The normal labor delivery Sun Dina Definition v

The normal labor & delivery Sun Dina

Definition: v The products of conception which include fetus and placenta are expulsed from mater. v It goes with effective sequence of involuntary uterine contractions, which result in effacement and dilatation of the cervix and voluntary bearing-down efforts.

Definition: A delivery that occurs before 28 weeks of gestation is called an abortion. In some other countries, the time defined as 20 or 24 weeks. v It is a dynamic process. v

Relative Definitions: v premature delivery: The delivery occurs between 28 weeks and 36+6 weeks. v Term delivery: The delivery occurs between 37 weeks and 41+6 weeks. v Postterm delivery: The delivery occurs 42 weeks or more.

Relative Definitions: v Parity: the state of having given birth to an infant or infants weighing 500 g or more, alive or dead. The length of gestation of 24 weeks or more may be used. v Nullipara: the woman has not delivered an offspring weighing 500 g or more or of 24 weeks gestation or more.

Relative Definitions: v Primipara: the woman has given birth to such a fetus once. v Multipara: the woman has given birth to such a fetus more than once.

Relative Definitions: v Gravidity: it refers to the total number of pregnancies, including abortions, hydatidiform moles, ectopic pregnancies, and normal intrauterine pregnancies. v Nulligravida: the woman has never been pregnant.

Relative Definitions: v Primigravida: the woman has been pregnant only once. v Multigravida: the woman has been pregnant more than once.

Relative Definitions: True labor: it is characterized by regular uterine contractions which become more frequent and forceful and of longer duration with the passage of time, accompanied by effacement and dilatation of the cervix. v False labor: it is quite common in late pregnancy, which characterized by irregular brief uterine contractions, inconsistent in interval and strength and cause no changes in the cervix. v

ueffacement of the Cervix internal os uteri external os uteri the onset of labor udilatation of the cervix uncomplete effacement of the cervix Full dilatation nullipara multipara

Mechanism of initiation of labor: Many theories have been proposed over the years. v mechanical theory v Endocritic theory v Neurological medium theory

Essential factors of labor There are four factors that influence the progress and final outcome of labor. powers (the contractions or forces of the uterus) v passage (the bony and soft tissues of the maternal pelvis) v passenger (the fetus) v psyche v

The powers: v The uterine contraction: It is the main power during labor and last for the whole puerperal process. It can make the effacement and dilatation of the cervix, accompanied the descent of the fetal presenting part. It also can make the fetus and placenta expulse.

The characters of the uterine contraction: vrhythmic Progressive period Polar period contraction Recessive period Interval contraction

The characters of the uterine contraction: vsymmetrical and polar

The characters of the uterine contraction: v Brachystasis Each individual myometrial cell as it contracts does not quite regain its normal length on relaxation.

uterine muscle fibers Brachystasis of the uterine muscle fibers

The powers: There have other powers: v Contraction of levator ani muscle It is very important in the internal rotation of the fetus. v Maternal efforts It is useful in the second stage of labor cooperating with uterine contractions.

The passage: v Bony pelvis: true pelvis Inlet pelvis midpelvis Outlet pelvis false pelvis v Pelvic soft tissues Midpelvis Outlet pelvis

The passage: Bony pelvis: The progress of delivery is directly determined by the sequence of attitudes and positions the fetus must assume in its passage through the birth canal. So a reasonably accurate assessment of the pelvic architecture and the pelvic diameters is an important part of obstetric care.

The passage: Bony pelvis v 1. 2. 3. 4. There are four basic generally pelvic confuguration. gynecoid android anthropoid platypeloid Most pelvis are mixed types. gynecoid android anthropoid platypeloid

Pelvic landmarks: Pelvic inlet: 1. anteroposterior diameter: 11 cm 2. transverse diameter: 13 cm 3. diagonal diameter: 12. 75 cm v
 diameter: 10")
Pelvic landmarks: Midpelvis: 1. anteroposterior diameter: 11. 5 cm 2. Transverse (interspinous) diameter: 10 cm v

Pelvic landmarks: Pelvic outlet: 1. anteroposterior outlet: 11. 5 cm 2. Transverse outlet: 9 cm 3. Posterior sagittal: 8. 5 cm 4. Anterior sagittal: 6 cm v the outlet pelvis from incline

Pelvic landmarks: If the transverse outlet is short, we can use the sum of the transverse and the posterior sagittal. If the sum is 15 cm or more, the moderate fetus also can be delivered.

The passage: pelvic soft tissues v The soft tissues have an effect on the type and progress of labor. v The levator ani muscles helps in the forward rotation of the presenting part during labor. v The anatomy of the uterus and the vagina may vary the progress of labor. eg, vaginal septa or constrictions, which should be noted prior to the onset of labor.

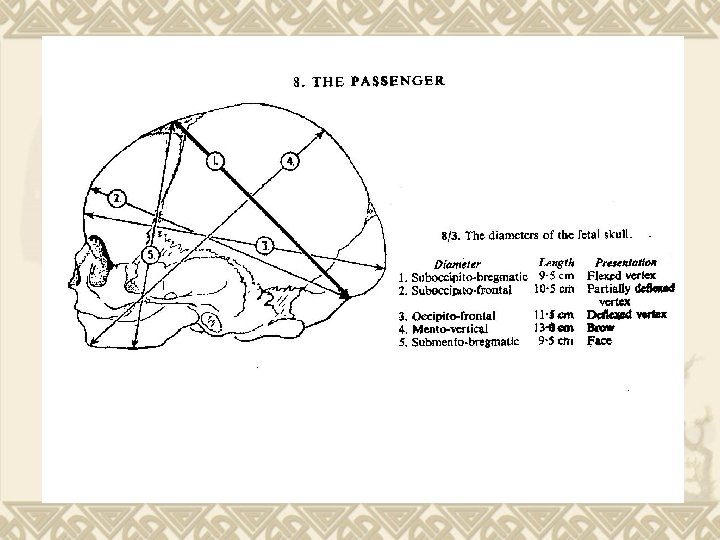
The passenger: v The fetus can be delivered successfully or not lying on the fetal size, position and whether or not existing abnormality.
: average 9. 3 cm v Occipito frontal diameter:")
fetus Anterior fontanelle Biparietal diameter (BPD): average 9. 3 cm v Occipito frontal diameter: BPD average 11. 3 cm v Occipito bregmatic diameter: average 9. 5 cm v Occipito mental diameter: Posterior fontanelle average 12. 5 cm v

Fetal presentation, position & lie Cephalic presentation Breech presentation Shoulder presentation longitudinal lie Transverse lie

Fetal presentation, position & lie occipito presentation Anterior fontanelle presentation brow presentation face presentation

Fetal presentation, position & lie complete breech frank breech incomplete presentation

Fetal presentation, position & lie If the presentation is the occipital, the reference point will be occiput. v If the occiput lies in contact with left iliopubic eminence, its position will be left occipito anterior. v Fetal position left occipito anterior

Fetal abnormality: conjoined twins hydrocephalus

The psyche: v. A high level of anxiety during pregnancy has been associated with decreased uterine activity and with longer and dysfunctional labor.

The psyche: v Prenatal education classes v Be supported psychologically as well as physically v Be encouraged to participate in prenatal exercise classes v Learn various psychoprophylactic techniques

The course of normal labor: Labor is commonly divided into 3 stages: Ø The first stage Ø The second stage Ø The third stage

The first stage: v Begin with the onset of labor v Ends with the completely dilatation of the cervix (10 cm). v The average duration of the first stage of labor is 8 -12 hours in a primigravida and 6 -8 hours in a multipara.

The second stage: v From full dilatation of the cervix to the birth of the baby v It varies from a few minutes to two hours depending on both fetal and maternal factors.

The third stage: v From the birth of baby to the delivery of the placenta v Postpartum hemorrhage occurs greatly immediately after the third stage.

Mechanism of labor: v Engagement v Flexion v Descent v Internal rotation v Extension v External rotation and restitution v Delivery of the fetus

Engagement Generally occurs in late pregnancy or at onset of labor v The head (BPD) of the fetus enter into the pelvic inlet. v

Flexion It is essential for both engagement and descent. v It utilizes the smallest diameter. v

Descent: v Descent is gradually progressive and is last for the whole process. v The descent of the head is the main sign of the stage of labor.

Internal rotation When the head descend to the midpelvis, rotation occurs. v In cases of occipitoanterior vertex, the head has to rotate 45 degrees and in occipitoposterior vertex, 135 degrees, to pass beneath the pubic arch. v Internal rotation

Extension v When the head is beyond the introitus and the occiput is beneath the symphysis pubis, extension occurs. the beginning of extension the completion of extension

External rotation and restitution When the head is delivered, the external rotation occurs so that the head rotates to the position which accord with the engagement. v Then the shoulder descend in a path similar to that traced by the head. v External rotation

Delivery of the fetus anterior shoulder delivers posterior shoulder delivers

Management of early labor: v v v Ø Ø Confirm labor Identify significant abnormalities, such as fetopelvic disproportion and ineffectual uterine contractions. The history should be recorded the onset of contractions the presence or absence of bleeding the possible loss of amniotic fluid the fetal heart tones and activity of the fetus.

Management of early labor: v Initial examination & procedures v Preparation of the patient for labor v Supervision of the first stage of labor v Preparation for delivery

Initial examination & procedures The initial examination include a basic evaluation of her current clinical condition and the reactions to labor, anxiety or tension.

Initial examination & procedures The following procedures should be performed. u Obtain a history of medical details u Record the vital signs u Obtain a clean-catch urine specimen and test for protein and glucose. u Do a brief general physical examination. u Examine the abdomen

Initial examination & procedures u Note the uterine contractions u Record the type and amount of the vaginal bleeding or loss of amniotic fluid u Vaginal examination • dilatation of cervix • effacement of the cervix • the position of the presenting part u Other examinations: ultrasonograms

ischial spine

Preparation of the patient for labor v Cleanse the perineum v Enemas or laxative suppository v Ambulation except the women who have the ruptured membrane, been bleeding or been administered sedative. v Analgesics including meperidine, butorphanol and nalbuphine.

Preparation of the patient for labor Diet and fluids v clear liquids are permissible. v The patient with a known risk for operative delivery should have oral intake restricted to small amounts of water or ice chips.

Supervision of the first stage of labor v Record the fetal heart tones v Examined abdominally and vaginally v Record the uterine contractions, tone of the uterus and the general reaction of the patient v Encourage the patient to void as labor progresses v Permit the patient to ambulate

Preparation for delivery v Anesthesia and resuscitation equipment and drugs v Sterile surgical instruments v Drapes, sponges, sutures v Povidone-iodine ( betadine )

Management of the second stage of labor v This stage may last as long as 1 -2 hours. v We should be alert to the imminence of delivery. v Anesthesia: pudendal block, local anesthesia

Management of the second stage of labor v Episiotomy: median episiotomy or medio-lateral episiotomy Median episiotomy

Management of the second stage of labor v Head visible on vulval gapping v crowning of head Head visible on vulval gapping

Immediate care of the infant v Clear the air passages v Record the apgar score v Resuscitation measures v Preserve body heat v Deal with umbilical cord and eye v A general physical examination

Immediate care of the mother postpartum v Inspecting the birth canal, including perineum, vagina and cervix v Lacerations, hematomas or extension of episiotomy incisions

Immediate care of the mother postpartum There are four degrees of laceration. 1. Only mucosa or skin (or both) is damaged. 2. Tears of the mucosa or skin (or both) plus disruption of the superficial fascia and the transverse perineal muscle 3. Previous structures plus the anal sphincter 4. Including entry into the rectal lumen

Management of the third stage of labor The signs of the expulsion of the placenta: 1. The uterus becomes globular 2. The umbilical cord becomes longer 3. Brisk bleeding 4. Place your hand above the symphysis pubis, the uterus rise and the umbilical cord no longer recede

the beginning of the placenta in the placenta expulsion of placenta lower segment expulsed

Management of the third stage of labor Inspect the placenta 1. The cotyledons are missing or not. 2. The membranes are complete or not. 3. There is succenturiate placenta or not. If the conditions above exist, we should expulse these retain tissue with sterile means.

succenturiate placenta

Management of the third stage of labor In this period, we should be alert to the postpartum hemorrhage and be in-dwelling for emergency therapy.

- Slides: 70