The Digestive System The main objectives of this

The Digestive System

The main objectives of this lecture was : 1. The student most know the most common GIT disorder in children, GERD. 2. To know the mechanism of GERD, the common manifestations among children and method of diagnosis. 3. How mange this common disorder and its complications. 4. to know what is achalasia, how differentiate it from other causes of dysphagia in children.
 Gastroesophageal reflux (GER) : retrograde movement of gastric")
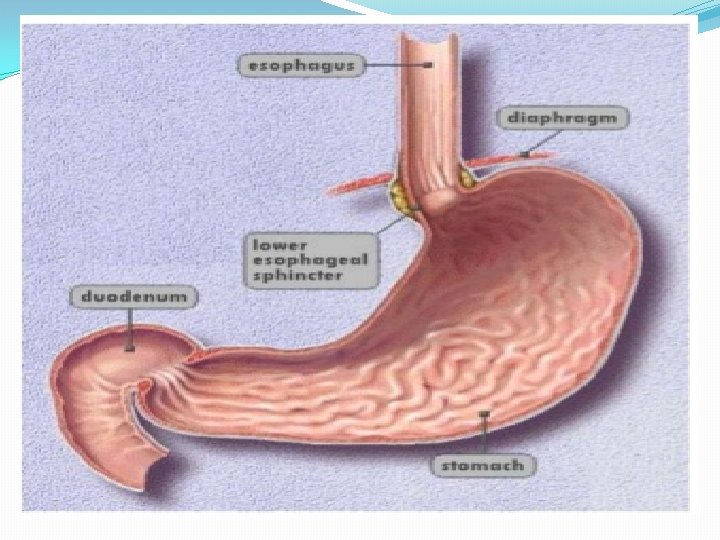
The Esophagus Gastroesophageal Reflux Disease (GERD) Gastroesophageal reflux (GER) : retrograde movement of gastric contents across the lower esophageal sphincter (LES) into the esophagus.
, but when the episodes of reflux")
It is occasionally physiologic (regurgitation of normal infants), but when the episodes of reflux are more frequent or persistent, and thus produce esophagitis or esophageal symptoms, or in those who have respiratory sequelae, the reflux becomes pathologic (GERD).
 *the crura of the diaphragm *gastroesophageal junction")
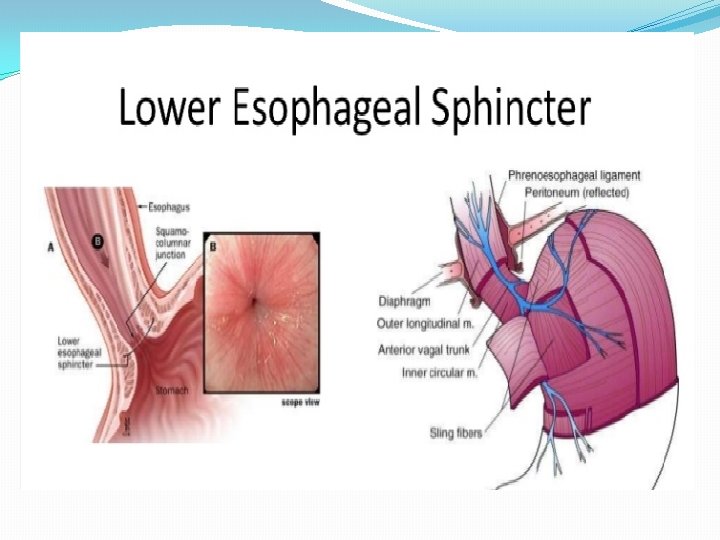
Pathophysiology Antireflux barrier: *lower esophageal sphincter (LES) *the crura of the diaphragm *gastroesophageal junction anatomy

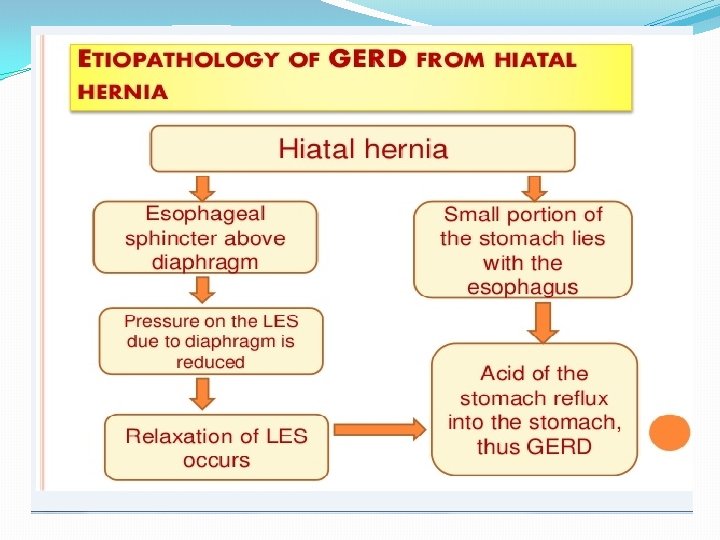
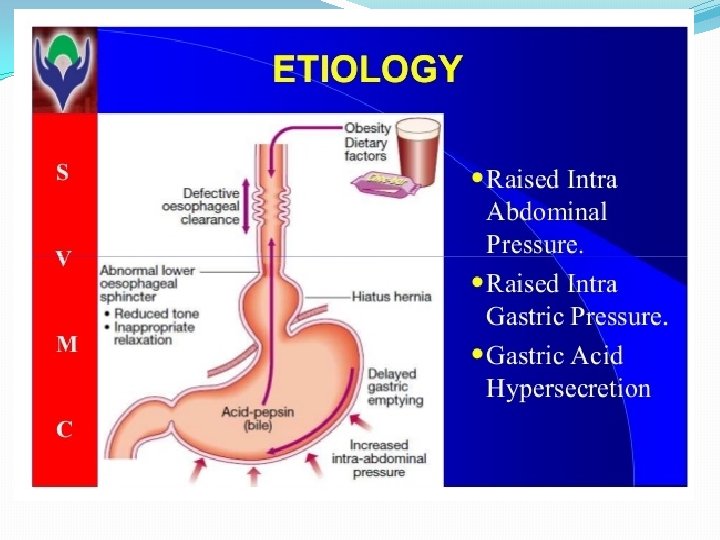
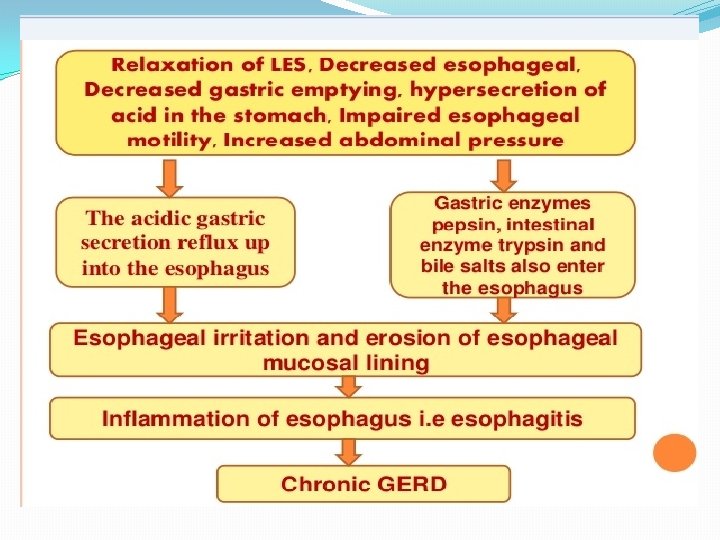
The mechanisms involved in the pathogenesis of GERD are multiple and include: 1. impaired LES resting tone 2. increased number of transient LES relaxations (TLESR) 3. Gastric distention (delayed gastric emptying, large fatty meals) can significantly increase the rate of transient LES relaxations) 4. hiatal hernia (promoting lower oesophageal sphincter dysfunction)

5. Impaired oesophageal acid clearance (this process involves peristalsis as well as the swallowing of salivary bicarbonate) lead to prolonged acid exposure of the mucosa. 6. increase intra-abdominal pressure (straining, obesity, coughing, wheezing).

Epidemiology : Infant reflux becomes symptomatic during the first few months of life, peaking at about 4 mo and resolving in most by 12 mo and nearly all by 24 mo. A genetic predisposition as an autosomal dominant form is located on chromosome 13 q 14 and chromosome 9.
 *signs of esophagitis (irritability, arching,")
Clinical Manifestations �Infantile reflux manifests with: *regurgitation (especially postprandially) *signs of esophagitis (irritability, arching, choking, feeding aversion) and, rarely, as hematemesis, anemia) *failure to thrive These symptoms resolve spontaneously in the majority by 12 to 24 mo.

In older children: *regurgitation during the preschool years. *abdominal and chest pain during later childhood and adolescence *Occasional children present with neck contortions (arching, turning of head) designated Sandifer syndrome. The respiratory (extraesophageal) presentations are also age dependent: In infants :

obstructive apnea or as stridor or lower airway disease. Otitis media, sinusitis, lymphoid hyperplasia, hoarseness, vocal cord nodules, and laryngeal edema. In older children are more frequently related to asthma , laryngitis or sinusitis.

Diagnosis 1. Thorough history and physical examination: GERD should differentiated from other causes of chronic vomiting like milk and other food allergies, pyloric stenosis, intestinal obstruction, inborn errors of metabolism, hydronephrosis, and increased intracranial pressure.
 radiographic study of the esophagus and upper gastrointestinal tract is performed")
2. Contrast (barium) radiographic study of the esophagus and upper gastrointestinal tract is performed in children with vomiting and dysphagia to evaluate for achalasia, esophageal strictures and stenosis, hiatal hernia, and gastric outlet obstruction. 3. esophageal p. H monitoring of the distal esophagus.

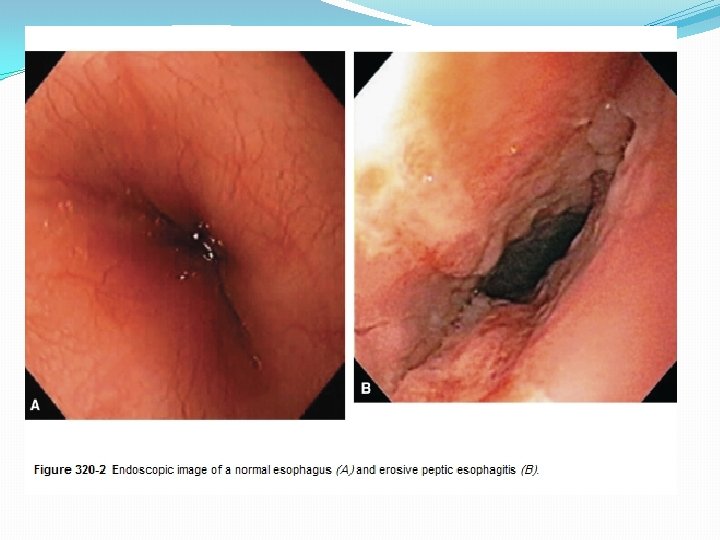
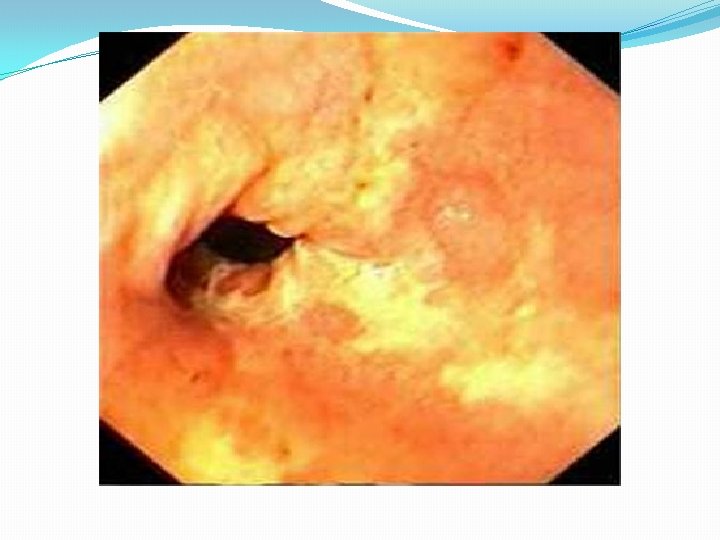
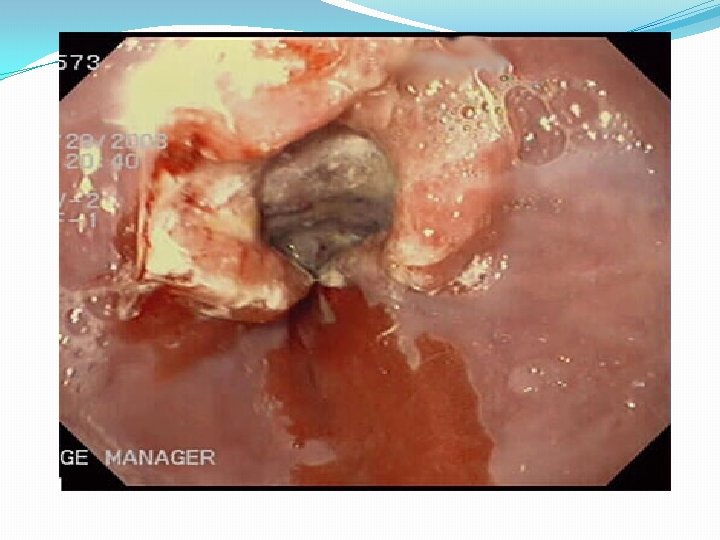
4. Endoscopy : allows diagnosis of erosive esophagitis and complications such as strictures or Barrett esophagus; biopsies can be taken. 5. Laryngotracheobronchoscopy : posterior laryngeal inflammation and vocal cord nodules. 6. Empirical antireflux therapy

Management 1. Conservative therapy and lifestyle modification * Dietary measures for infants include: Normalization of feeding techniques, volumes, and frequency if abnormal. Thickening of formula with a tablespoon of rice cereal per ounce of formula greater caloric density (30 kcal/oz), and reduced crying time.
 and beverages (juices, carbonated")
In older children : avoid acidic foods (tomatoes, chocolate, mint) and beverages (juices, carbonated and caffeinated drinks), weight reduction for obese patients. *Positioning measures: During awake periods when the infant is observed, prone position and upright carried position. For older children: left side position and head elevation during sleep.

2. Pharmacotherapy * Antacids: They provide rapid but transient relief of symptoms by acid neutralization. * Histamine-2 receptor antagonists (H 2 RAs; cimetidine, famotidine, and ranitidine) are antisecretory agents that act by selective inhibition of histamine receptors on gastric parietal cells. There is a benefit of H 2 RAs in treatment of mild-to-moderate reflux esophagitis.
 provide the most potent antireflux effect")
*Proton pump inhibitors (PPIs; omeprazole, lansoprazole, pantoprazole, ) provide the most potent antireflux effect by blocking the hydrogen-potassium ATPase channels of the final common pathway in gastric acid secretion. Also benefit in the treatment of severe and erosive esophagitis. Doses of omeprazole for children (0. 7– 3. 3 mg/kg/day).
 , these increase LES pressure;")
* Prokinetic agents: metoclopramide, and erythromycin (motilin receptor agonist) , these increase LES pressure; some improve gastric emptying or esophageal clearance. 3. Surgery( fundoplication): for intractable GERD in children, particularly those with refractory esophagitis or strictures and those at risk for significant morbidity from chronic pulmonary disease.

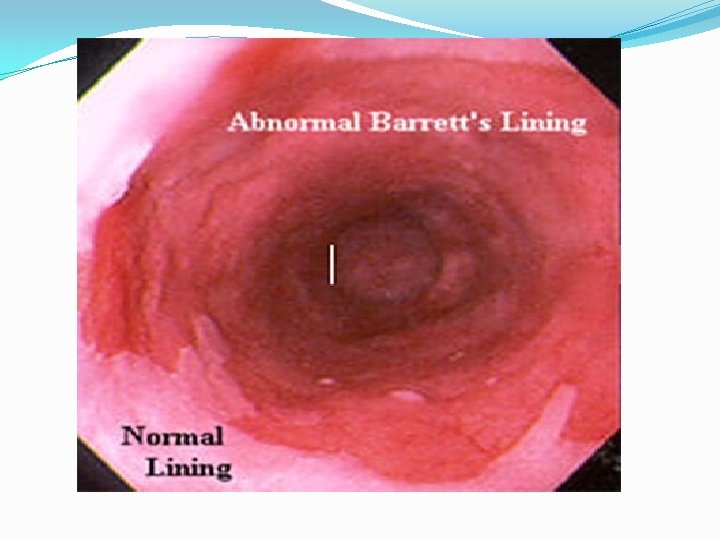
Complications of GERD 1. Esophageal *Esophagitis and Stricture. * Barrett Esophagus *Adenocarcinoma 2. Nutritional: failure to thrive because of caloric deficits.

 Presentations: Apnea, stridor, reflux laryngitis, hoarseness, chronic cough, pharyngitis, sinusitis,")
3. Extraesophageal: Respiratory ("Atypical") Presentations: Apnea, stridor, reflux laryngitis, hoarseness, chronic cough, pharyngitis, sinusitis, otitis media. Asthma may co-occur with GERD in about 50% of asthmatic children. 4. Dental erosions.

Achalasia is a primary esophageal motor disorder of unknown etiology characterized by loss of LES relaxation and loss of esophageal peristalsis, both contributing to a functional obstruction of the distal esophagus. Degenerative, autoimmune, and infectious factors are possible causes. Rarely , it is familial.

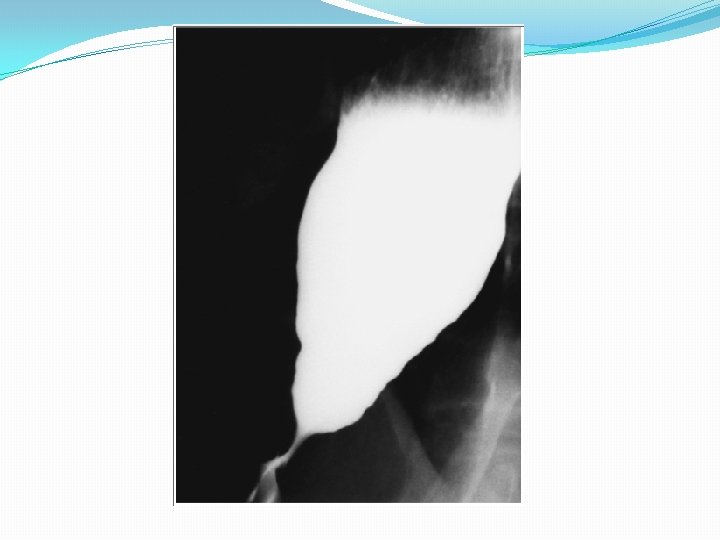
Clinical presentations dysphagia for solids and liquids and may be accompanied by undernutrition or respiratory symptoms. The mean age in children is 8. 8 yr Diagnosis 1. Chest radiograph shows an air-fluid level in a dilated esophagus. 2. Barium fluoroscopy reveals a smooth tapering of the lower esophagus leading to the closed LES, resembling a “bird's beak”.

3. Manometry confirms the diagnosis and reveals incomplete relaxation of a high-pressure LES during swallowing. Treatment *pneumatic dilatation *surgical myotomy. *Endoscopic injection of the LES with botulinum toxin that inhibiting the release of acetylcholine from nerve terminals.

Thank you
- Slides: 36