The gut Microbiome an introduction NZCOM website version

The gut Microbiome an introduction NZCOM website version Celia Grigg Midwife & Research Fellow October 2019 Image by Lorraine Renee Skuta

Summary • Definition • Roles • Influences • Impact on health and disease • Influences on neonatal microbiome • Breastfeeding microbiome • Mode of birth • Articles hyperlinked and open access ‘Germs are us’ – The New Yorker
, viruses, eukaryotes")
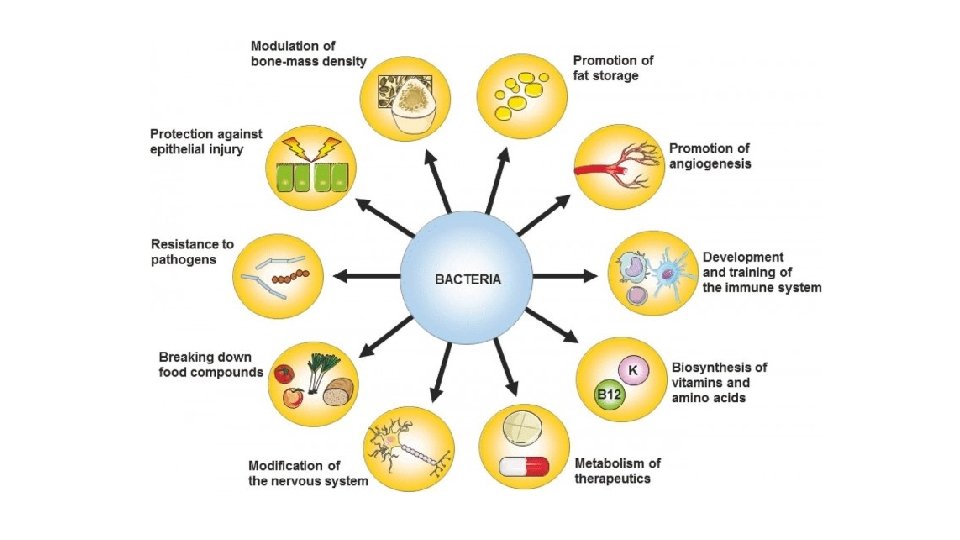
Definition of microbiome Background: Functions: Establishment affected by: • Bacteria (≥ 60%), viruses, eukaryotes (eg fungi), archaea • Metabolism and biosynthesis eg SCFA, cytokines • Human genome • Maternal diet • Mode of birth • Antibiotics • Timing of birth • NICU admission • Infant diet • Environment • Gut largest reservoir (≥ 30 genera & 500 species) • Symbiotic - they help us & we need them & Gut Assoc Lymphoid Tissue - Carbs, fibre; certain drugs, vitamins & minerals • Immune system development and regulation • Gut-brain axis – neurological dev. & function • Composition – richness & diversity important - not just about individual or ‘flag’ types • Protection from pathogens and disease • Epithelial development & maintenance

Source: Chong, Bloomfield, O’Sullivan Factors affecting Gastrointestinal microbiome development in neonates. Review. Nutrients 2018, 10: 274 (Some graphics edited by CG)
")
Human microbiome - called ‘second genome’ - Actively interacts with human genome (via metabolites) leading to far-reaching epigenetic modifications Epigenetics - ‘on top of genetics’ - Processes that cause miotically and meitotically heritable changes in the gene expression without modifying DNA. Source: Epigenetic matters: the link between early nutrition, microbiome & long-term health development. Indrio et al Frontiers in Pediatrics. Review 2017
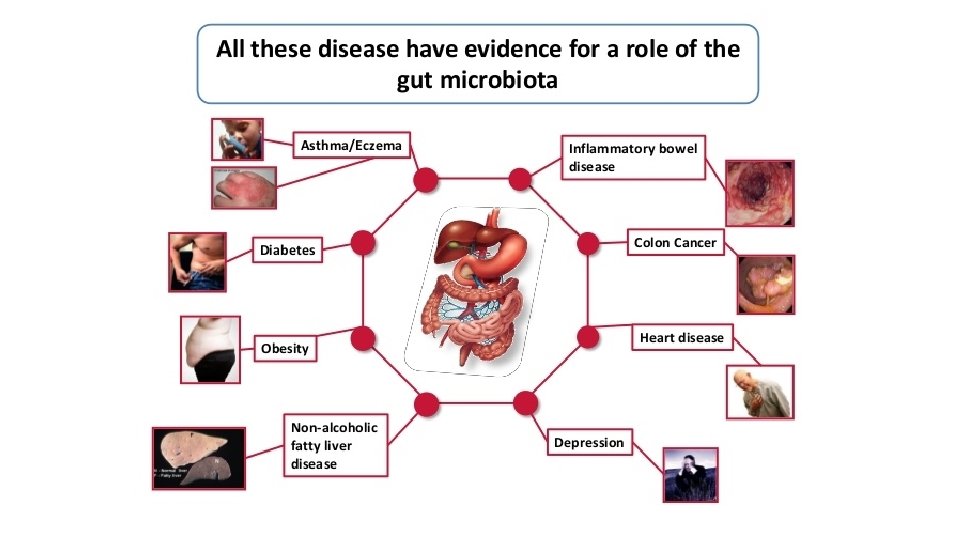

Impact on health and disease • Associations with multiple conditions known • Few mechanisms fully understood • Early days in research, but lots being done • Type 1 diabetes – breastfeeding known to be protective • It is gut bacteria which is protective • action of strain-specific genes which can utilise human milk oligosaccharides (Bifidobacterium longum) (Vatanen et al TEDDY study Nature 2018) • Allergy - Ig. A most abundant & impt antibody for mucosal immunity • Luminal secretory Ig. A binding to selected bacterial antigens 1 st step in maintenance of immune exclusion - production scarce in babies – rely on maternal via breastmilk - abnormal Ig. A responses in 1 st yr associated with allergy & asthma at 7 yrs. (Mezouar et al Microbiome & immune system Human Microbiome J 2018)

Birth as a unique moment • Likely first exposure to live bacteria • Some debate about sterility of womb, but not robust evidence that it’s not sterile (for a good review of the evidence see Perez-Muňoz et al Microbiome 2017: 5: 48 • Vaginal birth provides initial ‘probiotic shower’ with key bacteria for gut microbiome • When immune system ‘naïve’ and needing programming – bacteria types doing this can influence how it functions long term (genomic and epigenetic effects) • Babies stomach is ph neutral for 2 -3 hours after birth • Due to amniotic fluid • Enables ‘right’ or optimal bacteria to get into intestine • It then becomes acidic – which kills many bacteria coming later • Colostrum contains oligosaccharides • which the baby cannot absorb, but the bacteria from normal birth can absorb • our systems really want these bacteria to set up camp in the gut!!
 • Timing")
Influences on neonatal microbiome • Maternal diet • Antibiotics (antenatal, intrapartum, postnatal) • Timing of birth (preterm) • Mode of birth • Mode of feeding • NICU • Environment (rural/urban)

Breastfeeding microbiome • Under researched – still lots not known • Increased abundance of Staphylococcus (neonates) and Bifidobacterium and Lactobacillus (infants) • Wide variation – eg age of baby and lifestyle • Other constituents very important in multiple roles, some supporting microbiome: • Human Milk Oligosaccharides (HMOs) Recent Swedish study • 98 mothers and babies -> 12 mths • Differences between exclusive breastfed and formula fed babies microbiome, but functional difference very small (1. 30% of variation) • Cessation of b/f ‘had profound effect on microbiome in 12 mth olds’ – not intro of solids • 3 rd largest component • Prebiotic – can feed certain ‘good’ bacteria (Bacteroides and some types of Bifidobacteria) but not ‘bad’ bacteria (Enterobacteriaceae) Bäckhed et al Cell Host & Microbe 2015; 17: 690 -3
")
Stunted microbiota & opportunistic pathogen colonization in CS birth Shao et al (Sep 2019) Nature https: //doi. org/10. 1038/s 41586 -019 -1560 -1 (Open Access) Fig 2 a, Bar plot illustrating the clinical covariates that are associated with variation in the neonatal gut microbiota on day 4 (n = 310 individuals), day 7 (n = 532 individuals), day 21 (n = 325 individuals) and in infancy (n = 302 individuals, at 8. 75 mths +/-1. 98 mth). Only significant associations in cross-sectional tests are shown.

Mode of Birth and microbiome Fig 2 b, Longitudinal changes in the mean relative abundance of genera of faecal bacteria, sampled on day 4, 7 & 21 and infancy (8. 75 mths+/-1. 98), for genera with >1% mean relative abundance across all samples from the neonatal period. Vaginal births, n =744 samples from 310 babies; caesarean section births, n=725 samples from 281 babies. Source: Shao et al (Sep 2019) Stunted microbiota & opportunistic pathogen colonization in CS birth. Nature https: //doi. org/10. 1038/s 41586 -019 -1560 -1
 study 22, 068 offspring Prospectively followed from")
Caesarean section associated with obesity GUTS (USA) study 22, 068 offspring Prospectively followed from 1984 - 23% increase in rate of childhood obesity - 64% higher obesity rate within family (sub-group 12, 903 CS vs VB siblings) Adjusted for: - Maternal age - Pre-pregnancy BMI - Gestational diabetes - Birth weight - Previous LSCS - Sex of infant - Year of birth Yuan et al JAMA Pediatr 2016; 170(11): 1 -8 - Ethnicity - Pre-eclampsia - PIH - Smoking - Maternal height - Birth order - Region

Caesarean section and offspring allergic disease and chronic immune disorders • Allergy • Two Meta-analyses (2008) Bager P Clin Exp Allergy 2008 Apr; 38(4): 634 -42. Thavagnanam S Clin Exp Allergy 2008 Apr; 38(4): 629 -33 • • Food allergy (OR 1. 32) – 32% increase associated with CS birth Allergic rhinitis (OR 1. 23) Asthma in childhood (OR 1. 2) – 20% increase associated with CS birth Hospitalisation with asthma (OR 1. 2) • Chronic Immune disorders • Large population based cohort (2 million children, 35 yr->2012, Denmark) Sevelsted et al Pediatrics 2015; 135(1): e 92 • • • Asthma a. IRR 1. 23 Immune deficiencies 1. 46 IBD 1. 20 Leukaemia 1. 17 (p=. 048) Systemic connective tissue disorders 1. 11 Juvenile arthritis 1. 10

Caesarean section: partial restoration of microbiota - Research highlighted in Microbirth movie: Bacteroides Maternal vaginal swab to baby mouth, face, skin Lactobacillus N=7 N=4 30 days follow-up baby oral, skin and anal swab No faecal samples Current Auckland ECOBABe study aimed to collect evidence to see if we can get the right bacteria in the right place at the right time. N=4 N=7 So there is an extremely limited evidence base informing current vaginal seeding practice!! N=7 Dominguez-Bello et al Nature Medicine 2016; 22: 250 -3

Contact details Celia Grigg Email: celia. grigg@xtra. co. nz Mobile: 021 268 2128 Email: c. grigg@auckland. ac. nz or ecobabe@auckland. ac. nz Mobile: 027 606 5140 Google: ‘ECOBABe study’ for website

The following slides have been added for the website and were not presented at the NZCOM regional meeting. They give you more information about the ECOBABe vaginal seeding study underway in Auckland region. Feel free to contact me if you’d like more information, pamphlets/posters or if you want me to visit your practice meeting to discuss it.
 Elective LSCS (≥ 37")
80 women carrying singletons – Auckland region (ADHB, CMH, WDHB) Elective LSCS (≥ 37 wks, no diabetes, ‘well baby’) Vaginal swab inserted 30 mins prior to CS Swab mixed with sterile water for treatment (1/2 saved for sequencing) Randomised to treatment with maternal vaginal secretions or placebo 40 women carrying singletons - vaginal birth (reference group, untreated) Antenatal diet preferences and 3 day activity/exercise diary Antenatal screening for CS group (Liggins – incl GBS, Chlamydia, Hep, HIV, Tric, HSV etc) 16 s amplicon sequencing of: - maternal secretions, infant stools at <48 hrs, 1 mth, 3 mths Feeding mode, infant’s medical history (eg NICU admission) at <48 hrs, 1 mth, 3 mths Plan for later follow-up infant anthropometry and allergic diseases

https: //www. auckland. ac. nz/en/liggins/in-the-community/clinicalstudies/clinical-studies-pregnancy/ecobabe-study. html Feel free to copy the above woman’s jpeg file and add the hyperlink, for sending electronically to women.
- Slides: 21