The Evolution of the Spinal Needles Joseph Eldor





















")










")























")

")





")



















 (1996")











- Slides: 107
The Evolution of the Spinal Needles Joseph Eldor, MD
An Inguinal Hernia operation in 1382…Without Spinal needles
Valsalva, in 1682, was the first to remark on the CSF when he cut open the spine of a dog and noticed the liquid "which in all its aspects resembles that which is found in the joints".
In 1764, Cotugno described the presence of a collection of water around the brain and inside the spinal column.
In 1825, Magendie was credited with appreciating that this fluid circulated around the brain and the spinal column.
By 1841, Zophar Jayne of Illinois had designed a syringe attached to a small, sharp, hollow beak with an opening on the side near the tip.
Subsequently, in 1853, Daniel Ferguson developed a syringe and hollow platinum trochar with an oblique opening on one side encased in an outer tubing, also with an oblique opening. Ferguson is credited by some as being the first to use a hollow needle with a sharpened extremity, allowing skin penetration and attachment to a syringe.
Alexander Wood of Edinburgh is credited with developing the first hollow hypodermic needle in 1853.
The birthdate of regional anesthesia was September 15, 1884, the date on which Carl Koller , an intern at the Allgemeines Krankenhaus in Vienna, conclusively demonstrated the topical anesthetic properties of cocaine applied to the conjunctiva of the eye.
The first application of the principle of nerve blocking for surgical anesthesia was carried out early in November 1884, when Halsted removed a supraorbital lipoma following cocainization of the supraorbital nerve at the supraorbital notch.
The first spinal anesthetic was administered accidentally by J. Leonard Corning, a Neurologist from New York in 1885.
Corning was experimenting with the action of cocaine on the spinal nerves of a dog when he accidentally breached the dura between two lumbar vertebra, causing paralysis of the hindquarters, and hence inadvertently performed the first spinal anesthesia.
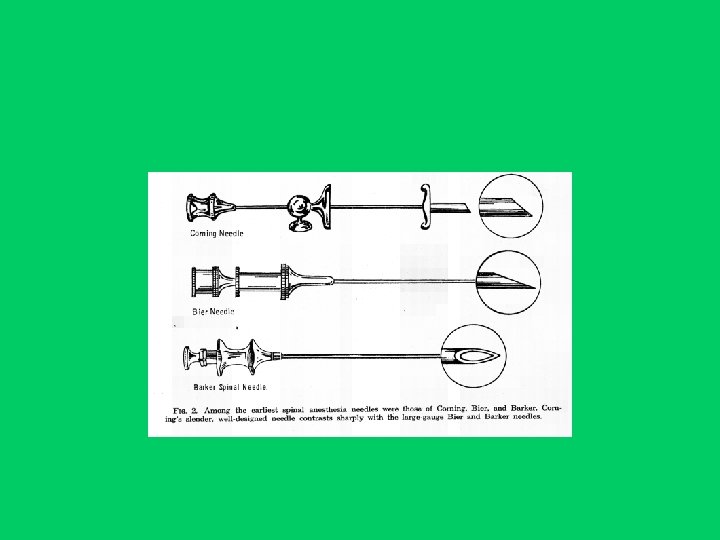
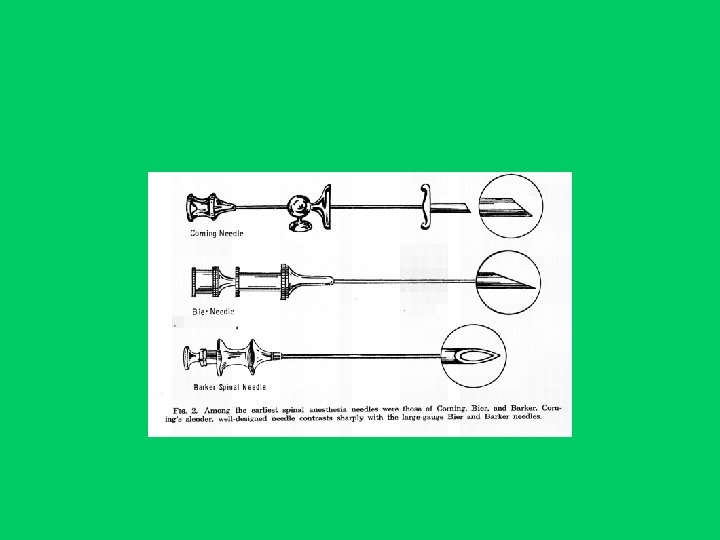
Corning developed his own spinal needle and introducer. The needle was made of gold or platina. The needle tip was based on the hypodermic needle developed by Wood in 1853. It was sharp, with a short cutting bevel.
(Corning Needle (1900
In 1891, Quincke published a paper describing a standardised technique of lumbar puncture for the release of CSF for diseases associated with increased intracranial pressure. He used a needle of which it is difficult to find a description, except that it was a sharp, bevelled, hollow needle.
August Bier, on August 24, 1898, asked his assistant, Dr. Hilderbrandt, "to perform a lumbar puncture on me", 8 days after he first performed it on a 34 -year-old patient for excision of a tuberculous capsule at the ankle joint. Bier wrote that he did not feel any discomfort "except for a quick flash of pain in one leg at the moment that the needle penetrated the meninges". Unfortunately, the experiment was not successful because of an error (the syringe did not fit the needle tightly. . . and consequently some CSF ran out and most of the cocaine was lost). No sensory loss ensued.
Dr. Hilderbrandt immediately offered to submit himself to the experiment, which was successful.
Both of them "went to eat after the experiments were performed on our bodies. We had no physical discomfort, we ate, drank wine, and smoked several cigars". However, next morning, after a one hour morning stroll Bier felt slight headache which increased in intensity during the course of the day. Nine days after the puncture, all the symptoms disappeared. After 3 more days, "I was able to go on a train trip without discomfort and was fit enough to participate in a strenuous 8 day hunting trip in the mountains".
In 1899, Bier published six case reports of surgery to the lower limbs under spinal anesthesia with cocaine. The needle used was described as a Quincke needle.
Bier also designed a larger bore needle that needed no introducer. The Bier spinal needle was 15 G or 17 G, with a long, cutting bevel and a sharp point.
(Bier Needle (1899
Dr. Augustus Karl Gustav Bier (1861 -1949)
Amputation in 1890
Bainbridge described a needle in 1900 that was attached to a metal syringe. It had a small circular hub, a short, sharp cutting bevel and a stylet with a matching bevel.
(Bainbridge Needle (1900
Barker designed in 1907 a needle which had a sharp, medium-length bevel and a stylet with a matching bevel. Barker advised that needles be made of hard nickel.
(Barker Needle (1907
ALL SPINAL NEEDLES ARE NOT CREATED EQUAL…
As early as 1898 Sicard realised that the cause of PDPH (Post Dural Puncture Headache) was the loss of CSF through the dural tears.
In 1914, Ravaut advised the use of finer needles to limit the size of the dural tear.
In 1914, Babcock described a needle that was closer in design to the original Corning needle but with a finer cannula to limit the incidence of PDPH. It had a sharp, medium-length bevel with a matching stylet. It was made of iridised platinum or gold and was 20 G in diameter. Referred to as the Quincke-Babcock needle.
Quincke-Babcock Needle (1914)
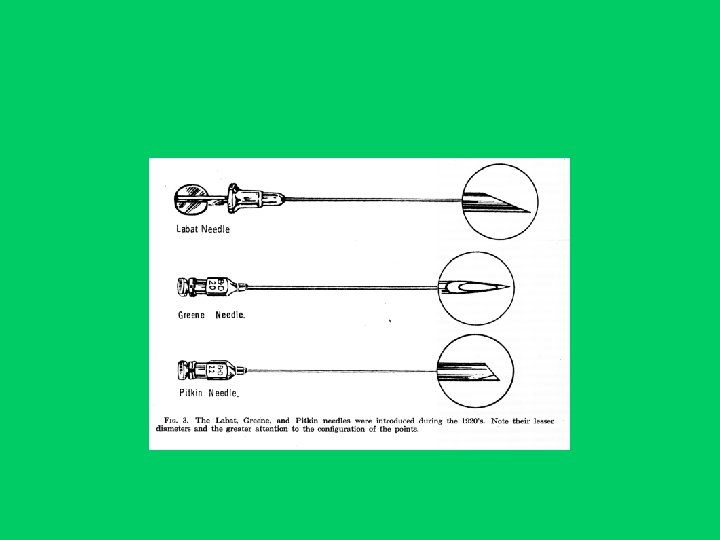
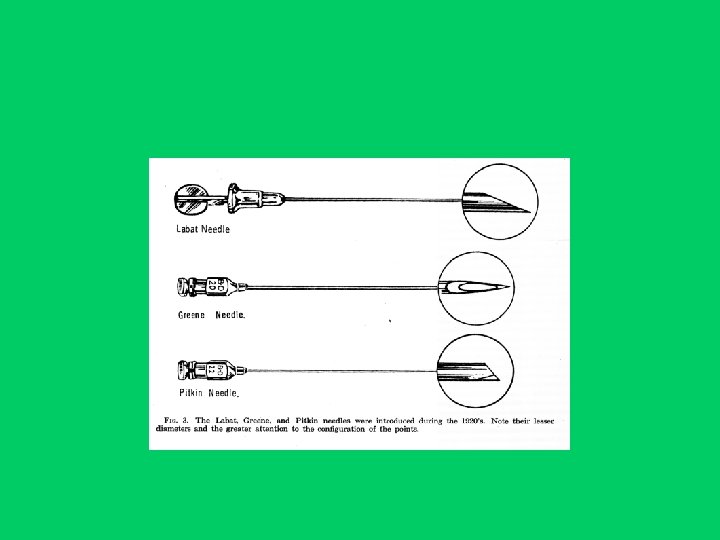
Gaston Labat designed a spinal needle that was made of unbreakable nickel. It was a medium-gauge cannula with a short, sharp bevel and matching stylet, with the tip ground to match the bevel of the cannula.
(Labat Needle (1921
In 1922, Hoyt published his theory that the large bore needles were, because of their rigidity, resulting in large holes in the dura and an increased loss of CSF. He proposed the use of a two-needle technique with a larger bore outer needle being used for penetration of the outer tissues and a finer inner needle for penetration of the dura and arachnoid.
(Hoyt Needle (1922
In the 1920 s, heat-tempered stainless steel was developed in England. Towards the end of World War I, Germany was manufacturing a hard steel alloy that was rustproof, very resistant to breaking and could be worked to a sharp point that was resistant to deformation. The rustproof products became the mainstay of needle production.
The Greene needle was sized between 20 G and 26 G. The point was a rounded, noncutting bevel of medium length with a matching, bevelled, fitted stylet.
There is some disagreement as to the actual date of the introduction of the Greene needle: Herbert Morton Greene presented his work in 1923 and 1926. However, the design should perhaps be attributed to Barnett A Greene who, in 1950, published on the use of a 26 G needle passed through a 21 g introducer.
(Greene Needle (1926 or 1950
George Praha Pitkin devised in 1927 a 20 G or 22 G needle made of relatively flexible rustproof steel with a collar to mark the depth of insertion. The tip of the needle had a short, sharp bevel ground off to a taper of 45º, resulting in a rounded, blunted bevel heel.
(Pitkin Needle (1927
Kirschner, in 1931, described a needle for spinal anesthesia with an opening in the shaft just proximal to the beveled closed end. He claimed that the lateral orifice allowed unilateral, cephalad or caudal anesthesia to be administered.
Rovenstine took up the design idea of the closed-end needle and in 1944 published a paper describing his spinal needle. Rovenstine’s needle was 19 G or 20 G. It had a closed, short-bevelled point with a lateral orifice 2 mm from the distal end of the needle.
(Rovenstine Needle (1944
Haraldson, a Swedish doctor, published a paper in 1951 (several months before Hart and Whitacre) that described a needle with a solid non-cutting tapering point and an orifice on the conical surface 2 mm from the actual tip of the needle. He quoted a PDPH rate of 9% for the noncutting needle (none severe) as opposed to 32% (18% severe) for a cutting needle.
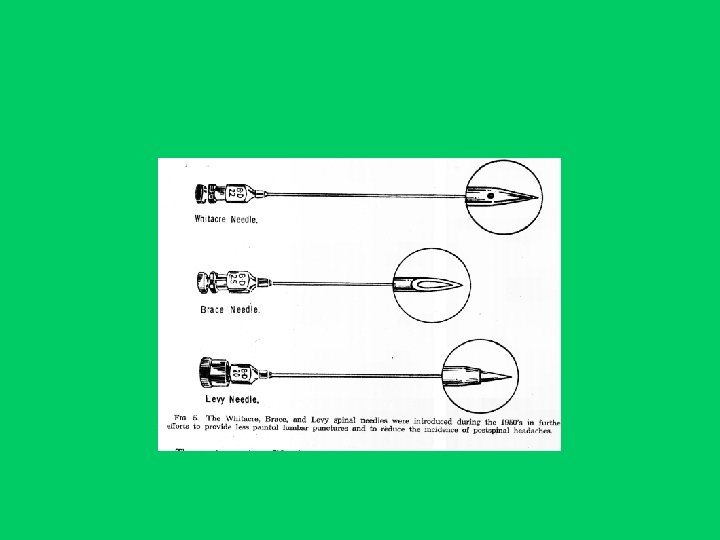
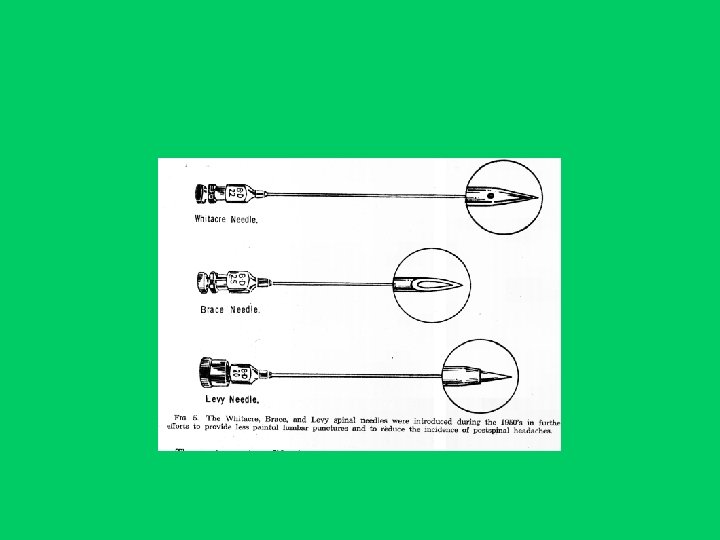
Hart and Whitacre published their paper entitled: “Pencil point needle in prevention of post spinal headache” in October 1951.
(Whitacre Needle (1951
In 1955, Brace produced a needle with a medium length, sharp, cutting bevel.
(Brace Needle (1955
Continuous spinal anesthesia needles
Dean had described a technique of continuous spinal anesthesia in 1907 in which he left the spinal needle in situ during surgery and injected more local anesthetic solution as and when necessary…
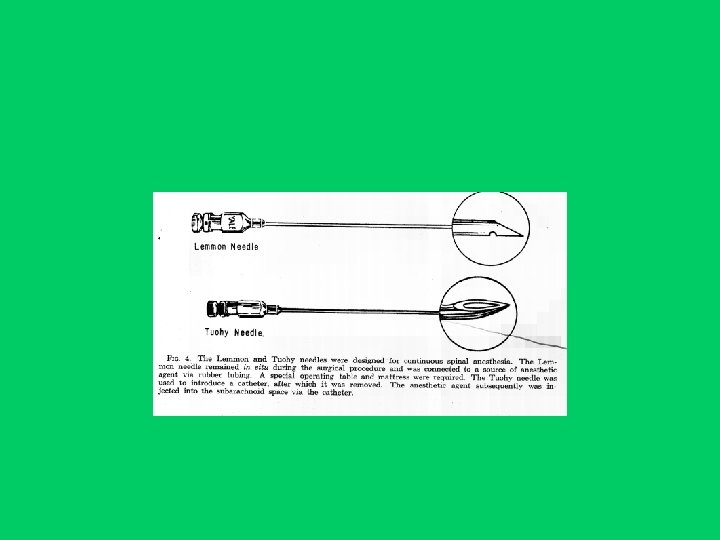
Lemmon published a paper in 1940 describing a 17 G or 18 G nickel/silver alloy malleable needle and introducer with a sharp, medium-length, cutting bevel and a small opening in the long side of the bevel to enable free flow of CSF. The patient lay on a mattress and table that had a hole placed so as to accommodate the protruding needle…
(Lemmon Needle (1940
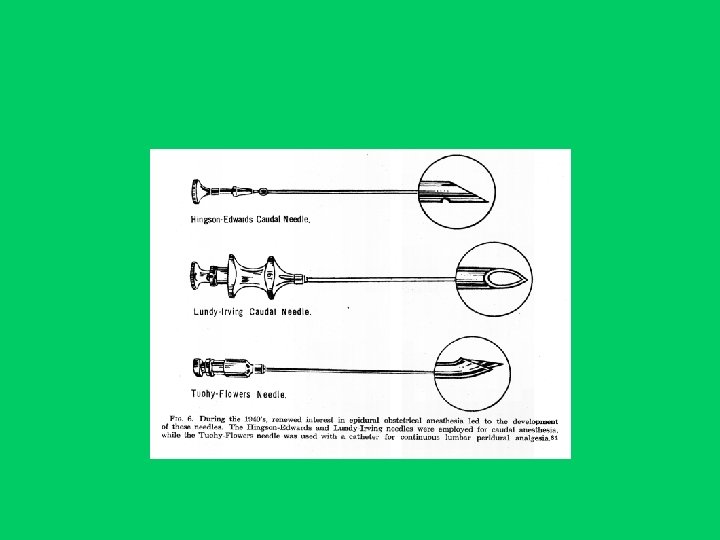
In 1943, Hingson presented his modification of the Lemmon needle.
Hingson-Ferguson Needle (1943)
In 1944, Tuohy used a 15 G directional spinal needle through which he passed a nylon ureteric catheter into the subarachnoid space to allow continuous spinal anesthesia.
Edward Boyce Tuohy (1908 -1959)
(Tuohy Needle (1944
A year later, Tuohy published an article describing an adaptation of his needle to incorporate a “Huber tip”, which allowed directional control of the catheter to point cephalad or caudal as required.
One of the modifications of the Tuohy needle was the Tuohy-Flowers needle, with a shorter and blunter bevel and the stylet protruding beyond the bevel of the needle to ease insertion of the point through tough ligaments.
(Tuohy-Flowers Needle (1956
Another needle for continuous spinal anesthesia was that of Cappe and Deutsch who described in 1953 a malleable cone-tipped spinal needle. It was 20 G in diameter and had a Whitacre tip and an 18 G introducer.
Cappe and Deutsch Needle (1953)
On October 13, 1947, two incidents occurred which resulted in one of the most famous of all medicolegal actions as far as the speciality of anesthesia was concerned. Two patients, Cecil Roe and Albert Woolley who were on the same operative list for relatively minor surgical procedures, developed permanent, painful, spastic paraparesis following spinal anesthesia with hypobaric 1: 1500 cinchocaine (nupercaine; dibucaine) administered by the same anesthetist. Both patients sued the hospital and the anesthetist and the case came to court in October 1953 and lasted 11 days.
This case had a profound effect on the practice of spinal anesthesia, as anesthetists were fearful of producing permanent neurological damage and the technique, in the UK, was probably retarded by 20 -25 years.
However, Noble and Murray in a review published in 1971 of 78, 746 spinal anesthetics in Canada, found no permanent neurological sequelae.
Similarly, Moore and Bridenbaugh in 1968 surveyed 12, 386 and Dripps and Vandam in 1954 - 10, 098 spinal anesthetics, and did not find evidence of permanent neurological deficits.
In an editorial published in 1975 on spinal anesthesia Scott and Thorburn wrote that "it has been virtually ignored in the last 20 years for several reasons, including the introduction of muscle relaxants. Since the Woolley and Roe cases, reported in 1954, in which two patients developed painful and permanent paraplegia following spinal anaesthesia, the use of the technique in the United Kingdom has been confined to a few enthusiasts".
Levy described his stylet-point needle in 1957, 29 years after Sise first described a needle where the stylet formed the tip of the advancing needle. Levy needle was a 20 G needle with a sharp pencil-point tip that included the stylet, and which protruded 2 -3 mm beyond the bevelled end of the cannula, with a smooth junction between the two.
(Levy Needle (1957
Tapered needles were one way of providing needle rigidity while having the finer tip. The cannula was 20 g at the hub, tapering to 24 g at the tip. The tapers available were either a gradual taper or a distal taper.
Gradual Taper Needle
Distal Taper Needle
The 1960 s saw the introduction of disposable spinal needles.
The 1970 s saw an increasing use of epidural anesthesia for surgical procedures.
However, by the late 1980 s, spinal anesthesia was once more becoming a popular technique.
Thirty seven years after Whitacre’s development of the pencil-point needle, Sprotte published in 1987 his paper on a modification of the Whitacre needle.
(Jürgen Sprotte (born: 1945
(Sprotte Needle (1987
A study describing the Atraucan needle was published in 1993. It has a double bevel with the sharp point making an initial incision. The second part of the bevel then dilates this incision rather than cutting a larger hole.
(Atraucan Needle (1993
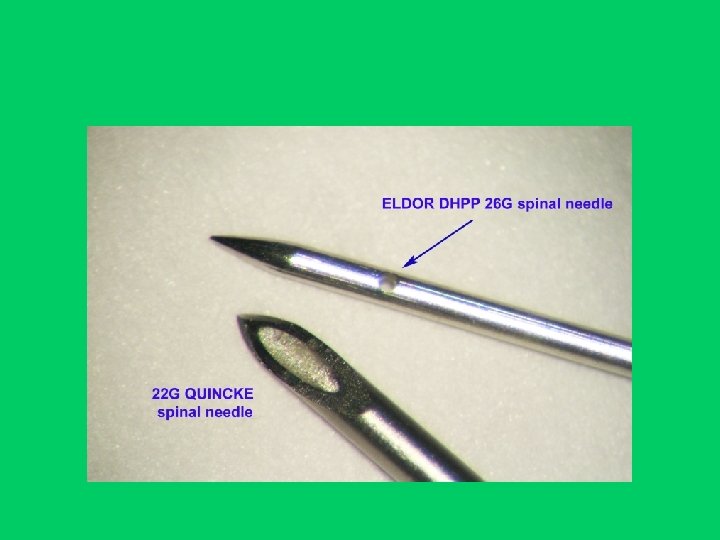
Eldor decribed in 1996 a pencil point tip with two lateral holes opposite each other.
(Eldor Needle (DHPP) (1996
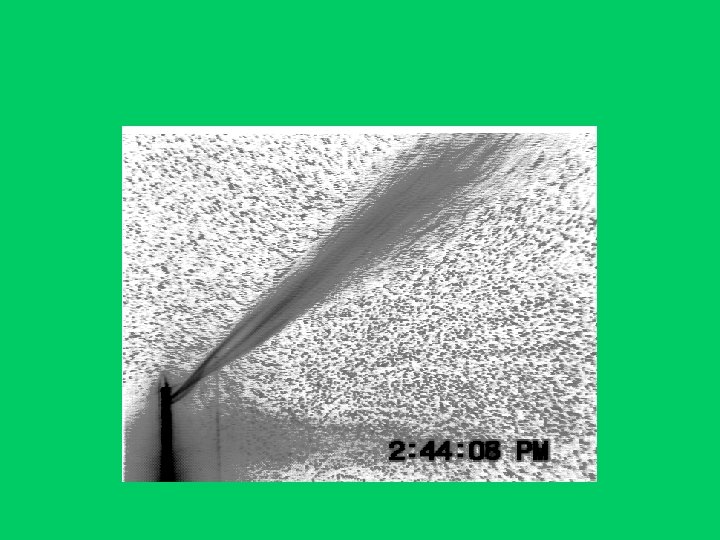
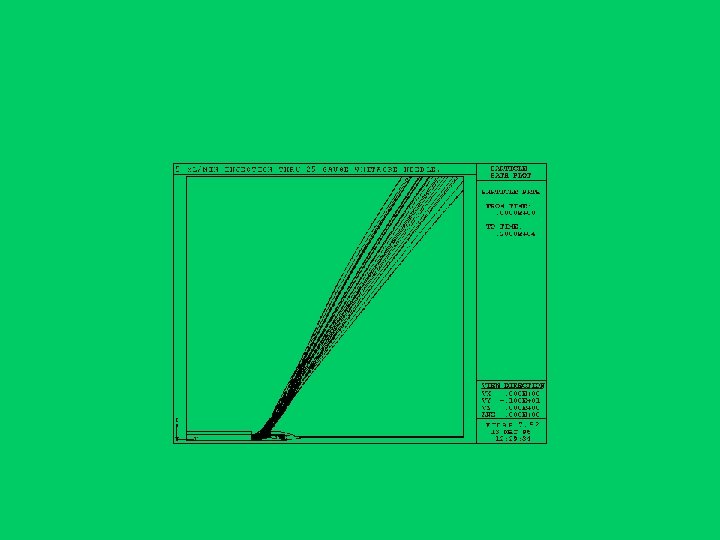
Eldor Needle: Advantages - The area of the two holes is almost the same as of the single hole Sprotte needle`s area, which enables more rapid CSF reflux. - The anesthetic solution injection spreads through both holes. - There is a possible advantage of a more diffuse anesthetic dispersion and less anesthetic solution dosage. - The Eldor spinal needle allows anesthetic solution injection when one of the holes is obstructed by a tissue fragment, through the opposite hole. - It reduces the incidence of the Transient Neurologic Symptoms (TNS).
Eldor needle dispersion
In 2000, an article was published that described a “new design concept” – a modification of a Quincke needle to make a “tip holed spinal needle”. It is marketed as the “Ballpen” without mentioning its true inventor from 1957 – Dr. Levy.
(Ballpen Needle (2000
In a meta-analysis of a total of 29 studies with a 2, 813 patients ALMOST ALL THE CASES OF TNS (TRANSIENT NEUROLOGIC SYMPTOMS) WERE DONE BY THE WHITACRE, SPROTTE, PENCIL POINT, or the SMALL BORE QUINCKE. (Eberhart LH, Morin AM, Kranke P, Geldner G, Wulf H. Transient neurologic symptoms after spinal anesthesia. A quantitative systematic overview (meta-analysis) of randomized controlled studies. Anaesthesist 2002 Jul; 51(7): 539 -46).
Single hole dispersion
“The most likely explanation is maldistribution of the drug in the CSF causing high local concentrations around certain nerve roots. ” (Gisvold SE. Editorial. Acta Anaesthesiol Scand 1999; 43: 369– 370).
A dural hole made by a 22 G spinal needle
A dural hole made by a 28 G Pencil point spinal needle
"Evolution is not a force but a process. Not a cause but a law. " John Morley (1838 -1923)
THANK YOU