3. Long-term variability frequency of 2 to 5 cycles per minute, � 4. Fixed or flat short-term variability, � 5. Oscillation of the sinusoidal waveform above or below a baseline, and � 6. Absent accelerations.
�classification of sinusoidal heart rate patterns into mild—amplitude 5 to 15 bpm, intermediate— 16 to 24 bpm, and major— 25 or more bpm to quantify fetal risk
pseudosinusoid �intrapartum sine wavelike baseline variation with periods of acceleration as pseudosinusoid �Pseudosinusoidal patterns were seen in 15 percent of monitored labors. �Mild pseudosinusoidal patterns were associated with use of meperidine and epidural analgesia. � Intermediate pseudosinusoidal patterns were linked to fetal sucking or transient episodes of fetal hypoxia caused by umbilical cord compression.
�few D-alloimmunized fetuses develop this pattern (Nicolaides, 1989). �The sinusoidal pattern has been reported to develop or disappear after fetal transfusion
�the majority of fetal arrhythmias are benign and spontaneously convert to normal sinus rhythm by 24 hours after birth � Persistent tachyarrhythmias may cause fetal hydrops if present for many hours to days.
�Persistent bradyarrhythmias are often associated with fetal heart disease (eg, cardiac conduction defects due to anatomic derangements, autoantibody [SSA, anti-Ro] inducedcardiomyopathy related to lupus), but seldom result in hypoxemia or acidosis in fetal life
Category III tracings �associated with abnormal fetal acid- base status at the time of observation than category II tracings. � Prompt evaluation of these patients
�Fetal oxygen deprivation can lead to significant fetal acidosis (umbilical artery p. H <7. 0, base deficit ≥ 12 mmol/L), which is the precursor of intrapartum hypoxic neurologic injury. �The goal of intervention is to improve fetal oxygenation by improving uteroplacental perfusion
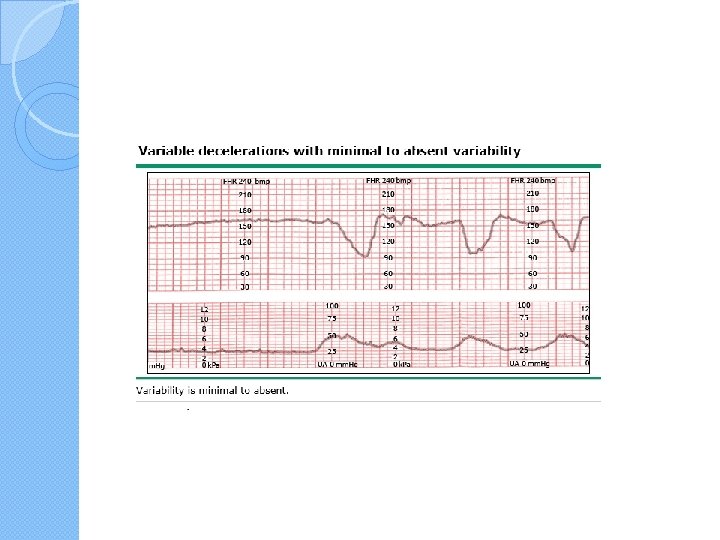
�●Absent baseline FHR variability and (any of the following): � • Recurrent late decelerations � • Recurrent variable decelerations � • Bradycardia �or �●A sinusoidal pattern
Absent or minimal variability with decelerations or bradycardia �The absence of FHR variability is thought to be a result of cerebral hypoxemia and acidosis, and signifies failure of fetal compensatory mechanisms to maintain adequate oxygenation of the brain. � absence of variability is often accompanied by abnormalities in FHR baseline or periodic late decelerations when the fetus is distressed.
�Nonhypoxia-related causes of diminished variability include anencephaly and other central nervous system defects, use of some centrally acting drugs (eg, opiates, magnesium sulfate, atropine), sepsis, defective cardiac conduction (eg, complete heart block), and quiet fetal sleep
Recurrent late decelerations � They can be associated with a falling fetal p. H and perinatal morbidity and �Recurrent late decelerations (ie, occurring with ≥ 50 percent of contractions in a 20 -minute segment) with absent variability are especially predictive of current or impending fetal acidosis due to progressively falling p. H
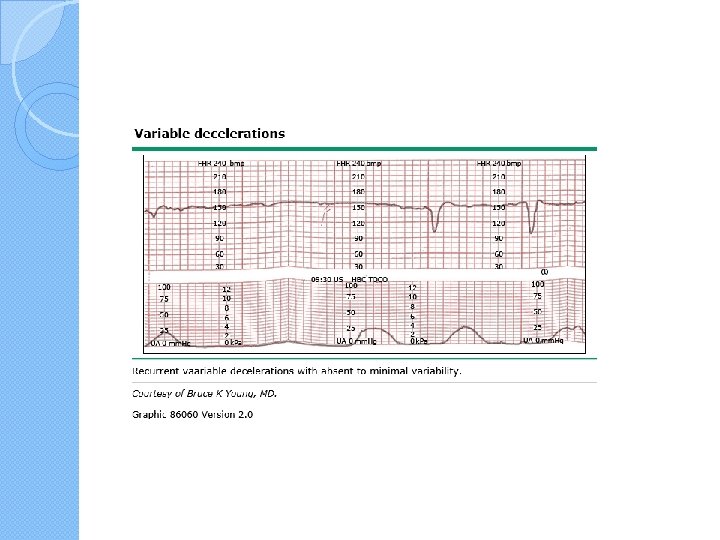
Recurrent variable decelerations �in labor tracings and are not usually associated with adverse consequences, presumably because transient cord compression is well tolerated by the fetus
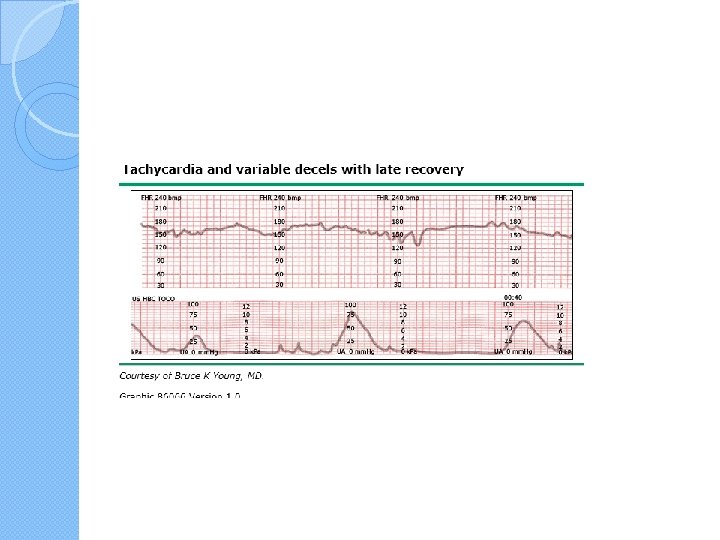
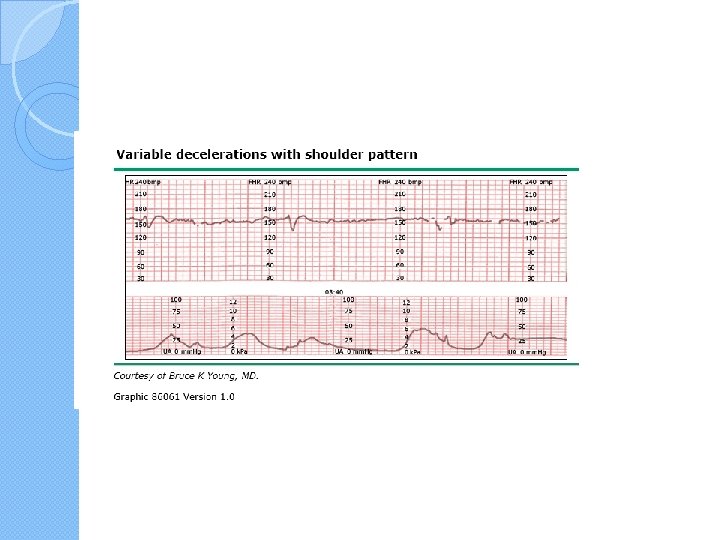
atypical variations �variable decelerations with lambda or W pattern (biphasic deceleration), slow return to baseline, loss of primary or secondary acceleration (shoulders), persistent secondary acceleration (overshoot), or reduction in postdeceleration baseline �persistent late recovery of the FHR to baseline has been associated with falling p. H, this has not been associated with significant reduction in Apgar scores
� The current NICHHD classification does not include atypical variable decelerations as a category of FHR pattern. �However, it does consider variable decelerations with absent baseline variability as predictive of an abnormal p. H.
Bradycardia � Bradycardia with absent variability appears as a smooth FHR below 110 bpm. �It is ominous when it occurs for a prolonged period of time (ie, at least 10 minutes) in the absence of hypothermia, complete heart block, or use of certain drugs (eg, beta-adrenergic blockers, paracervical block). �When the FHR falls below 100, tissue perfusion may not be adequate; this degree of bradycardia is nonreassuring
Sinusoidal heart rate pattern �Fetal scalp stimulation or fetal blood sampling may provide some reassurance that the fetus is not acidotic �In the absence of evidence of acidosis or other concerns, fetuses with a sinusoidal FHR pattern do not need to be delivered immediately. �The sinusoidal pattern sometimes resolves; �if acidosis or a worsening FHR pattern develops, we suggest urgent delivery
Category II tracings � FHR patterns that are category II are indeterminate. �The fetus may not be acidotic; however, continuation or worsening of the clinical situation may result in fetal acidosis. �continued surveillance and evaluation of these patients is indicated.
�Some examples of indeterminate patterns include tachycardia, minimal or marked variability, absent variability without recurrent decelerations, absence of accelerations without absent variability, recurrent late or variable decelerations without absent variability, and prolonged decelerations
FHR patterns associated with pre -existing fetal neurological injury � 50 to 90 percent of neurologically impaired infants are suffering from a Specific abnormal FHR patterns associated with neurological injury have been described and can be observed from the initiation of monitoring. The most common FHR abnormality is a persistent nonreactive heart rate and a persistent fixed baseline with minimal or absent variability
Causes of category II and III tracings unrelated to fetal hypoxemia � ●Fetal arrhythmias � ●Technical factors including a faulty leg plate, electrode, or monitor; setting the recording rate at 1 cm/min instead of the standard 3 cm/min; and the fact that very slow FH rates may be doubled and very fast rates (>240 bpm) may be halved by the machine. � ●The fetal and maternal heart beats are typically distinguished by the faster rate of the fetus (110 to 160 versus <100 bpm). they can beat at a similar rate. The fetal heart rate may be the same or slower than the maternal rate if there is a fetal heart rate deceleration or prolonged bradycardia or in the presence of maternal tachycardia due to fever or stress