The Kidneys Overview Introduction What do the kidneys







 • The e. GFR test is used to")
 Kidney Damage Stage Description GFR 1 Normal or")






 • Urea is a waste product made when protein is")















 Calcium oxalate crystals; (B) uric acid crystals (C)")











- Slides: 46
The Kidneys
Overview • • Introduction What do the kidneys do? What is renal function? Causes of kidney diseases What medical tests detect kidney disease? Diseases of the kidneys Management of kidney disorders
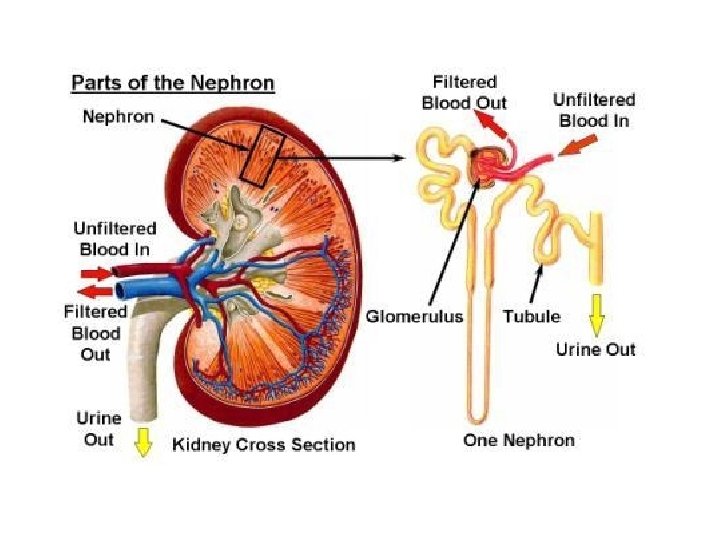
Introduction • The kidneys are bean-shaped organs, each about the size of a fist. They are located near the middle of the back, just below the rib cage, one on each side of the spine.
Kidney functions • The Kidneys have three major functions: 1. Excretion of wastes 2. Maintenance of ECF volume and composition 3. Hormone synthesis
What is renal function? • The word "renal" refers to the kidneys. • The term "renal function" is used to talk about how efficiently the kidneys filter blood. • Kidney function is now calculated using a blood sample and a formula to find the estimated glomerular filtration rate (e. GFR). • The e. GFR corresponds to the percent of kidney function available.
Causes of kidney diseases 1. 2. 3. 4. 5. Diabetes High blood pressure Glomerular diseases Inherited and congenital kidney diseases Poisons and trauma
Biochemical investigation of renal function • • 1. 2. 3. 4. • e. GFR Tests of glomerular function Measurement of creatinine clearance Creatinine Urea Cystatin C Tests of tubular function Urine osmolality Fluid deprivation test Urinary acidification tests Glycosuria Urinalysis
Estimated Glomerular filtration rate (e. GFR) • The e. GFR test is used to screen for and detect early kidney damage and to monitor kidney status. • It is performed by ordering a creatinine test and calculating the e. GFR.
Estimated Glomerular filtration rate (e. GFR) Kidney Damage Stage Description GFR 1 Normal or minimal kidney damage with normal GFR 90 + 2 Mild decrease in GFR 60 -89 3 Moderate decrease in GFR 30 -59 4 Severe decrease in GFR 15 -29 5 Kidney failure < 15
Creatinine clearance test • Measures how well creatinine is removed from the blood by your kidneys. • A creatinine clearance test is done on both a blood sample and on a sample of urine collected over 24 hours (24 -hour urine sample).
Plasma creatinine • The blood creatinine level shows how well your kidneys are working. • A high creatinine level may mean your kidneys are not working properly. • Men generally have higher creatinine levels than women. (Why? )
High plasma Creatinine • Acute or chronic renal failure • A high meat intake can cause temporary increase. • Exercise • Some drugs such as antibiotics and salicylates
Low plasma creatinine • In subjects with a small total muscle mass. • A low plasma creatinine may be found in children. • In pregnancy • Patients treated with corticoids • Starvation
Relationship between creatinine clearance and plasma creatinine concentration.
Creatinine clearance or plasma creatinine? • A normal plasma creatinine does not necessarily imply normal renal function, although a raised creatinine does usually indicate impaired renal function. • Measurement of plasma creatinine is more precise than creatinine clearance. (Why)?
Blood Urea Nitrogen (BUN) • Urea is a waste product made when protein is broken down in your body. • Urea is made in the liver and passes out of your body in the urine.
High Urea • Pre-renal • Increased hepatic production of urea: 1. high protein diet 2. gastro-intestinal haemorrhage - "protein meal" 3. increased protein catabolism - trauma, major surgery, extreme starvation with muscle breakdown • increased renal reabsorption of urea - any cause of reduced renal perfusion, for example, congestive cardiac failure, shock, severe diarrhoea. • Drug therapy leading to an increased production e. g. tetracyclines, corticosteroid • Renal • any cause of acute or chronic renal failure • Post-renal • any cause of urinary outflow obstruction
Low urea • • • Severe liver diseases. Pregnancy Very low protein diet Certain medications Low muscle mass
Cystatin C • Cystatin C may be used as an alternative to creatinine and creatinine clearance to screen for and monitor kidney dysfunction. • Measuring Cystatin C may be useful in the early detection of kidney disease when other test results may still be normal.
Urine osmolality • A urine osmolality test is a measure of the concentration of dissolved minerals (like sodium or salt) and wastes (like BUN) in a person's urine relative to water content. Higher mineral content and lower amounts of water lead to a high osmolality.
Urine osmolality • • Urine osmolality is dependent on 3 things: kidney function water intake the level of hormones released from the pituitary gland that help reabsorb water in the kidney (called Antidiuretic Hormone or ADH).
Fluid deprivation test • A fluid or water deprivation test is a medical test which can be used to determine whether the patient has diabetes insipidus as opposed to other causes of polydipsia.
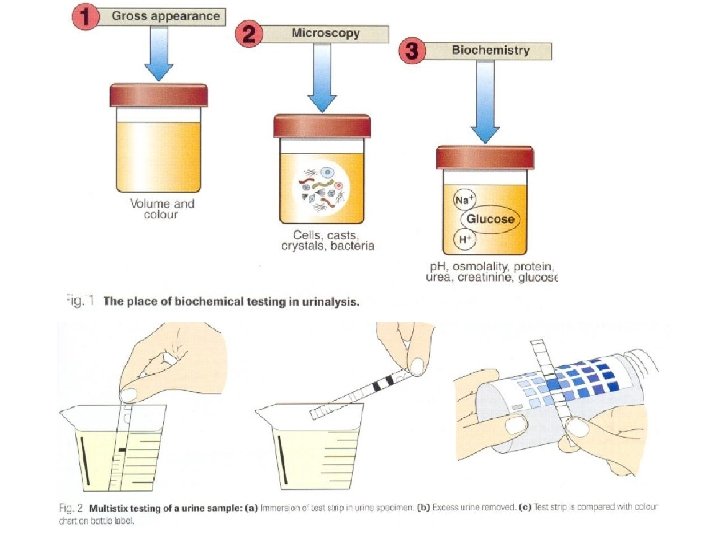
Urinalysis • • Appearance Specific gravity Osmolality p. H Glucose Protein Urinary sediments
Urinalysis Ø is important in screening for disease Ø is routine test for every patient, and not just for the investigation of renal diseases Ø Urinalysis comprises a range of analyses that are usually performed at the point of care rather than in a central laboratory.
Chemical analysis of the urine Glucose Bilirubin Ketones Specific Gravity Blood p. H Protein Urobilinogen Nitrite Leukocyte Esterase
Appearance
Specific gravity • This is a semi-quantitative measure of concentration. • A higher specific gravity indicates a more concentrated urine. • Assessment of urinary specific gravity usually just confirms the impression gained by visually inspecting the colour of the urine.
Urinalysis: Osmolality measurements in plasma and urine – Osmolality serves as general marker of tubular function. Because the ability to concentrate the urine is highly affected by renal diseases. – This is conveniently done by determining the osmolality, and then comparing this to the plasma. – If the urine osmolality is 600 mosm/kg or more, tubular function is usually regarded as intact – When the urine osmolality does not differ greatly from plasma, the renal tubules are not reabsorbing water
Urinalysis: p. H and sediments • p. H - Urine is usually acidic • Urine sediments - Microscopic examination of sediment from freshly passed urine involves looking for cells, casts, fat droplets - Blood: haematuria is consistent with various possibilities ranging from malignancy through urinary tract infection to contamination from menstruation. - Red Cell casts could indicate glomerular disease - Crystals - Leucocytes in the urine suggests acute inflammation and the presence of a urinary tract infection.
Urinary casts • Are cylindrical structures produced by the kidney and present in the urine in certain disease states. • They form in the distal convoluted tubule and collecting ducts of nephrons, then dislodge and pass into the urine, where they can be detected by microscope.
Red blood cell cast in urine White blood cell cast in urine Urinary casts. (A) Hyaline cast (200 X); (B) erythrocyte cast (100 X); (C) leukocyte cast (100 X); (D) granular cast (100 X)
• Crystals Urinary crystals. (A) Calcium oxalate crystals; (B) uric acid crystals (C) triple phosphate crystals with amorphous phosphates ; (D) cystine crystals.
Can you identify the type of crystals in these images?
Diseases of the kidneys • RENAL DISORDERS 1. Acute renal failure 2. Chronic renal failure • PROTEINORIA AND NEPHROTIC SYNDROME • RENAL TUBULAR DISORDERS • Urinary calculi
ACUTE vs. CHRONIC RENAL FAILURE • Acute renal failure Is usually caused by an event that leads to kidney malfunction, such as dehydration, blood loss from major surgery or injury or the use of medication. • Chronic renal failure Is usually caused by a long-term disease, such as high blood pressure or diabetes, that slowly damages the kidneys and reduces their functions over time.
PROTEINORIA AND NEPHROTIC SYNDROME • Nephrotic syndrome is kidney disease with proteinuria, hypoalbuminemia, and edema. • Nephrotic-range proteinuria is 3 grams per day or more.
RENAL TUBULAR DISORDERS • There a variety of disorders of tubular function, both generalised and specific. • These disorders may be isolated defects, generalised tubular defects as in Fanconil’s syndrome, or associated with more generalized disease processes.
Types of renal tubular disorders • Fanconi's syndrome: • Renal tubular acidosis • Defects of urinary concentrations 1. Glycosuria 2. Amino aciduria
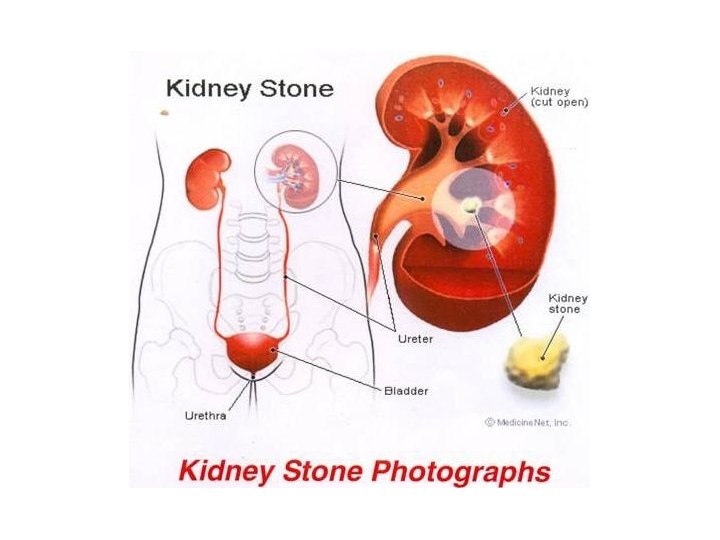
Urinary calculi • Stones or cacluli can form in urine when it is supersaturated with the crystalloid components of the calculus. 1. Hypercalciuria 2. Hyperoxaluria
Renal replacement treatment
Dialysis
Study case • An 8 -year-old girl was admitted to hospital with generalized oedema. Her urine had become frothy and has proteinuria. Investigations Serum Urea 2. 0 mmol/L (3. 3 – 6. 7) Creatinine 45 μmol/L ( 60 -120) Total protein 35 g/L (60 -80) Albumin 15 g/L (35 -50) Cholesterol 12 mmol/L (< 5 mmol/L) What is your diagnosis?
References • http: //kidney. niddk. nih. gov/kudiseases/pubs/you rkidneys/ • Marshall, W. and Bangert, S. (2008). Clinical chemistry (6 th ed. ). Edinburgh, London: Mosby Elsevier. ISBN 0723434557 (chapter 4) • Gaw, A. et al. (2004). Clinical Biochemistry (3 rd ed. ) • Beckett, G. et al. (2008). Clinical Biochemistry (8 th ed. ) • Bishop. , et al. (2000). Clinical Chemistry (4 th ed. )