The North of England Regional Back Pain Pathway

The North of England Regional Back Pain Pathway Nicki Skinner MSc MCSP MMACP Triage and Treat Practitioner 17 th March 2016

Background • • • Acute LBP experienced by 90% of population Back pain is largest cause of disability in UK (11% of disability burden) Global burden of disease 2010 Cost to NHS >£ 2 billion annually (Nice 2008) Huge management variation nationally and locally Poor adherence to evidence based guidelines
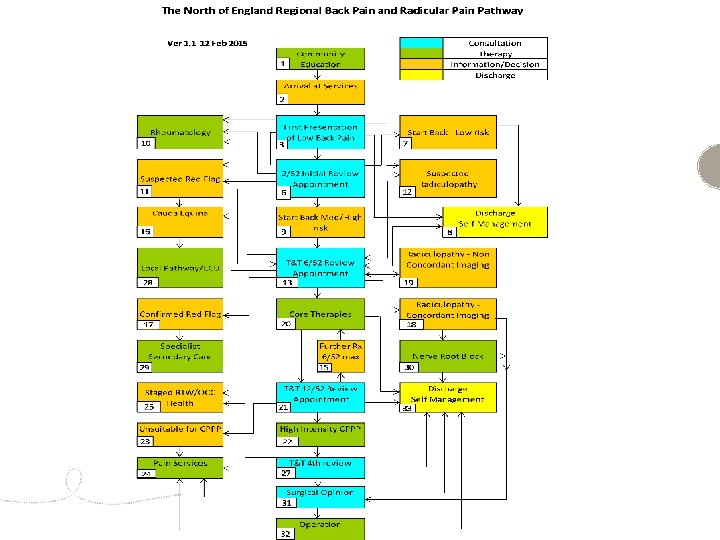

1 st consultation GP/Self Referral to Physio Red Flags Local Pathway 2 nd consultation GP – STar. T Back Triage and Treat Imaging Core Therapies Discharge Triage and Treat NRB Core Therapies Surgical Opinion CPPP Pain Clinic

What’s new? • • • Evidence based care with emphasis on prevention of chronicity Standardised managed pathway with consistent message from all healthcare professionals Integrated pathway with rapid access to appropriate services Combined physical and psychological programme (CPPP) – Back to Health Save money!

STar. T Back APPROACH • • • STar. T Back tool – 9 item self-reported questionnaire Physical and psychological constructs STar. T Back stratifies patients according to their risk of persistent disability due to back pain. Scored as high, medium or low risk Hill et al (2011) – stratified care is cost effective with targeted care towards med/high risk and avoids over-treatment of low risk

Managed pathway Triage and Treat • • • Spinal specialists – physiotherapists, nurses Named clinician responsible for each patient Working in an extended scope role with responsibility for ordering and interpreting investigations then directing care appropriately Promote and reinforce self-management Part of the MDT team

Consistent message • • Every clinician has the potential to be a yellow flag. (Darlow et al 2013) Patient and clinician beliefs affect outcomes “Weakness, instability, trapped nerves, wear and tear, disc bulge, degeneration” versus “Safe, strong, sensitive, active, relaxation, normal” Reassurance, advice and information to promote self-management.
 • • NICE (2009) – programme consisting of around 100")
Back to Health (CPPP) • • NICE (2009) – programme consisting of around 100 hrs over maximum 8 weeks Spinal Taskforce (2013) – serious gap in current services and recommendation to commissioners MDT approach Change mindsets Improve self management Increase exercise and functional ability Demedicalise Return to work

Physiotherapy and the future! • • Sir Bruce Keogh supporting national roll out Physiotherapists best placed to lead and deliver services. – Advanced clinical reasoning – Exercise prescription – Manual therapists – Acupuncture – Relaxation – Cognitive behavioural therapy – Team workers
- Slides: 10