The Heart Circuits Chambers Valves onewayflow Myocardiocytes Volumes
 • Myocardiocytes")
The Heart • Circuits • Chambers • Valves (one-way-flow) • Myocardiocytes

Volumes? Pressures? heart –> lungs –> heart –> body –> heart Artery = Vein =

Trace a RBC!

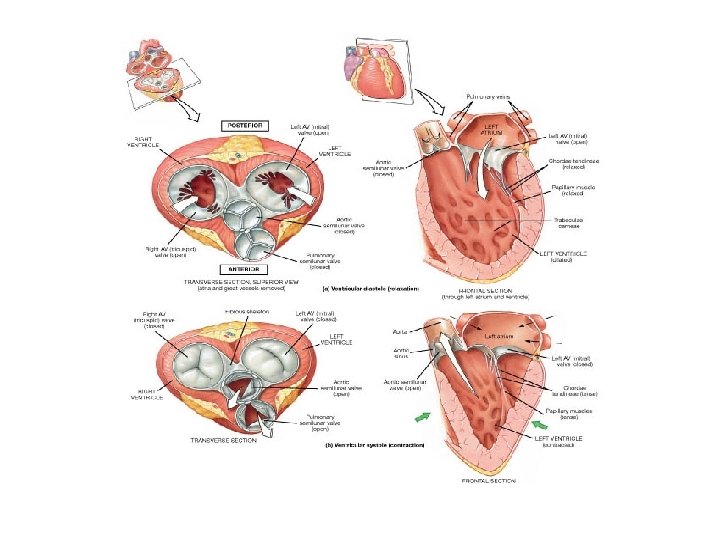
The Heart has 4 Valves To prevent retrograde flow of blood. 2 atrioventricular valves (AV) between the atria and ventricles. 1) Right AV (tricuspid) valve 2) Left AV (bicuspid/mitral) valve
 Aortic semilunar valve 2) Pulmonary")
2 semilunar valves between a ventricle and artery. 1) Aortic semilunar valve 2) Pulmonary semilunar valve Two heart sounds: “Lub” and “Dup” 1. Closure of AV valves = “Lub” 2. Closure of Semilunar valves = “Dup” http: //www. openheartsurgery. com/heart_murmur. html

Disorders of Heart Valves Normal Heart Valves Problems Opening: Stenosis – narrowing of valve, when a valve doesn't open completely. Turbulence = noise = murmur. Problems Closing: Prolapse –overlapping or when valve doesn't close tightly. Also termed valvular insufficiency (regurgitation) Retrograde flow = noise = murmur.
 Autorhythmic 2) Contractile")
Myocardiocytes: 1) Autorhythmic 2) Contractile

Action Potentials for Autorhythmic Myocardiocytes

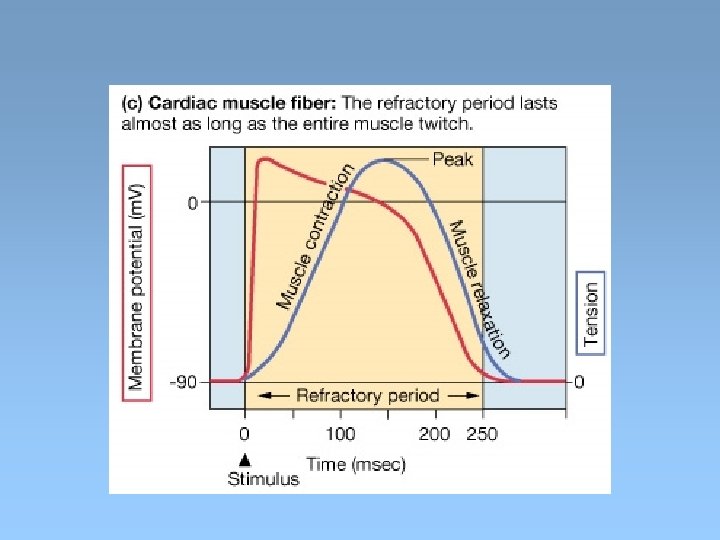
Action Potentials for Contractile Myocardiocytes stimulus

Myocardiocytes: Calcium induced Calcium release

Graded Contraction of Heart Force generated by myocardiocyte contraction is: 1. Proportional to amount of Calcium ions (Ca 2+) [Ca 2+] => more crossbridges, more force & speed.

Graded Contraction of Heart Force generated by myocardiocyte contraction is: 1. Proportional to amount of Calcium ions (Ca 2+) [Ca 2+] => more crossbridges, more force & speed. 2. Modulated by Autonomic N. S. => Sym HR and Force => Para HR

Sympathetic – speeds heart rate by Ca 2+ influx. Parasympathetic – slows rate by K+ efflux, Ca 2+ influx.

Graded Contraction of Heart Force generated by myocardiocyte contraction is: 1. Proportional to amount of Calcium ions (Ca 2+) [Ca 2+] => more crossbridges, more force & speed. 2. Modulated by Autonomic N. S. => Sym HR and Force => Para HR 3. Stretch-Length-Tension Relationship stretch, => Ca 2+ entering => contraction force

Factors Influencing Stroke Volume

The Cardiac Cycle http: //www. youtube. com/watch? v=rguzt. Y 8 aqpk

The Cardiac Cycle: Mechanical Events of the Heart 1. Late Diastole: “Heart at rest” all chambers relaxed filling with blood (passive filling ~ 80% full). 2. Atrial Systole: atria contract, adds the last 20% of blood to ventricles (top off ventricles) Occurs after P-wave on EKG End Diastolic Volume (EDV) = Maximum ventricular volume*
: Ventricular contraction begins - Pressure (P). Closure of AV")
3. Ventricular Systole (part 1): Ventricular contraction begins - Pressure (P). Closure of AV valves = 1 st heart sound ("lub") Sealed Compartment – all valves are closed. Isovolumetric ventricular contraction: => pressure builds as volume stays the same.
: Ejection phase: P pushes open semilunar valves, blood forced")
4. Ventricular Systole (part 2): Ejection phase: P pushes open semilunar valves, blood forced out into artery leaving ventricle. Pulmonary Semilunar => 25 mm. Hg (minimum pressure) Aortic Semilunar => 80 mm. Hg (minimum pressure) End Systolic Volume (ESV) = volume remaining in heart after ejection (~½)*. Stroke Volume = EDV - ESV (ml/beat)

5. Ventricular Diastole: Relaxation of ventricles, artery back flow slams semilunar valves shut = 2 nd heart sound ("dup"). Sealed Compartment again – all valves are closed. Isovolumetric ventricular relaxation: => pressure as volume stays the same. The AV valves then open, refilling starts – back to start of cycle.
 = Heart Rate x Stroke Volume *Heart Rate =")
Cardiac Output (C. O. ) = Heart Rate x Stroke Volume *Heart Rate = beats/min *Stroke Volume = EDV-ESV (vol/beat) e. g. calculation:
 Node Atrial Ventricular (AV) Node AV Bundle (of")
Electrical Conduction System Sino Atrial (SA) Node Atrial Ventricular (AV) Node AV Bundle (of His) L and R Bundle Branches Purkinje Fibers
")
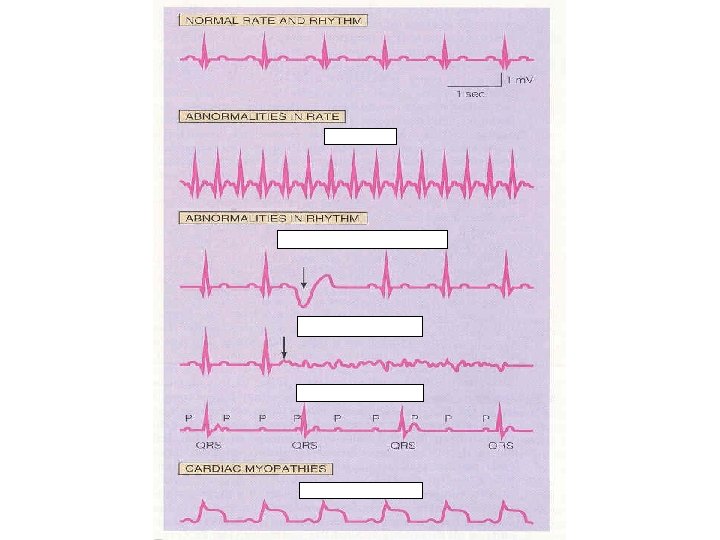
Trace of an Electro. Cardio. Gram (ECG)

The ECG P wave: PR interval: QRS complex: T wave:

Ventricular Assist Devices http: //www. youtube. com/watch? v=D 3 ZDJg. FDdk 0
- Slides: 29