THE DIRECT OBSERVATION SYSTEM DOS Tina Logan P
 Tina Logan, P. I. E. C. E. S. Manager")
THE DIRECT OBSERVATION SYSTEM (DOS) Tina Logan, P. I. E. C. E. S. Manager Geriatric Services Resource Team Revised November, 2016

WHAT IS THE DIRECT OBSERVATION SYSTEM? An Objective Assessment tool An organized way to map behaviours A document that is used to collect objective, measurable data A way to measure/correlate target and positive behaviours A way to determine the “rhythm of the persons day”
 • We can use the DOS to")
Direct Observation System (D. O. S. ) • We can use the DOS to determine effectiveness of our interventions • We can complete a DOS to determine baseline behaviors • When in doubt start a DOS!

Why is it important for us to track behaviors? ü Collects objective data ü Establishes a pattern that substantiates your shared solution finding ü Helps us find meaning behind behaviors ü Examines the entire person ü May reveal that the target behaviors are not happening with the frequency that is subjectively reported by a care giver

How will this result in improved care for our residents? We can focus on Person Centered Care We can provide this objective data to physicians to enhance their understanding of the residents needs We can help families understand their loved ones daily rhythms and frequency of target behaviors We can potentially determine antecedents (triggers) for behaviour by looking at the DOS and therefore will be able to provide intervention to mitigate the behaviors.

Date: Time 0000 0030 0100 0130 0200 0230 0300 0330 0400 0430 0500 0530 0600 0630 0700
 Client Name: Date: Instructions: Use the corresponding numbers")
D. O. S. (Direct Observation System) Client Name: Date: Instructions: Use the corresponding numbers to record the behaviour in ½ hour intervals. 1. Sleeping in Bed 3. Awake/Calm 5. Verbal Aggression (swearing) 2. Sleeping in Chair 4. Calling Out 6. Physical Aggression (slapping) 7. 8. Date: Jan. 1/16 Jan. 2/16 Jan. 3/16 Jan. 4/16 Jan. 5/16 0000 1 1 3 1 1 0030 1 3 3 3 1 0100 3 4 3 5 Time 3 0130 4 5 5 3 5 6 3 0200 4 5 3 4 5 4 3 0230 3 3 4 0300 3 3 3 0400 3 3 3 4 0430 3 3 3 0500 3 3 5 0530 3 4 3 3 3 0600 4 5 5 5 3 0630 3 5 5 0700 3 3 3 5 5 0730 1 3 3 5 3 0800 1 1 3 4 3 0830 3 1 3 3 3 0900 3 1 3 0930 3 3 3 1000 3 3 1 3 3 4 3 5 3 1030 4 5 3 1 5 1 1100 5 3 3 5 5 1 1130 3 3 1 1200 3 4 3 3 3 1230 3 4 3 3 3 1300 3 3 3 4 3 1330 3 3 3 4 4 1400 3 3 4 1430 3 3 3 1500 3 3 4 3 3 1530 3 3 4 3 3 1600 3 3 3 1 1 1630 4 1 3 1 1 1700 4 1 1 1730 1 4 1 3 1 1800 1 4 3 3 3 1830 1 1 3 3 3 1900 1 1 3 1 1 1930 1 1 1 2000 1 3 1 1 1 2030 1 3 3 2100 4 1 3 2130 1 1 4 1 3 2200 1 3 3 1 4 2230 1 1 1 3 1 2300 3 1 1 3 3 2330 3 1 1 2400 1 1 3 1 1


The DOS replaces opinion with measurable data by establishing the: • • Occurrence of a distinct behavioral expression Frequency with which target behaviors occur Duration the target behavior is displayed Frequency with which the target behaviors of the greatest risk are displayed in comparison with those behaviors that are considered positive (ex. Awake/calm).

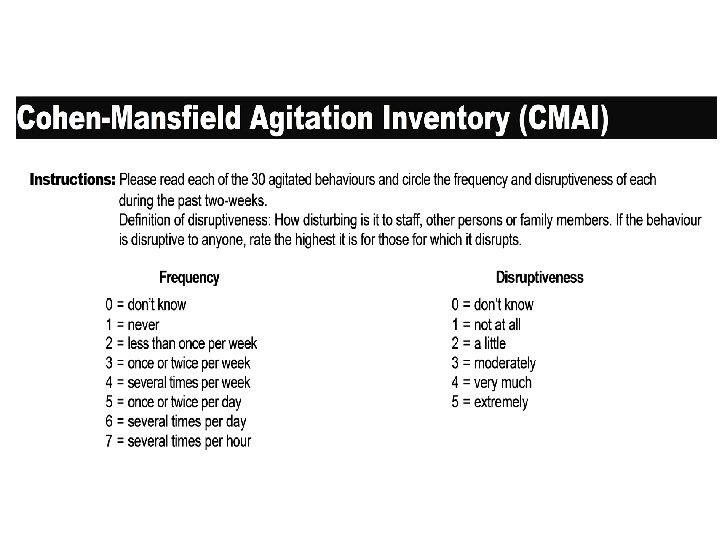
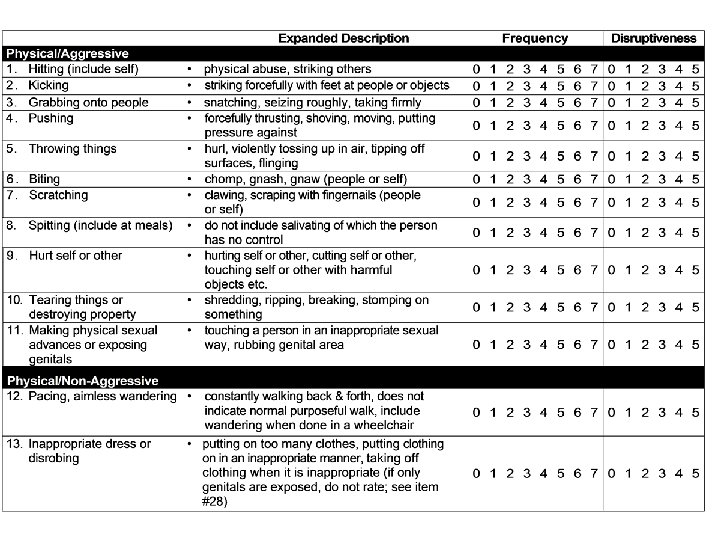
Determining target behaviours of the greatest risk! Discuss as a team the behaviours of concern Use the Cohen Mansfield Agitation Inventory over a 24 hour period. (day shift, evening shift, night shift) to determine which behaviors are the most frequent and disruptive Use specific behavior expressions Avoid “verbal aggression” instead use; ex. “swearing” Avoid “physical aggression” instead use; ex. “slapping”
 The D. O. S. is a caregivers’")
Direct Observation System (D. O. S. ) The D. O. S. is a caregivers’ descriptive worksheet! It has a behavioural key that describes up to eight (8) behaviours, though its important to note that it is recommended to choose only 3 frequent/disruptive behaviours: these target behaviours can be well-defined and written on the form to capture the unique characteristics of the person’s profile Designed so that the lower the number assigned to the behaviour, the lower the associated risk

The higher the number, the higher the associated risk with that behaviour It is very important to include positive behaviour ex. “awake/calm”. Remember to consider behaviors that are causing the most distress to the resident.

Using the DOS Some important tips to using the DOS effectively: 1. Have the entire team participate 2. Track only 1 -3 behaviors (highest risk) 3. Describe the behaviors in detail so everyone knows what they are looking for 4. Highlight the behaviors to more easily see “trends” 5. As a team, analyze the trends – look for rationale and intervention opportunities

When Do You Use D. O. S. ? • Whenever there is a change or concern in the person’s typical behavioral profile • When you are changing, discontinuing or initiating medication or a treatment plan • Whenever the team needs an outcome measure to determine if target behavior has changed in frequency and duration
 Instructions: Decide on target behaviours and when")
Direct Observation System (D. O. S. ) Instructions: Decide on target behaviours and when the D. O. S. will be started and completed. Enter behaviours to be tracked at top of D. O. S. form. Do not add behaviours once you have started the D. O. S Select the corresponding number from the behavioural key that best describes the behaviour being observed and enter it every 30 minutes under the appropriate date Record the behaviour in 30 minute intervals for approximately 3 days (72 hours)

Colour/Number Code for Interpreting the DOS Code Colour Target Behaviours 1 -2 Blue Sleeping in bed or chair 3 Green Awake/Calm 4 Pink Verbal Disruptions 5 Yellow Restless/Pacing 6 Orange Exit Seeking 7 Purple Verbal Aggression 8 Red Physical Aggression NOTE: For Verbal Disruptions and Verbal and Physical Aggression - please use specific behaviours derived from the CMAI to describe these behaviours in more detail when setting up the DOS.

Completing the D. O. S. At the end of the observation period, colour code the graph. using a different colour for each number. (use the colour key from previous slide) Calculate the number of hours spent in sleep, calmness, restlessness, verbal responsiveness/agitation and physical responsiveness Summarize the results and document

Direct Observation System How do we interpret the results? Discuss together as a team Look for patterns that may occur at certain times of the day or are associated with certain routines and discuss strategies to remove those triggers Implement strategies for at least oneweek. Re-administer the D. O. S. to see if target behaviours have been impacted.

DOS Case Study Mrs. J. is an 89 year old lady who moved into a long term care facility six months ago. In the past month, staff has noticed that she is calling out more frequently and becoming verbally aggressive and swearing when staff do not respond to her immediately. She has many vague complaints and had difficulty communicating her needs. She is not oriented to surrounding or staff; significant Short term and long term memory loss. She needs assistant with her ADL’s including dressing, bathing and personal care. She is incontinent of urine and occasionally of bowels. She relies on a wheelchair for mobility and can self-propel at times. Her diagnoses include cerebral vascular accident, diabetes, sleep apnea but refuses treatment, significant osteoarthritis (receives acetaminophen PRN). She can be aggressive with care at times and be explosive and irritable and verbally insult staff. She is very impulsive!! She often wants to be the first resident in the dining room, first to get her meal, and first out and becomes very angry when asked to wait or reminded that she could not always be first and why.

Date: Jan. 1/11 Jan. 2/11 Jan. 3/11 Jan. 4/11 Jan. 5/11 0000 1 4 1 3 1 0030 1 4 3 3 3 0100 1 1 3 3 3 0130 1 1 3 1 1 0200 1 1 1 0230 1 3 1 1 1 0300 1 3 3 0330 4 1 3 0400 1 1 4 1 3 0430 1 3 3 1 4 0500 1 1 1 3 1 0530 3 1 1 3 3 0600 3 1 1 0630 1 1 3 1 1 0700 1 1 3 1 1 0730 1 3 3 3 1 0800 3 4 3 5 Time 3 0830 4 5 5 3 5 6 3 0900 4 5 3 4 5 4 3 0930 3 3 4 1000 3 3 3 1030 3 3 3 4 1100 3 3 3 1130 3 3 5 1200 3 4 3 3 3 1230 4 5 5 5 3 1300 3 5 5 1330 3 3 3 5 5 1400 1 3 3 5 3 1430 1 1 3 4 3 1500 3 1 3 3 3 1530 3 1 3 1600 3 3 3 1630 3 3 1 3 3 4 3 5 3 1700 4 5 3 1 5 1 1730 5 3 3 5 5 1 1800 3 3 1 1830 3 4 3 3 3 1900 3 4 3 3 3 1930 3 3 3 4 3 2000 3 3 3 4 4 2030 3 3 4 2100 3 3 3 2130 3 3 4 3 3 2200 3 3 4 3 3 2230 3 3 3 1 1 2300 4 1 3 1 1 2330 4 1 1

DOS Case Study When you look at the completed DOS what stands out for you? Huddle/Discussion
- Slides: 23