The growing role of CDK 4 6 inhibitors

The growing role of CDK 4 -6 inhibitors in therapeutic strategy of metastatic breast cancer: how to choose? Dott. Katia Cannita UOC Oncologia Medica Università degli Studi L’Aquila

• Estrogen is involved in the pathogenesis of breast carcinoma • Estrogen sustains the growth of breast cancer cells that express the receptor for this hormone • 75% of Breast cancer (BC) patients are ER+ and/or Pg. R +
 and progesterone receptor (PR) expression are currently the best predictors of")
Estrogen receptor (ER) and progesterone receptor (PR) expression are currently the best predictors of response to endocrine therapy in the clinical setting. However, 25% of ER+/PR+ tumors, 66% of ER+/PR– tumors, 55% of ER–/PR+ tumors fail to respond to tamoxifen or develop early resistance to tamoxifen for reasons that are unclear ( Moy and Goss, Clin canc res’ 06).
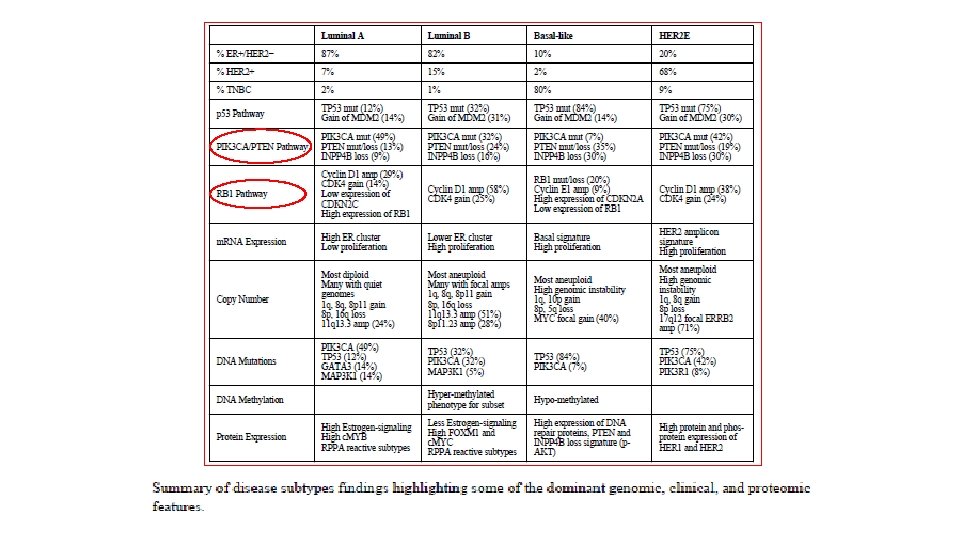

The role of CDK 4/6 in Breast Cancer I. A. /Fulvestrant ER/Pg. R • Cyclin D–CDK 4/6 complexes ciclib NF-k. B Pl 3 K/m. TOR p 5 3 p 21 MAPKs STATs Wnt/β-catenin p 16 Rb G 1 E 2 F M G 0 Restriction Spoint E 2 F • • promote cell proliferation through Rb protein phosphorylation 1 Increased CDK 4/6 activity is frequently observed in HR+ breast cancer 1, 2 Activation of the cyclin D–CDK 4/6– INK 4–Rb pathway has been associated with poor response and resistance to endocrine therapy 1, 2 G 2 1. Hosford S, Miller T. Pharmgenomics Pers Med 2014; 7: 203– 215; 2. Thangavel C, et al. Endocr Relat Cancer 2011; 18: 333– 345; 3. Kim S, et al. Mol Cancer Ther 2013; 12(Suppl 11): abst PR 02 (oral). CDK, cyclin-dependent kinase; HR+, hormone receptor-positive; INK 4, inhibitor of CDK 4; Rb, retinoblastoma.

Treatment for HR+, HER 2– Advanced Breast Cancer Recent Advances and Upcoming Therapies

HR+, HER 2─ Advanced Breast Cancer: Where Are We Now? • Investigations into CDK 4/6 inhibition in combination with endocrine therapy have significantly altered the treatment landscape for patients with HR+, HER 2─ ABC 1 ─ In the first-line setting, the addition of CDK 4/6 inhibitors to endocrine therapy significantly improves PFS, ORR, and CBR versus endocrine therapy alone 2 ABC, advanced breast cancer; ABE, abemaciclib; CBR, clinical benefit rate; CDK, cyclin-dependent kinase; ET, endocrine therapy; FUL, fulvestrant; HER 2–, human epidermal growth factor receptor-2–negative; HR, hormone receptor; LET, letrozole; NSAI, nonsteroidal aromatase inhibitor; OFS, ovarian function suppression; PAL, palbociclib; PBO, placebo; PFS, progression-free survival; RIBO, ribociclib. 1. Ramos-Esquivel A, et al. Breast Cancer. 2018. doi: 10. 1007/s 12282 -018 -0848 -6 [Epub ahead of print]; 2. clincialtrials. gov.

How and When to incorporate CDK 4/6 Inh in the managemenet of HR+ MBC Remain one the main unmeet clinical need in this setting ? ? ? ET naive Non visceral disease Long DFI CIRS, old patient with no good caregiver

Ciclibs: NOT if but when Tamoxifen 105€ year Letrozole 880€ year Fulvestrant Ciclibs 6. 000€ year 25. 000€ year . . . it is clinically necessary, scientifically wrong, ethically acceptable and financially sustainable to prescribe everything to everyone. . . Davis C et al. BMJ 2017; 359: j 4530; Cancerworld Spring 2018; 4 -11; Zhang B et al. Breast Cancer Res Treat 2019; epub ahead of print

LG AIOM 2019 Palbo o Ribo o Abema+ NSAI Fulvestrant I. A. Palbo o Abema + Fulvestrant Everolimus + exemestane Fulvestrant Ripresa di malattia tardiva > 12 mesi dal termine adiuvante Precedente esposizione a Terapia endocrina in adiuvante SI Ripresa di malattia precoce < 12 mesi dal termine dell’adiuvante o in corso di adiuvante I line II line

HOW TO CHOOSE?
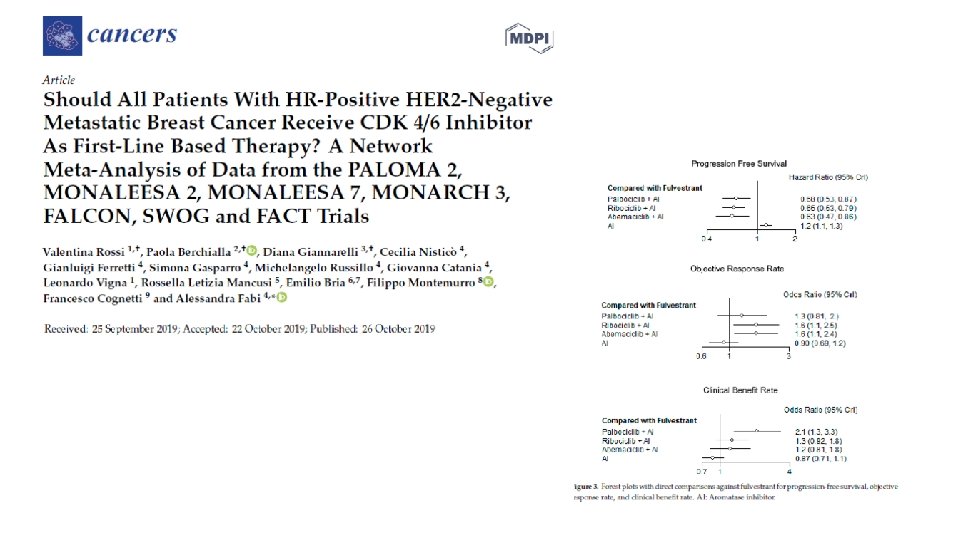

Conclusions: CDK 4/6 produced significant improvement in PFS, CB, ORR in all pts The results are indipendent of age, race, PS, Disease site, prior Ct or ET Indipendent of menopausal status, DFI, CDK 4/6 Inhibitor, and Pg. R expression Improvement of PFS in favor of CDK 4/6 inh even in pts with bone only disease or in non visceral disease

CDK 4/6 Inh Trials In First Line Setting • PALOMA 2 • MONALEESA 2 • MONARCH 3 HOW TO CHOSE ? Premenopausal status • MONALEESA 7

…. . Are the treated populations similar? PALOMA 2 % MONALEESA 2 MONARCH 3 22. 3 < 12 mo from adj 1. 2 >12 – <24 mo 4. 2 MONALEESA 7 Endocrine resistant < 12 mo from adj DFI ( from diagnosis) </=12 mo 7 Endocrine sensitive DE NOVO 37. 6 > 12 mo from adj 34. 1 > 24 mo 40. 1 41. 2 >12 mo from adj 60. 5 40 DFI From diagnosis >12 mo <36 mo 28 >36 mo 62 53

Prospective view Endocrine sensitive % Primary endocrine resistant % Median PFS Paloma 2 77 22 27. 6 Monaleesa 2 94. 6 5. 4 25. 3 Monaleesa 7 93 7 23. 8 Monarch 3 100 28. 2

Monaleesa 7: the only phase III focused in premenopausal Overall Survival • ≈ 29% relative reduction in risk of death • The P value of. 00973 crossed the prespecified boundary to claim superior efficacy Events/N Median OS, mo HR (95% CI) P value Ribociclib + ET Placebo + ET 83/335 109/337 Not reached 40. 9 Landmark Analysis Kaplan-Meier Estimate Ribociclib + ET Placebo + ET 0. 712 (0. 535 -0. 948) 36 months 71. 9% 64. 9% . 00973 42 months 70. 2% 46. 0% Dr Sara Hurvitz 18

Monaleesa 7 Overall Survival Subgroup Analysis • Consistent OS benefit seen within subgroups a In patients with no prior chemotherapy in the metastatic setting. 19

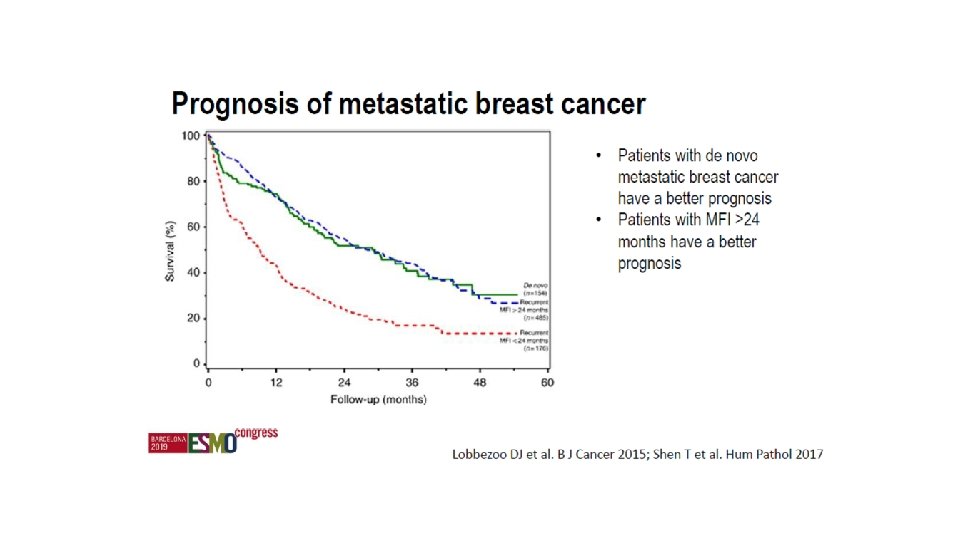
Patient populations in trials and OS



Results for Sensitive vs Non sensitive pts

")
HOW to CHOSE Molecular mechanism: Abema inhibitor of CDK 2/ciclin E/A (resistance in palbo) Activity in p. RB deficient Profile toxicities

Registrative trials CDK 4/6 inhibitors Main toxicities % G 3 -G 4 neutropenia % Diarrhea % G 3 -G 4 AST and/or ALT elevation % G 1 -G 4 creatinine elevation % QTc. F interval increase (>60 msec) % Thromboembolic events Palbociclib* Ribociclib** Abemaciclib*** 66 59 21 1(G 3) 36(G 2=27/G 3=9) 3 9 7 NR NR 19 (G 3/G 4=2/0) <1 3 NR 1 3 5 *Finn RS et al New Engl J Med 2016; **Hortobagyi G et al, New Engl J Med 2016; ***Goetz MP t al, J Clin Oncol 2017


Potential drug‐drug interactions with palbociclib and ribociclib © 2017 by Alpha. Med Press Laura M. Spring et al. The Oncologist 2017; 22: 1039 -1048

Abemaciclib Month 1 Complete blood count Liver function tests Diarrhoea Month 2 Months 3– 4 Months >4 Day 1 Baseline Day 14 Day 1 • • • Patients advised to monitor throughout Venous thromboembolism and Monitor throughout treatment pulmonary embolism As clinically indicated • •

Conclusions HOW CHOSE? Trials cannot be compared • Different population • Different subgoup Profile of toxicities Drug interaction Patients preferences are probably the only parameter for decision making process

Conclusions • Endocrine sensitive + bone only : Palbociclib and Ribociclib ? • Endocrine resistant and visceral disease: Abemaciclib? • Premenopausal: Ribocilcib? Combine all CDK 4/6 clinical trial data (in 1 st and 2 nd line) and perform a meta-analysis to reveal any potential differences in subgroups

Grazie !

 PALOMA 2 22")
Endocrine sensitive Primary Endocrine resistance (Relapse during or < 12 mo) PALOMA 2 22 77 MONALEESA 2 94. 6 5. 4 MONALEESA 7 7 93 MONARCH 3 100 26

- Slides: 36