THE EFFECTS OF A MODERATEINTENSITY CIRCUITTRAINING EXERCISE PROTOCOL

 is the state of an underactive thyroid and is the")







- Slides: 10
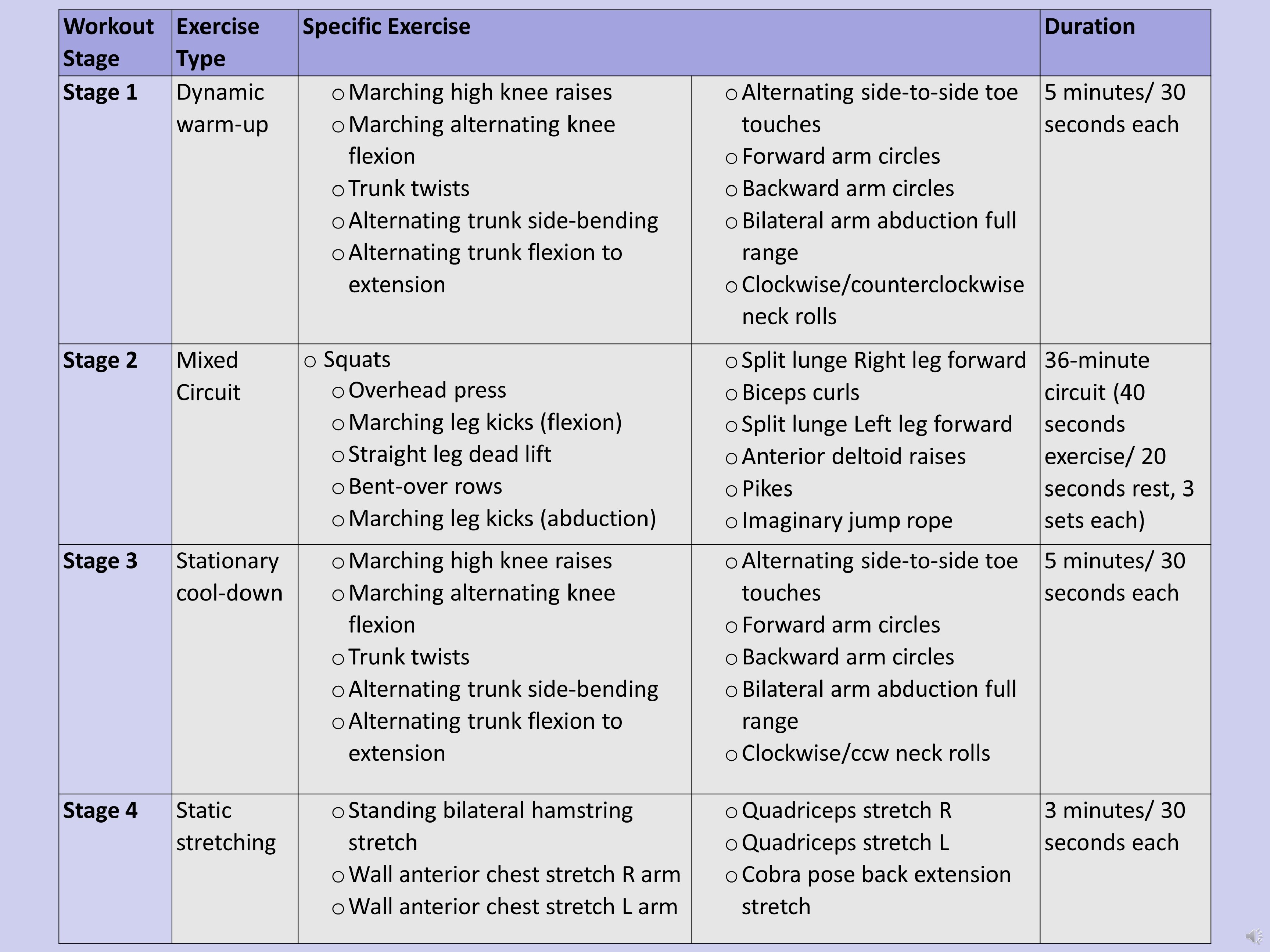
THE EFFECTS OF A MODERATE-INTENSITY CIRCUIT-TRAINING EXERCISE PROTOCOL ON WOMEN WITH HYPOTHYROIDISM: A CASE REPORT Kayla Knight, SPT Dr. Rob Sillevis, PT, DPT, Ph. D, OCS, FAAOMPT, MTC; Dr. Jacqueline van Duijn, PT, DPT, OCS Florida Gulf Coast University, Department of Rehabilitation Sciences, Fort Myers, FL, USA Introduction Clinical Impression Outcomes • Hypothyroidism (HT) is the state of an underactive thyroid and is the second most common type of endocrine disorder predominantly affecting women of reproductive age with a 5 -20 times higher incidence rate than men. 1, 2 • She presented with several symptoms related to hypothyroidism and had poor body composition in the form of obesity and poor cardiovascular health related to her low VO 2 max and hypertension. • Common manifestations of HT are reduced metabolism, weight gain, fatigue, decreased cardiac output, decreased exercise capacity, increased cardiovascular risk (e. g. Hypertension and/or vascular issues). 3, 4 • It was expected that there would be no adverse effects on her HT and hypothesized that the proposed exercise protocol would have a positive effect in improved baseline measurements of health and symptoms, thus supporting the use of therapeutic exercise as a potential method of treatment for HT. • There are currently no validated evidence-based parameters of exercise for the female population with hypothyroidism. 5 Current research of exercise tolerance with HT in general is scarce. • Based on reviewed literature, it appears that circuit training at a moderate intensity, combining strength exercises with aerobics is an appropriate exercise regimen to trial with HT patients. 6, 7 Patient History/Systems Review • The case subject was a 56 -year-old female with a long-time history of health struggles since her initial diagnosis with Hypothyroidism sixteen years ago. • This included thyroid hormonal imbalance, high blood pressure that began seven years ago, and difficulties with increased weight gain/losing weight. • The subject also has experienced other symptoms such as depression, fatigue, dizziness and concentration issues. • Upon baseline testing, it was established that she was in a deconditioned state. Intervention Week 1: Baseline testing Weeks 2 -9: 8 -week exercise intervention moderate-intensity circuit-training • Pre-participation vitals (BP, HR) • Individualized resistance measured at moderate intensity (12 -14 using Borg RPE scale) Week 10: Post Intervention testing • She has been unable to adhere long-term to any regular exercise program • She was on the hormone replacement medication NP Thyroid 120 milligrams at the time of the examination, and consented to participation. Examination • Thyroid Symptom Rating Questionnaire symptoms, waist-tohip ratio, weight, pre/post VO 2 Max using the six-minute walk test (6 MWT), blood pressure (BP), and heart rate (HR) data was collected. (Thy. SRQ)8 Stage 2 Mixed Circuit • The subject completed a 15 -symptom survey using the Hypothyroidism Symptom Rating Questionnaire (Thy-SRQ questionnaire). 8 • The highest scores of symptoms bothersome to the participant on the Thy. SRQ 8 were given to tiredness, weight gain, memory problems, concentration issues, dizziness, and depression. Stage 3 • The subject reported experiencing 9 of the 15 symptoms included in the survey in some capacity. Variable Measurement Weight 211 lbs BMI 32. 2 WHR . 86 BP 1 133/80 mm. Hg HR 1 75 bpm VO 2 Max 9. 6 m. L · kg− 1· min− 1 Stage 4 Stationary cool-down Static stretching • Improved quality of movement • Less soreness • Increase in speed of movement, resistance tolerated, or both Thy. SRQ 8 symptoms such as dizziness, depression, concentration and weight gain were reduced the greatest (3 to 0). Other areas of improvement were regarding fatigue, hair loss, skin problems, hearing, and memory. Variable • BP, HR, Waist-to-Hip Ratio, Weight, 6 MWT, Thy. SRQ 8 Workout Exercise Stage Type Stage 1 Dynamic warm-up Exercise Performance: Specific Exercise o Marching high knee raises o Marching alternating knee flexion o Trunk twists o Alternating trunk side-bending o Alternating trunk flexion to extension o Squats o Overhead press o Marching leg kicks (flexion) o Straight leg dead lift o Bent-over rows o Marching leg kicks (abduction) Completion Measurement Weight Baseline Measurement 211 lbs BMI 32. 2 31 WHR . 86 . 85 BP 133/80 mm. Hg HR 75 bpm 136/84 mm. Hg (10 th Measurement) 75 bpm (10 th Measurement) VO 2 Max 9. 6 m. L · kg− 1· min− 1 13. 3 m. L · kg− 1· min− 1 Duration o Alternating side-to-side toe 5 minutes/ 30 touches seconds each o Forward arm circles o Backward arm circles o Bilateral arm abduction full range o Clockwise/counterclockwise neck rolls o Split lunge Right leg forward o Biceps curls o Split lunge Left leg forward o Anterior deltoid raises o Pikes o Imaginary jump rope 36 -minute circuit (40 seconds exercise/ 20 seconds rest, 3 sets each) o Marching high knee raises o Marching alternating knee flexion o Trunk twists o Alternating trunk side-bending o Alternating trunk flexion to extension o Alternating side-to-side toe 5 minutes/ 30 touches seconds each o Forward arm circles o Backward arm circles o Bilateral arm abduction full range o Clockwise/ccw neck rolls o Standing bilateral hamstring stretch o Wall anterior chest stretch R arm o Wall anterior chest stretch L arm o Quadriceps stretch R o Quadriceps stretch L o Cobra pose back extension stretch 3 minutes/ 30 seconds each References: See Handout with Reference List 206 lbs Clinical Implications • This case describes the successful use of a moderate-intensity combined strength and aerobic circuit training program in one female HT subject. • The program was performed over the course of 10 weeks, resulting in improvements in body composition including reduced waist and hip circumference, weight, BMI, and improved VO 2 Max in our subject. • She also reported improvement in overall well-being and selfperception. • The participant was able to successfully complete the program without compromising the integrity of her thyroid condition, nor did she experience overbearing fatigue, unbearable soreness, new onset of pain or injury, or worsening symptoms. • Although this case report showed a positive effect of the exercise program, no cause and effect can be inferred from a case report. • Additional research will be necessary to further explore the effect of a moderate-intensity circuit training program in subjects with HT.
Introduction • Hypothyroidism (HT) is the state of an underactive thyroid and is the second most common type of endocrine disorder predominantly affecting women of reproductive 1, 2 age with a 5 -20 times higher incidence rate than men. • Common manifestations of HT are reduced metabolism, weight gain, fatigue, decreased cardiac output, decreased exercise capacity, increased cardiovascular risk 3, 4 (e. g. Hypertension and/or vascular issues). • There are currently no validated evidence-based parameters of exercise for the female 5 population with hypothyroidism. Current research of exercise tolerance with HT in general is scarce. • Based on reviewed literature, it appears that circuit training at a moderate intensity, combining strength exercises with aerobics is an appropriate exercise regimen to trial 6, 7 with HT patients.
Patient History/Systems Review • The case subject was a 56 -year-old female with a long-time history of health struggles since her initial diagnosis with Hypothyroidism sixteen years ago. • This included thyroid hormonal imbalance, high blood pressure that began seven years ago, and difficulties with increased weight gain/losing weight. • The subject also has experienced other symptoms such as depression, fatigue, dizziness and concentration issues. • She has been unable to adhere long-term to any regular exercise program • She was on the hormone replacement medication NP Thyroid 120 milligrams at the time of the examination, and consented to participation.
Examination • Thyroid Symptom Rating Questionnaire symptoms, waist-to-hip ratio, weight, pre/post VO 2 Max using the six-minute walk test (6 MWT), blood pressure (BP), and heart rate (HR) data was collected. 8 (Thy. SRQ) • The subject completed a 15 -symptom survey using the Hypothyroidism Symptom Rating 8 Questionnaire (Thy-SRQ questionnaire). • The highest scores of symptoms bothersome to the participant on the were given to tiredness, weight gain, memory problems, concentration issues, dizziness, and depression. 8 Thy. SRQ • The subject reported experiencing 9 of the 15 symptoms included in the survey in some capacity.
Clinical Impression • She presented with several symptoms related to hypothyroidism and had poor body composition in the form of obesity and poor cardiovascular health related to her low VO 2 max and hypertension. • Upon baseline testing, it was established that she was in a deconditioned state. • It was expected that there would be no adverse effects on her HT and hypothesized that the proposed exercise protocol would have a positive effect in improved baseline measurements of health and symptoms, thus supporting the use of therapeutic exercise as a potential method of treatment for HT.
Intervention Week 1: Baseline testing 8 • BP, HR, Waist-to-Hip Ratio, Weight, 6 MWT, Thy. SRQ Weeks 2 -9: 8 -week exercise intervention moderate-intensity circuit-training • Pre-participation vitals (BP, HR) • Individualized resistance measured at moderate intensity (12 -14 using Borg RPE scale) Week 10: Post Intervention testing
Outcomes Exercise Performance: Improved quality of movement Less soreness Increase in speed of movement, resistance tolerated, or both 8 Thy. SRQ symptoms such as dizziness, depression, concentration and weight gain were reduced the greatest (3 to 0). Other areas of improvement were regarding fatigue, hair loss, skin problems, hearing, and memory.
Clinical Implications • This case describes the successful use of a moderate-intensity combined strength and aerobic circuit training program in one female HT subject. • The program was performed over the course of 10 weeks, resulting in improvements in body composition including reduced waist and hip circumference, weight, BMI, and improved VO 2 Max in our subject. • She also reported improvement in overall well-being and self-perception. • The participant was able to successfully complete the program without compromising the integrity of her thyroid condition, nor did she experience overbearing fatigue, unbearable soreness, new onset of pain or injury, or worsening symptoms. • Although this case report showed a positive effect of the exercise program, no cause and effect can be inferred from a case report. • Additional research will be necessary to further explore the effect of a moderateintensity circuit training program in subjects with HT.
References 1. Dunn D, Turner C. Hypothyroidism in women. Nursing for Women’s Health. 2016; 20(1): 93 -98. https: //www. sciencedirect. com/science/article/pii/S 1751485115000045. doi: 10. 1016/j. nwh. 2015. 12. 002. Gietka-Czernel M. The thyroid gland in postmenopausal women: Physiology and diseases. Przeglad menopauzalny = Menopause review. 2017; 16(2): 33 -37. https: //www. ncbi. nlm. nih. gov/pubmed/28721126. doi: 10. 5114/pm. 2017. 68588. 3. Brenta G. Diabetes and thyroid disorders. Diabetes & Vascular Disease. 2010; 10(4): 172 -177. http: //journals. sagepub. com/doi/abs/10. 1177/1474651410371321. doi: 10. 1177/1474651410371321. 4. Surks MI. Clinical manifestations of hypothyroidism. Uptodate. Waltham, MA. Retrieved from http: //www. uptodate. com. 2012. 5. Ahmad J, Tagoe CE. Fibromyalgia and chronic widespread pain in autoimmune thyroid disease. Clin Rheumatol. 2014; 33(7): 885 -891. Accessed Jul 16, 2018. doi: 10. 1007/s 10067 -014 -2490 -9. 6. Goodman C, Helgeson K. Exercise prescription for medical conditions: Handbook for physical therapists. FA Davis; 2010. 7. Pedersen BK, Saltin B. Exercise as medicine–evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. 2015; 25: 1 -72. 8. Mc. Millan C, Bradley C, Razvi S, Weaver J. Evaluation of new measures of the impact of hypothyroidism on quality of life and symptoms: The Thy. DQo. L and Thy. SRQ. Value Health. 2008; 11(2): 285 -294. Accessed Jul 9, 2018. doi: 10. 1111/j. 1524 -4733. 2007. 00232. x.