The Joint Commission Whats New 2019 Objectives Participant

The Joint Commission: What’s New 2019

Objectives � Participant can name new standards or new interpretations related to GI area of practice � Participant will identify current hot topics � Participant will identify areas that are cited the most frequently � Participant will be able to identify Joint Commission resources that are available

AGENDA � Navigating the TJC Web Site � What’s New ◦ ◦ ◦ Scoring Methodology Sentinel Event Alerts Standards Interpretive Guidelines Frequent Findings/Low Hanging Fruit � Question & Answer

Joint Commission – OH NO!

What Drives Joint Commission Standards? Joint Commission’s Vision Statement: � All people always experience the safest, highest quality, best-value health care across all settings

Unannounced Survey Process � Majority of organizations are expected to be surveyed in the year their routine full survey is due � Recent CMS Mandate: ◦ 50% of organizations should be surveyed up to 5 -6 months earlier than triennial date ◦ Less than 10% to be surveyed in their due month � CMS is piloting and evaluating a new validation survey process for future using a concurrent survey rather than post

It is not about getting ready for the survey…but always being ready for the next patient.

New Scoring Methodology 1/1/17

Navigating TJC Website
")
Chapter, Standard, Element of Performance (EP)

Sentinel Events

Sentinel Event �A sentinel event is a patient safety event (not primarily related to the natural course of the patient’s illness or underlying condition) that reaches a patient and results in any of the following: ◦ Death ◦ Permanent Harm ◦ Severe temporary harm

Sentinel Events � Fall 2018 TJC updated sentinel event classifications – the highest level grouping: ◦ ◦ ◦ ◦ ◦ Anesthesia-related events Care management events Criminal events Environmental events Product or device events Protection events Suicide – ED Suicide – inpatient Suicide – offsite within 72 hours of DC Surgical or invasive procedure events

Recent Sentinel Event Alerts � #61: Managing the risks of DOACS… � #60: Developing a reporting culture… � #59: Physical and verbal violence against healthcare workers � #58: Inadequate Hand-off Communication #57: Essential role of Leadership in Developing Culture of Safety � #56: Detecting and treating suicide ideation in all settings
 -published July")
Sentinel Event Alert #61: Managing the risks of direct oral anticoagulants (DOACs) -published July 30, 2019 DOACs Include: • • • Apixaban (Eliquis) Betrixaban (Bevyxxa) Dabigatran (Pradaxa) Edoxaban (Savaysa) Rivaroxaban (Xarelto) Clinicians may not always recognize these names as anticoagulants. DOACs are very different than warfarin & heparin in dosing, monitoring, and treatment of complications.

New Standards New Elements of Performance

Culture of Safety Survey � Increased focus on results and action plan � Day One review � Included in Individual and System Tracers

Surveyor Questions for Staff regarding Safety Culture � Have you completed a safety culture survey? Have you seen the results? Does your supervisor discuss the results? � Does leadership conduct root cause analyses of “close calls/near misses” that are reported? ◦ What process is in place for reporting these? � When an error occurs, do you have confidence that leadership will take an appropriate look at how the system or process in accountable versus an individual?

Pain Management Standards � Opioid Use / Abuse � Huge Focus ◦ New Standards �Heavy on Leadership ◦ R 3 report ◦ PI monitoring related standards

Fluoroscopy: Effective Jan 1 2019 � NOT just in the Radiology Department � PC. 02. 01; The hospital provides care, treatment, and services for each patient ◦ 30. Fluoroscopy skin exposure review requirements. � PI. 02. 01; data The hospital compiles and analyzes ◦ 20. Review excess fluoroscopy exposures

Workplace Violence in Healthcare Joint Commission recommendations 1. 2. 3. 4. 5. 6. 7. Clearly define workplace violence…enable staff to report…including verbal abuse Recognize data comes from multiple sources – capture, track & trend all Provide appropriate f/u & support Review each case…to determine contributing factors Develop quality improvement initiatives Train all staff in de-escalation, self defense & emergency response Evaluate workplace violence reduction initiatives Source: Joint Commission Sentinel Event Alert, Issue 59, April 17, 2018
:")
Removal of Smoking Materials EC. 02. 01. 03 � New Element of Performance (EP): 1/1/18 � EP 4: Smoking materials are removed from patients receiving respiratory therapy. ◦ When a nasal cannula is delivering oxygen outside of a patient’s room, so not sources of ignition are within the site of intentional expulsion (within 1 foot). When other oxygen delivery equipment is used or oxygen is delivered inside a patient’s room, no source of ignition are within the area of administration (within 15 feet)…

Newborn Naming Added to NPSG 01. 01 � Use distinct methods of identification for newborn patients

Recently an expiration date has been added to new Ambu Bags. If you have one that does not have this date they are good for five years or until they feel “tacky” (which ever comes 1 st).
 ◦ Texting of")
Text Messaging � CMS Survey & Certification Letter 18 -10 (1/5/18) ◦ Texting of patient information between members of the care team IS permissible IF accomplished through a SECURE platform ◦ Texting of patient ORDERS is PROHIBITED regardless of the platform used �CPOE is the preferred method of entry of orders by a provider

New Interpretations Same Ole’ Standards

Oxygen Storage CHANGE - AGAIN 2/28/18 - FAQ EMPTY cylinders shall be segregated from all other cylinders that are intended for patient care use.

EXAMPLE

NFPA 99 -2012: 15: 13 Flammable germicides/antiseptics used during surgeries utilizing electrosurgery, cautery, or lasers the following are required: � Nonflammable packaging � Unit-dose applicators � Preoperative “time-out” prior to the initiation of any surgical procedure to verify the following: ◦ Application site is dry prior to draping & use of surgical equipment ◦ Pooling of solution has not occurred or has been corrected ◦ Solution-soaked materials have been removed from the operating room prior to draping & use of surgical devices

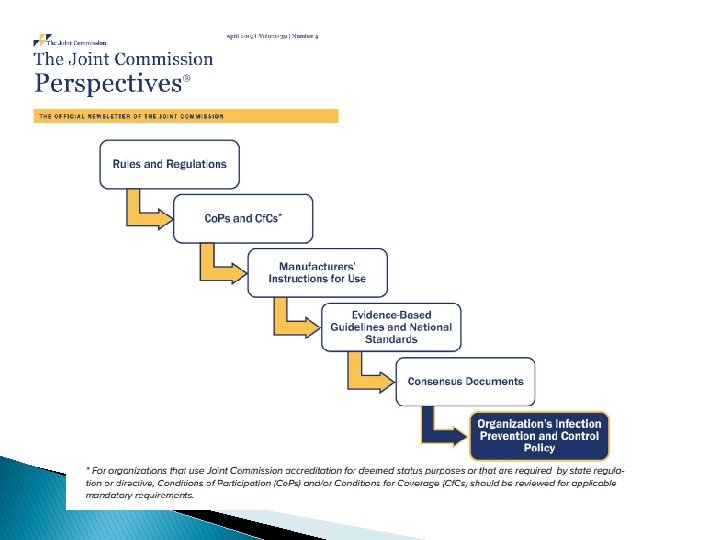
Policies & Evidence Based Guidelines � Joint Commission will hold the organization to their policy – EVEN – if the policy is more stringent than the requirement. � Educate your staff on what Evidence Based Guidelines your area uses – do not let them spout “alphabet soup” when the surveyor asks them.

Endoscopy Risk Areas Focus

Google Search � Outbreak related to endoscope cleaning ◦ 404, 000 results � Endoscopy ◦ 6, 490, 000 related infections

Endoscopy focus � Competencies � High Level Disinfection � Medication Management � Infection Control practices ◦ Hand Hygiene � Environmental safety � Manufacturer’s Guidelines � Post procedure physician documentation

Competency vs Education & Training � Education is the process of receiving systematic instruction resulting in the acquisition of theoretical knowledge. � Training differs in that “training” focuses on gaining specific – often manually performed – technical skills. � Competency requires a third attribute – ability. Ability is simply described as being able to “do something”. The ability to do something “competently” is based on an individual’s capability to synthesize and correctly apply the knowledge and technical skills to a task. Source: Joint Commission Standards FAQ

Competency vs Education & Training � Competency differs from education and training in that competency incorporates all three attributes. ◦ Knowledge, technical skills, and ability – all are required to deliver safe care, correctly perform technical tasks, etc. Assessing competency, then, is the process by which the organization validates, via a defined process, that an individual has the ability to perform a task, consistent with the education & training provided. Source: Joint Commission Standards FAQ

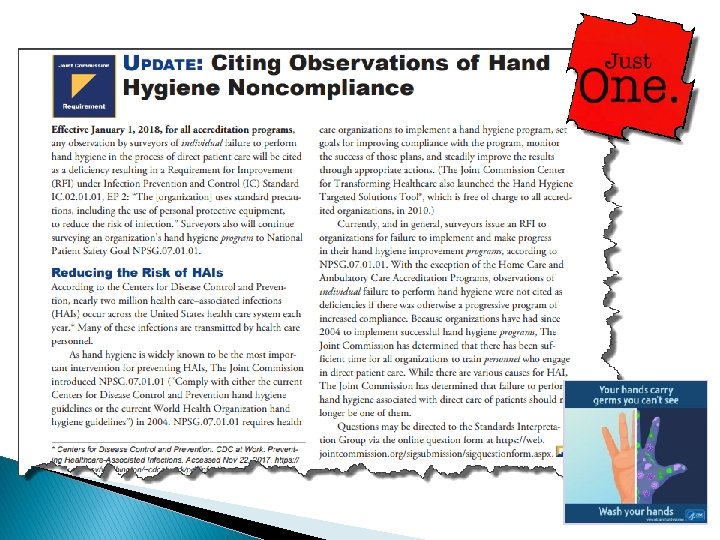
Infection Control Risk Points � HAND HYGIENE � Staff unable to speak to LLD/HLD process � Not following IC policies/procedures � Identification of clean vs dirty � Storage on the floor, under the sink, bottom shelf with no solid liner � Mixing clean and dirty items � Adherence to infectious precautions (contact, airborne, droplet)

� Infection Prevention & Control Medical Equipment, Devices & Supplies IC. 02. 01 Implement infection prevention and control activities related to: ◦ EP 1 Cleaning and performing low-level disinfection ◦ EP 2 Performing intermediate and high-level disinfection and sterilization ◦ EP 3 Disposing of medical equipment, devices, and supplies ◦ EP 4 Storing medical equipment, devices, and supplies Standards Spaulding Classification
 � Manufacturer’s ◦ ◦ ◦ Recommendations Posted; Current Cleaning PPE")
High Level Disinfection (HLD) � Manufacturer’s ◦ ◦ ◦ Recommendations Posted; Current Cleaning PPE Policies and Procedures Written �Includes preventive maintenance, storage, cleaning, processing, handling, transport, documentation �Disinfection and cleaning product instructions for use, testing, and maintenance

HLD Continued � Cleaning and Processing areas ◦ Decontamination and cleaning in negative vented room ◦ Dirty to clean ◦ Designated area for processes and placement � Endoscope processing ◦ Point of Use �Immediate Pre-cleaning �Wipe and flush with enzymatic detergent/water – manufacturer? ◦ Transport �In a container to prevent environmental contamination �Labeled as biohazardous �Based on manufacturer’s instructions and evidence based guidelines

IC. 02. 01: New Interpretive Guidelines � The hospital reduces the risk of infections associated with medical equipment, devices, and supplies • Sterile Medication Compounding • Suicide Prevention • High Level Disinfection and Sterilization • Renal Dialysis

Recent Webinar Available https: //www. jointcommission. org/disinfection_and_sterilization_dispelling_myths/

IC: High Level Disinfection October 2018 PERSPECTIVE S: Pages 12 - 21
 Bags in Advance of Administration Once an IV")
Medication Preparation - Spiking Intravenous (IV) Bags in Advance of Administration Once an IV bag of fluid is spiked with the IV tubing, how soon must this infusion be initiated ? � The infusion must be started within 1 hour of spiking the bag unless the bag was spiked in an ISO 5 environment. ◦ When a bag is spiked and the infusion is immediately begun, the spiking of the bag is considered part of the administration process. ◦ If the bag is spiked and then stored for later use, it is considered to be a part of preparation. � If the bag is spiked in an ISO 5 environment, then beyond use dating would be consistent with those listed in the USP 797 Chapter. TJC Standards FAQ published 8/20/2019

Universal Protocol should be hard wired by now -Don’t forget to add the removal of fluid soaked materials prior to draping If Time-Outs are always completed properly there would be NO wrong side/site surgery/procedures

National Patient Safety Goals NPSG. 01. 01 Patient Identification Use at least two patient identifiers when providing care, treatment and services: � FIRST: Identify the person for whom the test or procedure is intended for AND � SECOND: Match the intended service or treatment to that person Label containers used for blood and other specimen in presence of patient

NPSG. 03. 04. 01 Medication Safety: Labeling � Label all medications, medication containers, and other solutions on and off the sterile field: Label when not immediately used Label even if only ONE medication/solution Label at time of transfer Include medication/solution & strength Include expiration date/time, IF applicable Verification process, especially if the one preparing is NOT the one administering and when change of staff ◦ Immediately discard any meds found unlabeled ◦ ◦ ◦

Frequent Findings AND Low Hanging Fruit

High Level Disinfection & Sterilization � Not following manufactures guidelines or Advancing Safety in health Technology Guidelines (AAMI) � Enzymatic cleaning agent not used on dirty instruments at end of procedure (multiple locations) � No process for assuring proper soaking, washing, and rinsing � Biological indicators during Immediate Use Steam Sterilization not being logged � No documentation of lot numbers of Rapicide test strips � Leakage testing not being completed � Visual reading for controls was documented as negative and should be positive

Storing Medical Supplies/Devices � Expired laryngeal airway found � Dirty & clean patient supplies stored together � No process for cleaning/disinfecting the inside of bronchoscope carrying cases � Components of the valve assembly (multiple sets) stored inside a drawer after disinfection without any protective covering � Airway exchange devices & bougies on top of cart – removed from original packaging without being wrapped or protected from cross contamination

Environment of Care: EVERYONE’s Responsibility No stained ceiling tiles!

Summary � Don’t focus on survey prep – be always ready � Surveys truly more unannounced � Endoscopy ◦ ◦ ◦ ◦ is a high focus area Evidence Based Guidelines High Risk Medications High volume of Infection Control issues High Level Disinfection processes Multiple kinds of scopes and equipment Manufacturer’s Use Guidelines Competencies are Key

QUESTIONS?

60

Lynn Smith, MHA, BSN, CPQH Senior Director Performance Improvement North Kansas City Hospital Lynn. smith@nkch. org 816. 691. 5335

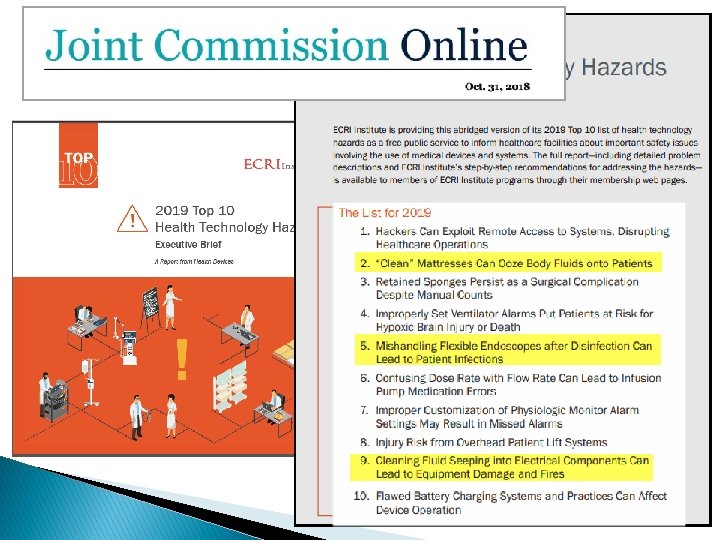
References � Joint Commission website � Joint Commission E-dition � Joint Commission Perspectives � Joint Commission presentations � Joint Commission newsletters � Joint Commission Sentinel Event Alerts � ECRI Institute: 2019 Top 10 Health Technology Hazards Executive Brief
- Slides: 61