The Eye Ocular Pursuit Eye wanna win but

The Eye

Ocular Pursuit “Eye wanna win” but “There is no eye in team”

History • Trauma – Consider unrecognized trauma- awoke with symptoms • • • Pain? Itch? FB sensation? Visual acuity changes, halos Contact lenses- ? Overwear Sick contacts/Viral symptoms Prior surgery or eye disorders Systemic disease


Eye exam (the basics. From a non-ophthalmologist who isn’t particularly good at examining eyes. ) if you can read this last line I’ll eat my shoe right here and now.

Eye exam • • • Visual acuity Visual fields Pupil shape and reactivity Lid closure Foreign bodies Ciliary flare Foggy cornea (edema) Corneal infiltrate Fluorescein- corneal defects, Sidel’s sign Anterior chamber cells Intraocular pressure
 Examine each eye")
Visual Acuity • • Snellen Chart Use corrective lenses (or pinhole) Examine each eye separately If can’t read largest letter, go to finger counting • If can’t count fingers, check motion perception • If no motion perception, go to light perception

Abbreviations which will impress your chart reader • OS – Left eye • OD – Right eye • OU – Both eyes • VA – Visual acuity

Ocular Pursuit Question #2 • What does the latin abbreviation OS stand for?

More Abbreviations • • • L/L/L – Lids, lashes, lacrimal C/S – Conjunctiva and Sclera K – Cornea AC – Anterior Chamber I – Iris L – Lense AV – Anterior Vitreous CF – Count Fingers HM – Hand motion LP – Light perception

Match the nerve with the extraocular muscle! • Extraocular Muscle • Cranial Nerve • • VI Superior Oblique Superior Rectus Lateral Rectus Medial Rectus Inferior rectus Inferior oblique • III • IV

Pupillary Reactions • Patient looks in the distance • Hold light in front of eye #1 for 3 -5 seconds, then swing to the other eye • Should get initial constriction, then dilation

Anterior – posterior • Lids, lashes • Conjunctiva, sclera, cornea • Evert eyelids • Anterior chamber • Retina

Intraocular Pressure Measurement • Tonopen – need to calibrate first • Normal measurements 10 – 21 mm. Hg

Approach to Ophthalmic Emergencies • Diagnostic Category – trauma, vascular, infectious, inflammatory, chemical exposure • Location - extraocular and periorbital, conjunctiva, sclera, cornea, anterior chamber, lens, posterior chamber, retina, vascular • Symptom

Symptom approach • • • 1. Vision loss Painless Painful 2. Eye pain 3. Red eye and discharge 4. Double vision

Painless Vision Loss • • • Retinal Detachment Central Retinal Artery Occlusion Central Retinal Vein Occlusion Vitreous hemorrhage Occipital lobe TIA/CVA Toxins (Methanol)

Central Retinal Artery Occlusion • Anatomy • Internal Carotid Artery – – Ophthalmic Artery » Central Retinal Artery

CRAO

History • Sudden, painless, monocular blindness • Most of the visual field - worse in the central visual field
 • Trauma")
Causes • Emboli – most common • Vasculitidies (temporal arteritis) • Trauma

EMERGENCY!!!

Yes. True. But… • Loss of vision may be irreversible within 90 minutes. Needs emergent ophthalmology referral. • Unfortunately… not much evidence for any therapeutic interventions. Studies tend to be small, not one center, without significant change in long term vision.
 • Hemodilution – bolus 1 -2 liters of normal saline")
Therapies (you can try) • Hemodilution – bolus 1 -2 liters of normal saline • Ocular massage – closed lids – 10 -15 seconds – sudden release of pressure • Rebreathing CO 2 – paper bag strategy • Intra-arterial thrombolysis • Anterior Chamber paracentesis – tetracaine – 30 guage needle – aspirate 0. 1 ml.

Bottom line… • Call the opthalmologist immediately if you suspect this diagnosis. • Post CRAO immediate window – treat like TIA – need to look at risk factors (HTN, dyslipidemia, diabetes, smoking), carotid doppler U/S, look for Atrial fibrillation.

Central Retinal Vein Occlusion • Again, sudden, painless, monocular vision loss • More common than CRAO (CRVO prevalence ~ 1%, compared to ~ 1/10000 for CRAO) • Ischemic and non-ischemic variants

Central Retinal Vein Occlusion

Branch Retinal Vein Occlusion
 be helpful • Aspirin • Intravitreal t-PA")
More treatments that may (or may not) be helpful • Aspirin • Intravitreal t-PA • Surgical options • Treat underlying disease

Which of the following ocular problems is most commonly associated with a patient report of “curtain-like” vision loss? • • A. Vitreous hemorrhage B. Retinal detachment C. Optic neuritis D. Central retinal artery occlusion

Retinal Detachment

Retinal Detachment • Acute or subacute monocular vision loss • Floaters • Peripheral vision loss • Patients might describe “curtain like” visual loss

Retinal Detachment • • • Occurs in 1/300 over the course of a lifetime Risk factors: Age Previous cataract surgery Focal retinal atrophy Myopia Trauma Diabetic retinopathy, Family history of retinal detachment Uveitis Prematurity

If you suspect it… • Immediate ophthalmology consultation • Surgical options • Laser treatment of tears –

Vitreous Hemorrhage • History – painless, monocular vision loss • Patients may describe “haze”, “smoke”, “streaks”

Vitreous Hemorrhage • Causes: • Diabetic retinopathy • Posterior vitreous detachment • Trauma (shaken baby)

Vitreous Hemorrhage • Consult ophthalmology: • Will look for any retinal tears which could be mended • Coag studies • Avoid exertional activities which could increase IOP

Doctor… • My eye hurts! • And I can’t see out of it!

Optic Neuritis

Physical exam • Pain with eye movements • Afferent pupillary defect • May see optic disc swelling on fundoscopy

Optic Neuritis • Inflammatory demyelination of the optic nerve • Most common in 20 -40 year old women • Association with multiple sclerosis

Imaging • MRI: • Optic nerve inflammation • Periventricular white matter lesions somewhat predictive of MS

Treatment • Generally improves spontaneously over days – weeks • ? Steroids – may decrease progression to MS – talk to Neurology

Which of the following is one of the diagnostic criteria for temporal arteritis? • • A. Bounding temporal artery pulse B. Erythrocyte sedimentation rate of > 20 C. New headache D. Age > 70

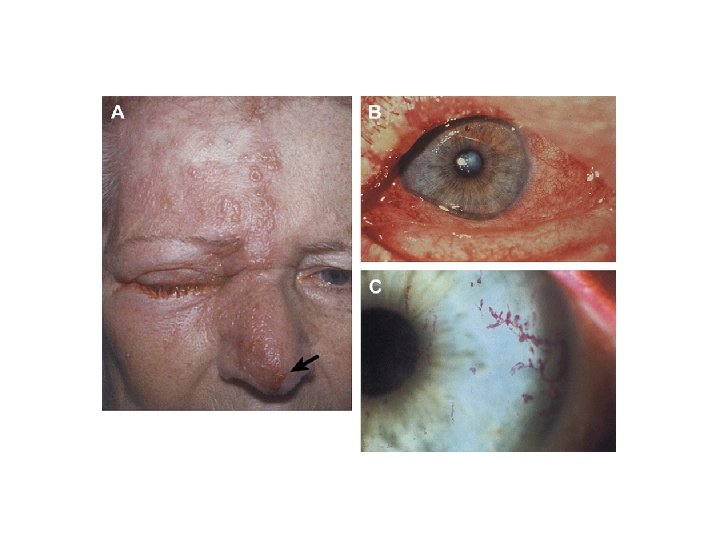
Temporal Arteritis • Medium/large vessel vasculitis • Carotid artery branches • Disease of the elderly

Physical Exam • Palpate – firm, tender temporal artery • Joint pain with movement • Visual acuity

Diagnosis • Age > 50 • New Headache • Abnormalities of the temporal artery (tender, pulseless) • ESR > 50 • Positive biopsy • 3/5 positive findings give sensitivity of 93% and specificity of 91%

Treatment • Consult Ophtho and/or Rheumatology • High dose steroids
 • TIA of the eye •")
Amaurosis Fugax • Transient monocular vision loss (minutes) • TIA of the eye • Neurology consult

Name the phenomenon demonstrated in this picture

Cortical Blindness • Think about it in the patient with vision loss and the absence of eye pathology • Occipital lobe insults, vertebrobasilar infarcts • Usual stroke treatment

Question – name 3 causes of this condition

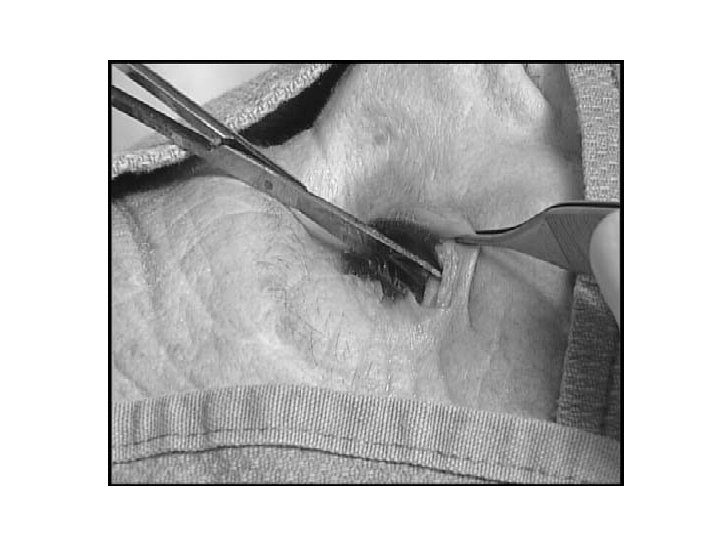
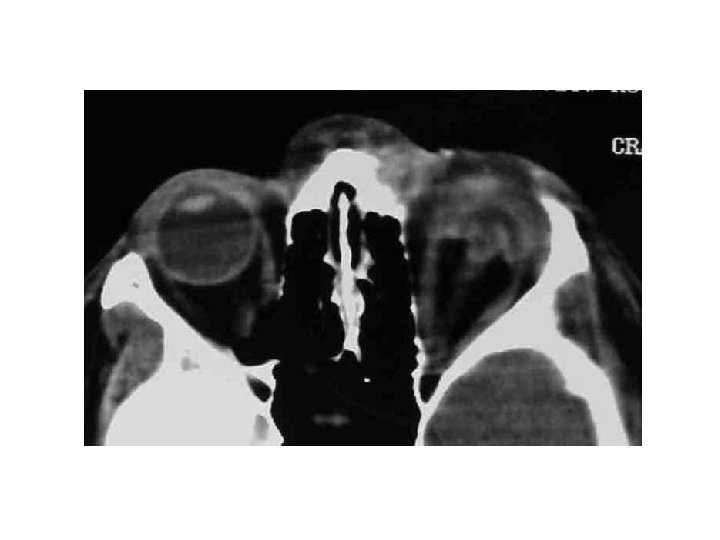
Lateral Canthotomy/Cantholysis • Procedure to decompress a compartment syndrome of the orbit

Retro-orbital hematoma

Primary Indications • Decreased visual acuity • Intraocular pressure > 40 mm. Hg • Proptosis

Contraindication • Globe rupture

The things you’ll need to do your very own lateral canthotomy/cantholysis • • • 1. Lidocaine with epinephrine 2. Syringe with 25 -gauge needle 3. Hemostat or needle driver 4. Iris or suture scissors 5. Forceps

Step 1 • Prep skin • Anaesthetize – lido with epi into lateral canthus


Step 2 • Apply needle driver or hemostat from lateral canthus to bony orbit to devascularize the area for 30 – 90 seconds.


Step 3 • Remove the hemostat and cut the demarcated area 1 – 2 cm laterally


Step 4 • Use the forceps to pull down the lower eyelid until you can see the inferior lateral canthal tendon • Cut through it

Step 5 • Reassess IOP • If still greater than 40 mm. Hg haven’t provided adequate pressure relief: • Expose the superior lateral canthus and cut this too.

Congratulations!
 in the treatment of")
What is the mechanism of action for fomepizole (4 -MP) in the treatment of acute methanol toxicity? • • A. Active diuresis of methanol through the kidney B. Enhanced hepatic conversion of the toxic methanol molecule through CYP 450 3 A C. Competitive elimination with bile D. Competitive inhibition of alcohol dehydrogenase E. Inhibits blood flow through affected organs by the angiotensin pathway

Examination of a ruptured globe with fluorescein may demonstrate displacement of the fluorescein due to aqueous humor flow. This has been named the: • • A. Seidel test. B. Adie’s pupil. C. Gunn’s phenomenon. D. Hoover’s test.

Intraocular pressures associated with acute angle glaucoma tend to be: • • A. > 7 mm. Hg. B. > 14 mm. Hg. C. > 21 mm. Hg. D. > 28 mm. Hg.

Chemical burns to the eye are true ophthalmologic emergencies. Generally speaking, which class of chemicals typically causes more damage? • • A. Acids B. Bases C. No difference D. p. H 7. 4

What is the hallmark finding of vertebrobasilar syndrome? • • • A. Crossed neurologic deficits B. Unsteady gait C. Afferent pupilary defect D. Bitemporal hemianopsia E. “Cherry red” macula

Name that Finding/Disease!

Epidemic keratoconjunctivitis

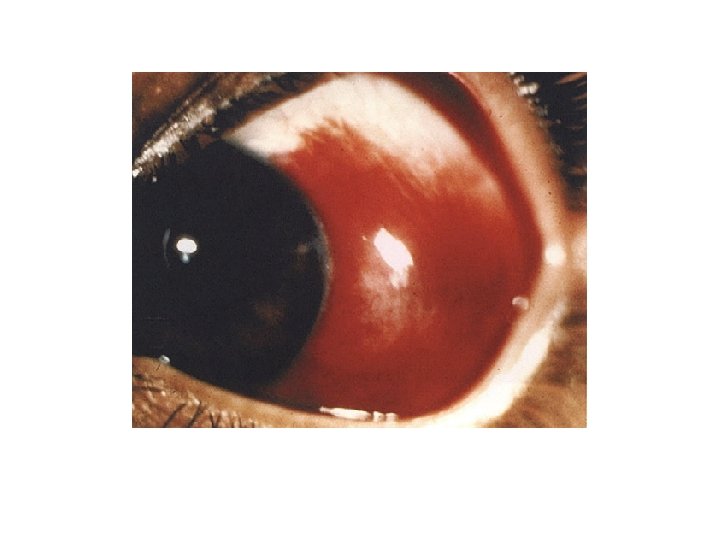
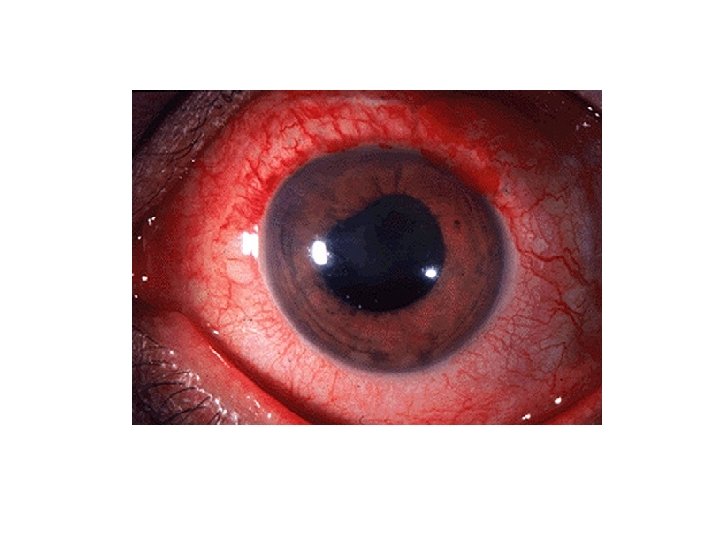
Nodular episcleritis

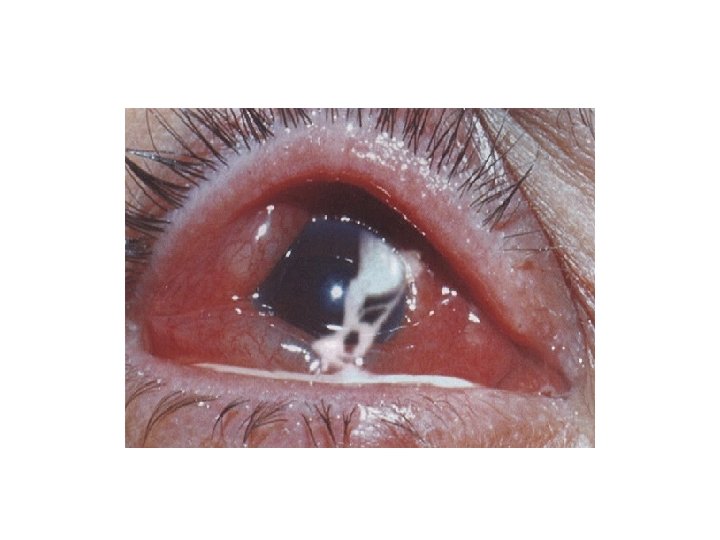
Scleritis

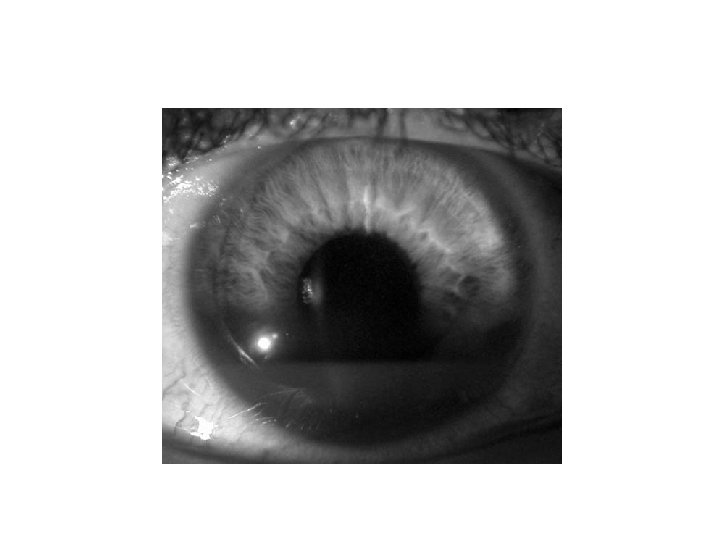
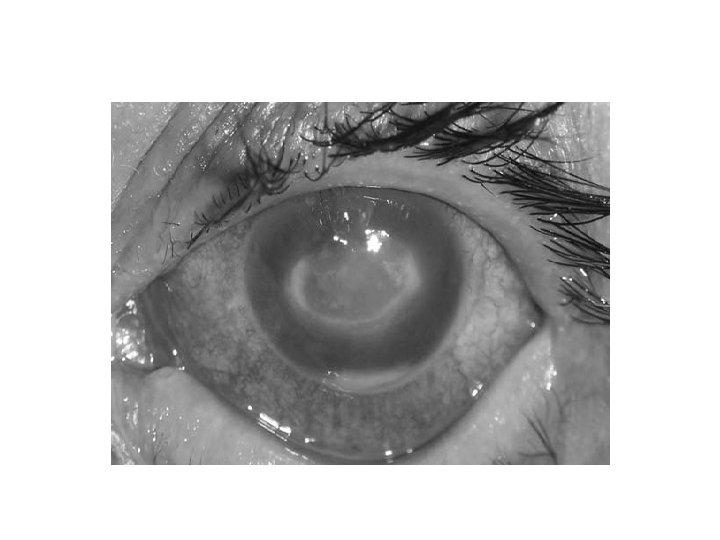
Acute Angle-Closure Glaucoma

Acute angle closure glaucoma • Acute angle closure glaucoma has at least 2 of the following • symptoms: • • ocular pain • • nausea/vomiting • • history of intermittent blurring of vision with halos • And at least 3 of the following signs: • • IOP > 21 mm. Hg • • conjunctival injection • • corneal epithelial edema • • mid-dilated nonreactive pupil • • shallow chamber in the presence of occlusion

References • Basic Ophthalmology – 7 th edition. Cynthia Bradford. American Academy of Opthalmology. • Med Clin N Am 90 (2006) 305– 328 • Emerg Med Clin N Am 26 (2008) 233– 238 • Ophthal Plast Reconstr Surg. 1994 Jun; 10(2): 137 -41. Efficacy of lateral canthotomy and cantholysis in orbital hemorrhage • CJEM 2002; 4(1): 49 -52 • Cochrane Database Syst Rev. 2009 Jan 21; (1): CD 001989. Interventions for acute non-arteritic central retinal artery occlusion. • Emergency Medicine Reports. Volume 29, Number 17. August 4, 2008.
- Slides: 86