The lung and the Upper Respiratory Tract Lung



 2. Adenocarcinoma 1. Bronchial derived")
 Increase in women and decreasing in")
 70 -75% of all lung Ca cases:")
")














: –")

. – Migratory thrombophlebitis. Lambert-Eaton")







: presence")
= –")




- Slides: 38
The lung and the Upper Respiratory Tract Lung Tumors
Lung tumors : General features Most are malignant. Metastatitc neoplasms are most common.
Types Bronchogenic Carcinoma. Bronchial carcinoids. Lymphoma. Hamartoma
Bronchogenic carcinoma 1. Squamous cell carcinoma ( most common) 2. Adenocarcinoma 1. Bronchial derived 2. Broncheoloalveolar Non small cell carcinoma 3. Larger cell carcinoma 4. Small cell (oat cell) carcinoma.
Bronchogenic Carcinoma Leading case of cancer death (M/F) Increase in women and decreasing in men. Age: old adult. Etiology: – smoking of cigarettes ( amount/ years). – Asbestosis – Uranium and radiation – Air pollution – Radon
Molecular pathology Non-Small Cell Lung Carcinomas (NSCLC) 70 -75% of all lung Ca cases: – p 16/CDKN 2 A & K-RAS mutations, – p 53 mutation ( inhibit apoptosis). Small Cell Lung Carcinoma (CSLC) 20 -25%, TP 53 & RB gene mutations ( deregulate cell cycle).
Squamous cell carcinoma Central tumor Arising from Squamous cell ( often from main bronchus) Smoking is main etiology also caused by radon. p 53 mutation and overexpression of epidermal growth-factor receptor very common. Morphology: next
Squamous cell carcinoma: The neoplasm is very firm and has a pale white to tan cut surface. Central necrosis is frequently seen. Central necrosis
Micro: nests of polygonal cells with pink cytoplasm and distinct cell borders with intercellular bridges and keratin pearl.
Adenocarcinoma Peripheral tumor. Sex: female. Age: much younger person. Types: – Bronchial derived: occur in the site of previous scar (scar carcinoma). Not clearly linked to smoking. – Bronchoalveolar Ca: Not related to smoking. Multiple tumor, present as pneumonia.
Adenocarcinoma : peripheral tumor K-RAS mutations are seen primarily in adenocarcinoma.
Adenocarcinoma: The glandular structures formed by this neoplasm + mucin production ( mucin stained purple with PAS)
Bronchioloalveolar carcinoma Appears as pneumonic consolidation. Well differentiated tumor: better prognosis.
Bronchioloalveolar carcinoma is composed of columnar cells that proliferate along the framework of alveolar septae.
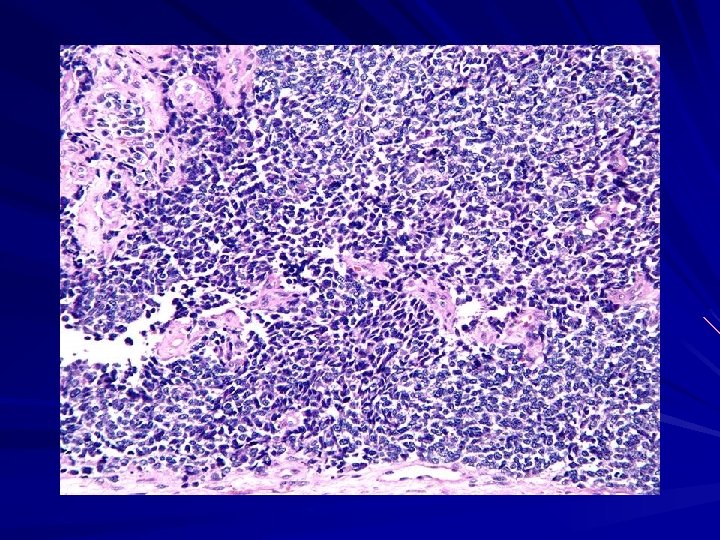
Small Cell Carcinoma: central tumor Central tumor. Aka- oat cell carcinoma Origin: Neuroendocrine argentaffin (Kulchitsky) cells. Smoking is main etiology Gene: p 53 and RB tumor suppressor genes + over expression of the anti-apoptotic gene BCL 2. Poor prognosis.
Gross: This Th tumor has a soft, lobulated, white to tan appearance. Micro: sheets of blue cells are regular, and round molded nuclei and a moderate amount of eosinophilic cytoplasm. Blue round cells
Large cell carcinoma Micro: large anaplastic cells. Poor prognosis
Relax your eyes Next topic : Clinical features of tumors
Clinical Common presentation: Cough, hemoptysis, weight loss. Clubbing of the fingers. Others: – Due to spread of tumor – Due to paraneoplastic syndromes
Clinical: Due to spread of tumor Local lymph nodes metastasis; – Supraclavicular node (Virchow node). Distant : Brain, Liver , Bone. – Adrenals cortex (Addison’s diseasedeficiency of cortical hormones- skin & mucosa hyper pigmentation)
Others Superior Vena caval syndrome (common in small cell carcinoma, followed by squamous cell Ca. ) – Congestion of veins of neck, face: red – Engorges jugular vein- edema in arms. Hoarseness: recurrent laryngeal nerve invasion ( with apical tumor). Acanthosis nigricans: black, thick skin with skin tags= axillae, groin etc (common in adenocarcinoma).
Clinical: Due to spread of tumor Horner syndrome ( in Pancoast tumor ): – Seen in apical tumors due to involvement of cervical sympathetic plexus. – Features are: Ipsilateral enophthalmos. Ptosis, Meiosis. Anhidrosis.
Clinical: Due to paraneoplastic syndromes Squamous cell carcinoma Secret PTH like hormone > Hypercalcemia→ renal calculi Small cell carcinoma Secret ACTH>Cushing syndrome= weight gain, hypertension. Skin pigmentation Secret ADH > SIADH > Hyponatremia= cerebral edema
Other Paraneoplastic syndromes in bronchogenic carcinoma Hematologic manifestations (In adenocarcinoma). – Migratory thrombophlebitis. Lambert-Eaton myasthenic syndrome ( In Small cell carcinoma: muscle weakness is caused by auto-antibodies directed to the neuronal calcium channel). Calcitonin, causing hypocalcemia.
Bronchial Carcinoid Origin: Kulchitsy cells: a neuroendocrine cells that line the bronchial mucosa. Age: mean around 40. Gross: yellow polypoid mass. Micro: – LM: Salt pepper. – EM: Dense core neurosecretory granules in their cytoplasm
Microscopy Salt pepper Dense core granules
Presentation of Carcinoid Benign carcinoid: – Cough. – Hemoptysis, bronchiectasis. – Recurrent bronchial & pulmonary infections. Malignant carcinoid: liver mets. and Secret serotonin > carcinoid syndrome: diarrhea and flushing on skin.
Hamartoma Common Less than 2 cm. Micro: haphazard lung tissue and cartilage. Clinical: Present as a "coin lesion" on X-ray. d/d of coin lesion Granuloma are multiple. coin lesion
Metastatic Cancer to the lungs Multiple variably-sized masses are seen in all lung fields.
Next Topic Mesothelioma Pleural effusion
Malignant Mesothelioma Site: The visceral or the parietal pleura. Carcinogen: asbestosis- amphiboles by reactive free radicals. Morphology: – Asbestos bodied are found in the tumor. – Lung gets ensheathed by tumor tissue may produce cicatrisation and atelectasis.
Diagnosis of malignant mesothelioma Positive staining with: Acid mucopolysaccharide Keratin Electron microscopy (EM): presence of long microvilli and abundant tonofilaments.
Pleural effusion Empyema- Pus in pleural cavity following abscess. Chylothorax : Chyle (lymph)= – It is a Milky white fluid due to tumor emboli in lymphatic or in Lymphoma. All patient present with respiratory distress, relieved when the effusion in drained by thoracentesis.
Pneumothorax Def: air in pleural cavity Types: – Traumatic: Trauma – Spontaneous: rupture of paraseptal bulla – Tension : due to shift of the mediastinum from the midline. Tracheal shifting to other side , and hyperresonant lung on side of injury.
Thank you
Thank you