The Knee Unit the knee joint is the





")













")

")

 the outer 1/3 is")

")





 As the knee increases in flexion, the PFJRF")










- Slides: 51
The Knee Unit
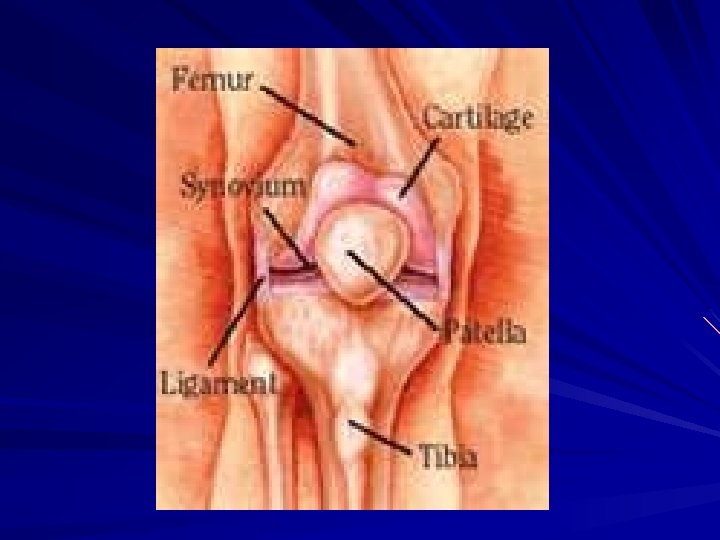
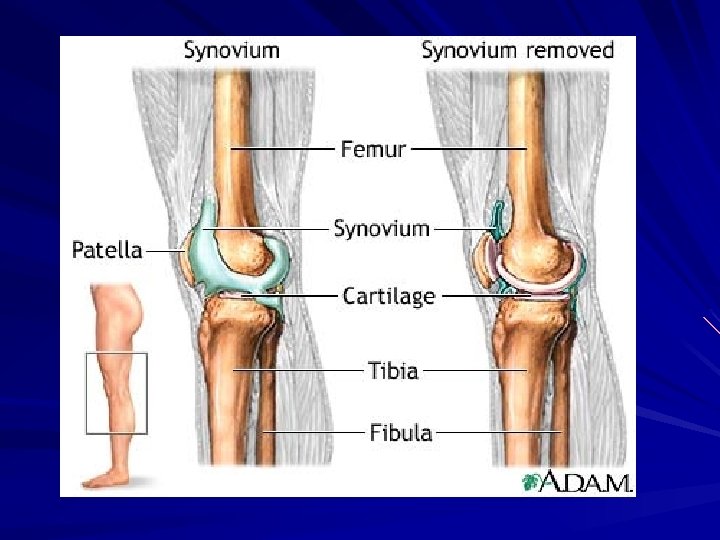
the knee joint is the largest joint space in the body it is greatest at 30 degrees of flexion the knee is considered a synovial joint b/c it is aligned with the joint capsule the synovial layer secretes synovial fluid (like oil to a car) to help lubricate the joint and keep it moving purpose of synovial fluid – lubrication – nutrient rich
BONES
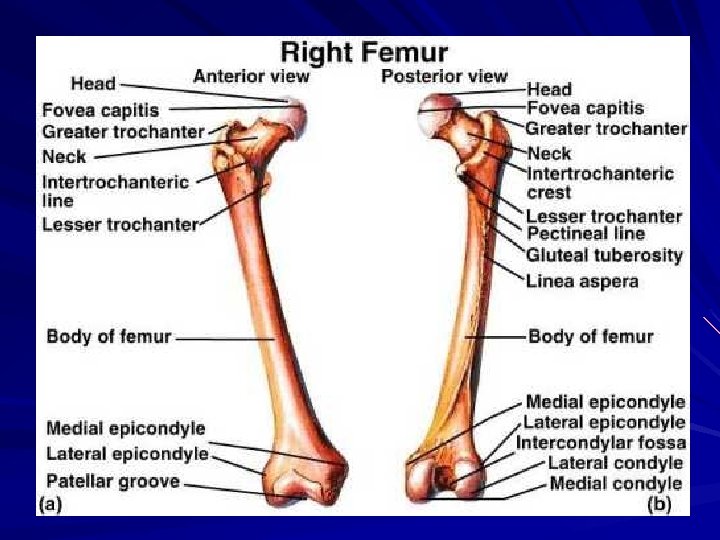
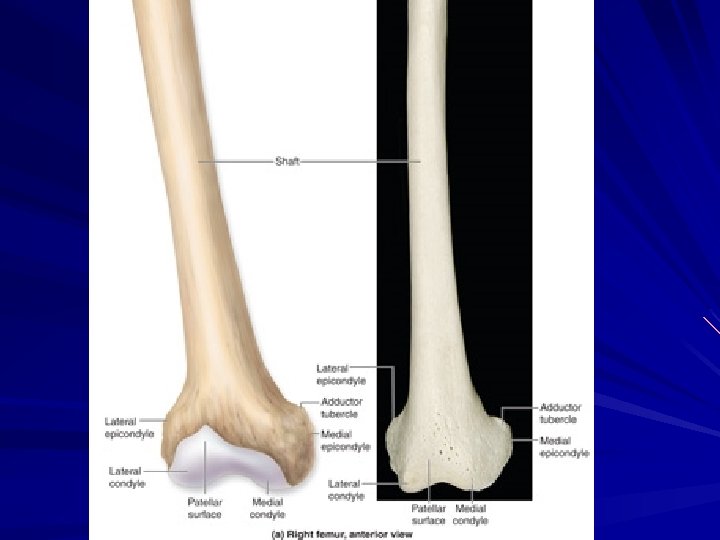
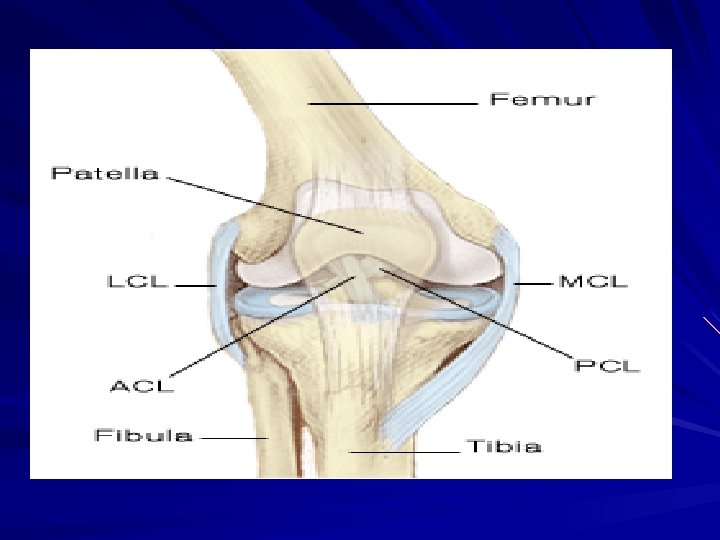
Femur largest bone in the body distal end makes up knee – forms convex medial and lateral condyles – medial condyle is larger and longer in the AP direction, which causes external tibial rotation
Screw Home Mechanism - external tibial rotation when the knee is fully extended due to the medial condyle being larger than the lateral condyle proximal end makes up hip trochlear groove - hollow area between 2 condyles where the patella glides
Tibia 2 tuberosities – concave in nature – separated by popliteal notch (Tibial Spine) ACL & PCL attach to the tibial spine ACL & PCL are named from their attachment on the tibia Tibia Fracture
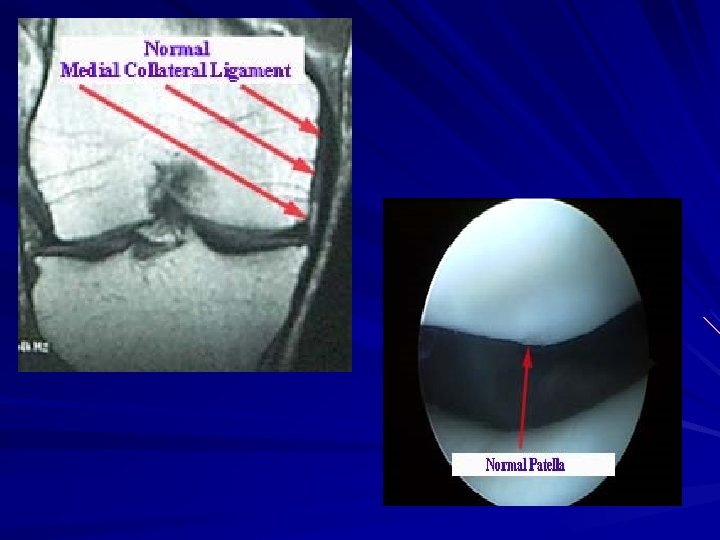
Patella Sesmoid bone – largest one in the body – lies within the quad tendon to increase function Function – protect anterior knee – increase mechanical advantage
patella is most palpable in extension b/c it is above the trochlear groove at 30 degrees of flexion, the patella is in the trochlear groove patella is held in place by the retinaculum lateral retinaculum is stronger than medial retinaculum
patella baja - low riding patella; more prone to fat pad irritaiton & tendonitis; injuries tend to be overuse injuries
patella alta - high riding patella; more prone to dislocation
Why patella dislocation happens laterally ? weak VMO shallow trochlear groove small or abnormal patella increased Q-angle tight IT band tight lateral retinaculum
Chondromalacia Patella
LIGAMENTS ALL STATIC STABILIZERS
MCL - Medial Collateral Ligament Injured by valgus force 2 parts – Deep close to bones; thin layer thickening of joint capsule, intracapsular injury causes effusion (joint swelling) attaches to the medial meniscus – Superficial forms the MCL palpable extracapsular injury causes edema (swelling outside the joint)
LCL - Lateral Collateral Ligament thickening of capsule does NOT attach to lateral meniscus attaches to fibular head and attaches to lateral epicondyle very palpable
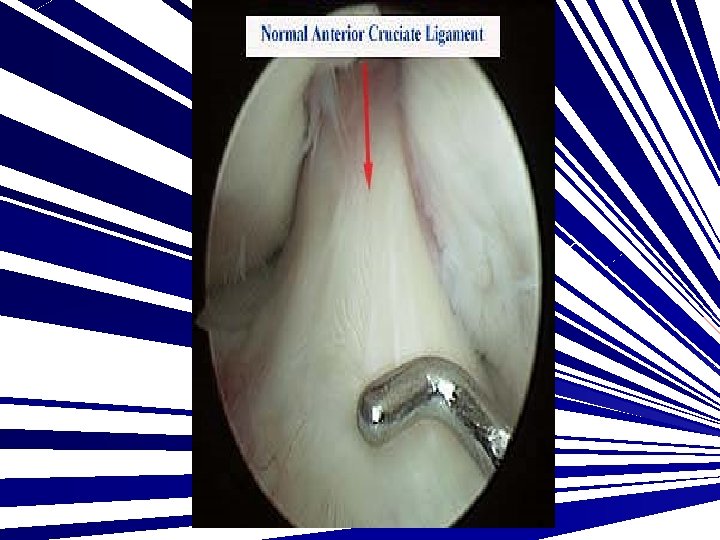
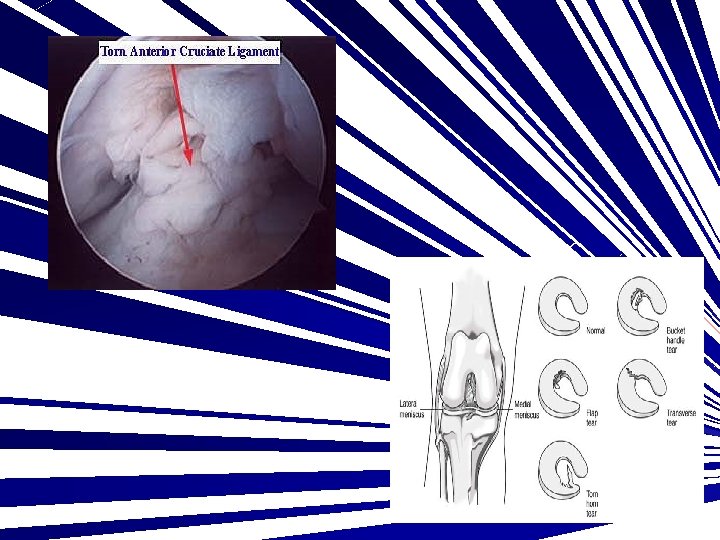
ACL - Anterior Cruciate Ligament attaches on tibia and lateral femoral condyle (medial aspect) moves superior, posterior, lateral injury happens by anterior blow to femur or deceleration with rotation prevents the tibia from moving anteriorly
PCL - Posterior Cruciate Ligament attaches on tibia and medial femoral condyle (lateral aspect) moves superiorly, anteriorly, medially injury happens by anterior blow to tibia or posterior blow to femur
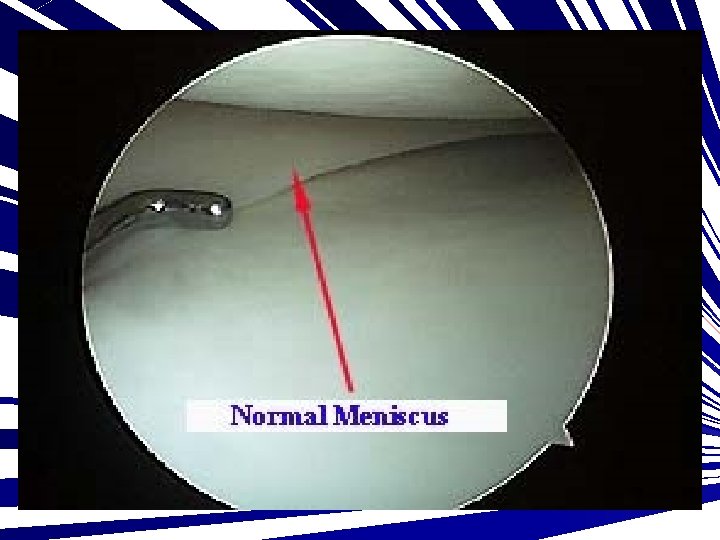
MENISCUS curved, wedged, fibrocartilaginous discs lies between the femoral condyles and tibial plateaus the outer edge is thicker than the inner edge
the inner 2/3 of menisci are avascular (no blood supply) the outer 1/3 is called the "red zone" because it is highly vascular (has blood supply) reasons for having the menisci – enhance stability of knee – assist with knee motion by decreasing friction – shock absorber
Menisectomy - removal of the meniscus the lateral and medial meniscus are connected by the transverse ligament located in front of the tibial spine Medial meniscus - "C" shaped Lateral meniscus - "O" shaped Medial meniscus is larger than lateral meniscus Medial meniscus is attached to entire periphery (outer edge), and intrachonduloar eminence (tibial spine), which is also the attachment for the ACL Lateral meniscus is loosely attached
Meniscal Tears Bucket Handle – occurs in the middle of the meniscus (red-white zone) – often times posterior – most common Peripheral Tear – red zone – responds extremely well to surgery Avascular Tear – white zone – must be removed and cleaned up on the edges – heals poorly because no blood supply
Hamstring Group
Quadricep Group
Patella Femoral Assessment
Patella Femoral Joint Reaction Force (PFJRF) As the knee increases in flexion, the PFJRF increases The reaction force in through the patella from the increased pull on the patella tendon and the quadriceps muscle As knee flexion increases the angle between the quad and the patella tendon decrease creating more force in the joint
Increased weight distribution in the patella Level walking 0. 5 x body weight Stair climbing 3 -4 x body weight Squatting 7 -8 x body weight ****proper lifting techniques decrease the stress on the patella and the knee joint
Symptoms of Patella Femoral Pain Diffuse ache on the anterior knee Pain with stair climbing “moviegoers” knee crepitus (clicking/popping) giving away swelling locking, catching
Mechanics of Patella Femoral Joint Patella functions to increase quad control During 1 st 20 degrees of flexion, the tibia derotates (internal rotation) and the patella is drawn into the trochlear groove Tibial derotation causes a decrease in the QAngle
Mechanics of Patella Femoral Joint Patella stays in trochlear groove ~ 90 degrees and then moves laterally In full flexion, the lateral femoral condyle is covered by the patella The ability of the patella to track properly in the groove is dependant upon the bony structures and the balance of forces of soft tissue
Mechanics of Patella Femoral Joint Lateral forces are resisted by Medial Retinaculum Vastus Medialis Oblique (VMO) Lateral forced aided by Q-Angle Lateral Retinaculum (3 -4 x stronger than medial) Iliotibial (IT) Band Vastus Lateralis The only medial stabilizer is the VMO It is active through the full ROM VMO & VL need to have 1: 1 Ratio for proper knee function
Patella Malalignments
Patella Glide
Patella Tilt
Patella Rotation
Patella AP Tilt