The diabetic patient with kidney disease and neuropathic

The diabetic patient with kidney disease and neuropathic pain Dr Lisa Chin-Harty MBBS, DM(Internal Medicine) Department of Medicine, UWI

A Patient We All See • 70 year old male with a 20 year h/o poorly controlled type 2 DM and HTN, dyslipidemia • 5 years ago diagnosed with nephropathy after urine screening positive for protein, last e. GFR 60 ml/min/1. 73 m 2 • Proliferative retinopathy sp laser photocoagulation 2 years ago • Developed an ulcer to right foot 1 year ago- has had recurrent debridements • Meds: Metformin 1 gm bid, 70/30 insulin 10 units sc bid, Lisinopril 40 mg od, carvedilol 3. 125 mg bid, ASA 81 mg od, Lasix 40 mg od • Main complaint at every clinic visit is numbness and tingling to both legs with occasional shooting pains.

Epidemiology Diabetic Neuropathy is the most common complication of diabetes In the USA: Diabetic Neuropathy is the • 1. primary cause of diabetic foot problems and ulcerations • 2. leading cause of diabetes-related hospital admissions • 3. Leading cause of non-traumatic amputations. 3

AMPUTATIONS About Foot Ulcers • One in ten result in the amputation of a foot or a leg Leg amputations in people with diabetes is 15 times higher when compared with persons without diabetes

AMPUTATIONS: Mortality in persons with amputations from Diabetes contd • 70 per cent of people die within five years of having an amputation • Amputations are more prevalent in patients with ESRD • Diabetic patients with stage 4 -5 CKD have a 10 times greater risk of amputation vs the diabetic population

Prevalence • 50% of people with diabetes have Diabetic Neuropathy • Prevalence varies from 10% to 90% • Neuropathic pain is present in as much as 50% of all dialysis patients • The progression of diabetes to advanced stages of CKD is associated with progression of other micro and macrovascular complications Innis J. Pain assessment and management for a dialysis patient with diabetic peripheral neuropathy. CANNT J. Apr-Jun; 2006 16(2): 12– 17. 20– 16. quiz 18 -19, 27 -18. [Pub. Med: 16875290] 6

Prevalence of Diabetic Neuropathy in Jamaica • In persons with Newly Diagnosed DM • 31. 1% W I Med J 1998: 47; Suppl 2 : 53

BARBADOS’ 1 -YEAR INCIDENCE OF LOWER EXTREMITY AMPUTATION Non-diabetic population • 173 per 1, 000 population Population with diabetes • 936 per 1, 000 In Madrid, Spain, the incidence is 2. 8 per 1000, 000 per year Hennis et al. Diabetes Care , 27 (11) pp. 2636 -2641. Global Lower Extremity Amputation Study Group. Abstract Br J Surg. 2000 Mar; 87(3): 328 -37.

DCCT: Relative Risk of Developing Chronic Complications of Diabetes in Relation to Hb. A 1 c (%) Adapted by Skyler J, Endocr & Metab. N. Amer, 1996: 250

l Correlation between a 1% reduction in A 1 C and decreased of complication 14% 21% 43% 37% Cardiovascular complication Amputations or death Microvascular from peripheral complications vascular disease (P<0. 0001) Diabetes-related death Myocardial infarction All-cause mortality (P<0. 0001) Stratton 2000: IM, Adler AI, Neil HAW, et al. BMJ. 2000: 321: 405 -412 10 14%

11

DM and Neurotoxicity

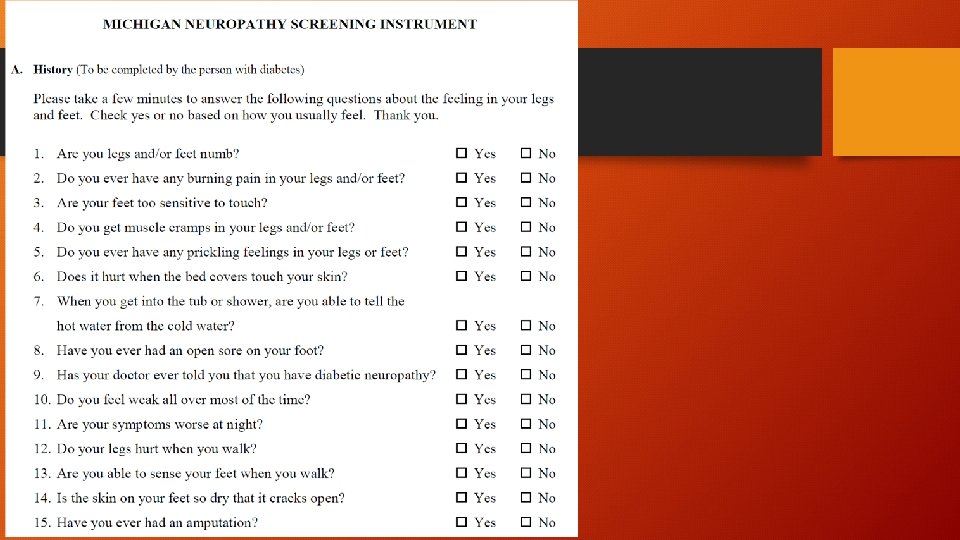
Clinical Features 50 % asymptomatic 4 th November, 2009

Common Descriptions of Neuropathic Pain • • • Numbness Tingling Burning Paraesthesia Paroxysmal Lancinating Electrical-like Raw skin Shooting Deep, dull, bonelike ache 4 th November, 2009 Tanenberg, ADA 2005

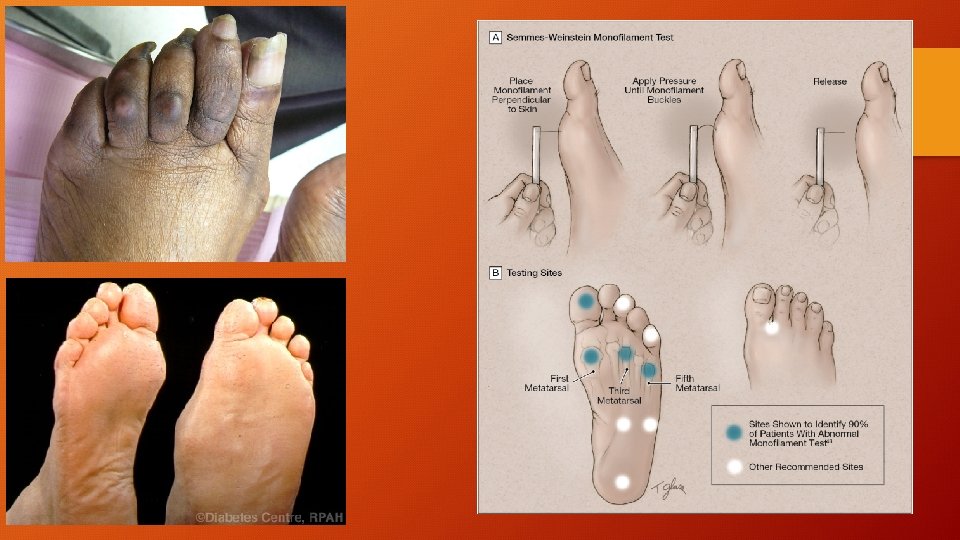
Signs of peripheral diabetic neuropathy • • Bilateral Symmetric https: //youtu. be/mj. ARqy 9_i. Do? t=63 Dulled perception to 1. Vibration 2. pain 3. temperature Especially in the lower extremities

Signs of peripheral diabetic neuropathy contd • • • Loss of function Stocking and glove pattern https: //youtu. be/mj. ARqy 9_i. Do? t=63 Motor weakness 1. Mild 2. the most distal intrinsic muscles of te hands and feet Ankle jerks absent

Painful Diabetic Neuropathy • Hypersensitivity to light touch • Severe “burning “ pain • Especially at nights

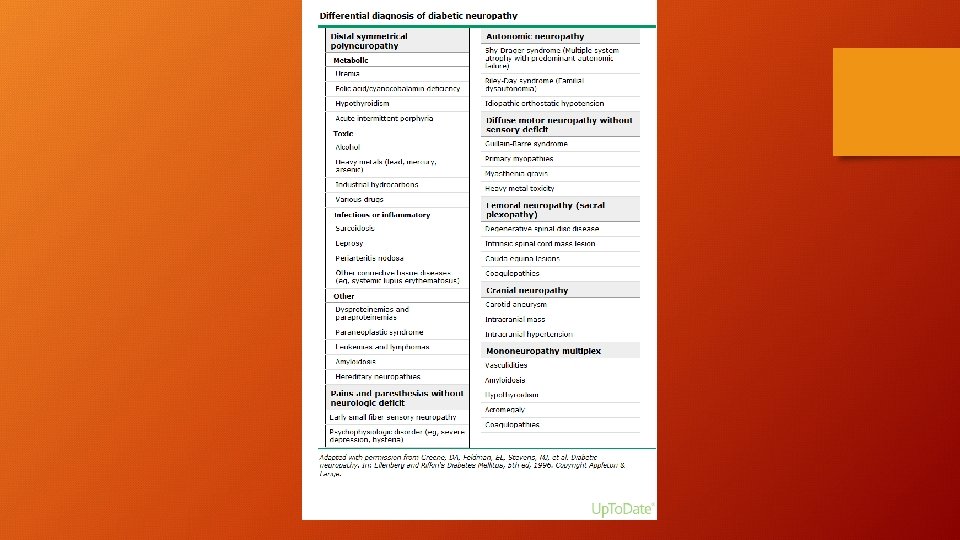
Investigations • Nerve conduction studies are not usually necessary • Determine progression • Determine severity • Detect other conditions, superimposed mononeuropathies such as carpal tunnel syndrome • ALWAYS CHECK FOR OTHER CAUSES OF NEUROPATHY
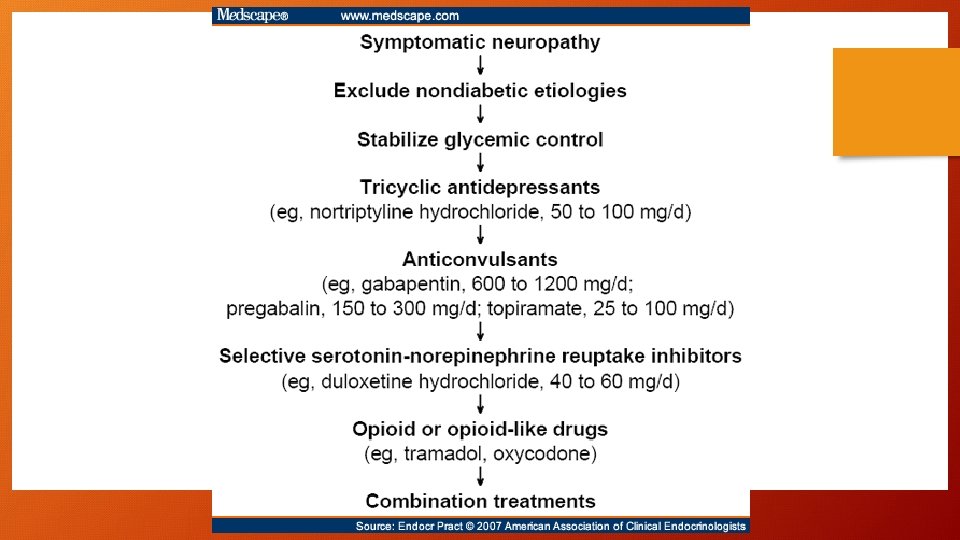

Treatment in DM patients with CKD • Dosages and dosing intervals often need to be adjusted • Side effect profiles can be more severe and distinct • Little evidence of the treatment effectiveness in patients particularly on dialysis and stage 4 -5 CKD

Pregabalin • one of the two agents currently approved for the treatment of pain associated with diabetic peripheral neuropathy • Acts by binding to the α 2 -δ subunit of L-type voltage gated calcium channels and decreasing calcium influx. • 300 -600 mg/day • Unlike gabapentin, pregabalin has better GI absorption and can be administered twice per day. • Rapid (< two weeks) onset of maximal pain relief • 150 mg daily dose is generally ineffective • However, side effects such as dizziness, ataxia, sedation, euphoria, ankle edema, and weight gain may limit its use.

Pregabalin • A 50% reduction in pregabalin daily dose is recommended for patients with Cr. Cl between 30 and 60 m. L/min compared to those with Cr. Clr > 60 m. L/min • Daily doses should be further reduced by an additional 50% for each additional 50% decrease in Cr. Cl • Pregabalin is rapidly cleared by hemodialysis • Supplemental pregabalin doses should be given to patients after each hemodialysis treatment to patients on maintenance hemodialysis to maintain steady-state plasma pregabalin concentrations within desired ranges. • Each 4 -hour hemodialysis session removes approximately 50% of the drug from the body, therefore 50 mg will need to be replaced after each dialysis session

Gabapentin • Also binds to the α 2 -δ site of L-type voltage gated calcium channels. • In general, gabapentin ≤ 2400 mg/day is effective in treating diabetic peripheral neuropathy in patients with normal kidney function • Is cleared solely by renal excretion and is not bound to plasma proteins • It is recommended that total dose does not exceed 1400 mg/day for a Cr. Cl of 30 -60 ml/min given in two doses, • 700 mg/day for a Cr. Cl of 16 -29 ml/min given in one or two doses and • 300 mg/day for Cr Cl of 15 ml/min taken in one dose. • For patients with a Cr. Cl less than 15 ml/min, the dose should be decreased in proportion to the decrease in the Cr. Cl

Gabapentin • Patients on maintenance dialysis receive an initial 300 -mg to 400 -mg gabapentin loading dose and then maintain plasma concentrations by receiving 200 -300 mg after every 4 hours of hemodialysis. • Titration to the maximal dose should be done gradually to avoid side effects, which include dizziness, ataxia, sedation, euphoria, ankle edema, and weight gain • The risks of myoclonus and altered consciousness due to gabapentin are increased in patients with stage 4 -5 CKD and in dialysis patients • Myoclonus in these individuals is more disabling than in patients with normal kidney function, and when it occurs, discontinuation of gabapentin is mandatory

Tricyclic Antidepressants The first line treatment in clinical practice- effective and inexpensive Inhibit the reuptake of norepinephrine and serotonin Control pain and pain related symptoms such as insomnia and depression Use limited by side effects Secondary amines (nortriptyline, desipramine) are better tolerated than tertiary amines (amytriptyline, imipramine) • Not well tolerated in older patients • Should be used with great caution (or avoided altogether) in patients with cardiac arrhythmias, congestive heart failure, orthostatic hypotension, and urinary retention, which further limits their use in dialysis patients • • •

Tricyclic Antidepressants • An electrocardiogram is mandatory before the initiation of treatment • Analgesic effects require several weeks to develop which limits their utility for acute pain • TCAs are contraindicated in patients taking monoamine oxidase (MAO) inhibitors • The usual dosage schedule for TCAs is 10 to 25 mg at bedtime initially, titrating as tolerated up to 100 or 150 mg as a single bedtime dose • no dose adjustments are needed in dialysis or CKD patients.

Duloxetine • the only other agent besides pregabalin that has been approved by the FDA for treating painful diabetic peripheral neuropathy • Serotonin-norepinephrine Reuptake Inhibitor • 60 mg and 120 mg daily • Nausea, orthostatic hypotension, tremor, anxiety and elevated blood pressure. • The presence of kidney impairment requires a lower starting dose of 30 mg and a more gradual titration with a maximum suggested dose of 60 mg daily. • The use of duloxetine is not recommended for a Cr Cl of < 30 ml/min.

Other Anticonvulsants • Phenytoin and carbamazepine primarily block the voltage gated sodium channel. • 200 -600 mg/day • However, due to quite serious side effects and newer improved therapies, their use is not recommended in patients with stage 4 -5 CKD or on renal replacement therapies

Opioids • multiple mechanisms including • peripheral, presynaptic, and postsynaptic-located opioid receptors in the dorsal horn and at • sites in the brain • the most common side effects are constipation, cognitive side effects, and nausea • Risk of drug abuse is a limiting factor for using these drugs in nonmalignant pain. • There is no general agreement on how opioids should be dosed, but usually, these drugs are dosed with short-acting opioids every 4– 6 h followed by a switch to long-acting opioids after 1– 2 weeks.

Opioids • Tramadol is a weak μ -receptor agonist that inhibits re-uptake of serotonin. • 200 -400 mg/day • Tramadol is well tolerated with a modest side effect profile that includes nausea, constipation, headache, and dyspepsia • In patients with stage 4 -5 CKD it is recommended that treatment should start at a lower dose and carefully titrate up to a maximum of 200 mg/day, with a dosing interval of 12 hours. • Since only 7% of an administered dose is removed by hemodialysis, dialysis patients can receive their regular dose on the day of dialysis.

Topical Agents • Capsaicin is an extract of capsicum peppers. Capsaicin binds to TRPV 1 receptor and exhausts substance P in the peripheral nerves to achieve it analgesic effects. • Burning was the most common side effect which tends to decrease as therapy is continued. The therapeutic effects of capsaicin are however modest and usuallymanifest weeks after the cream application. • Lidocaine 5% patches-Lidocaine blocks voltage-gated sodium channels, and topical application is thought to silence ectopic discharges on small afferent fibers by blocking sodium channels • data from RCTs in patients with painful diabetic peripheral neuropathy and CKD are not available. • Botulinum toxin, which has been shown to inhibit vanilloid receptors to inhibit release of glutamate and substance P, has also been shown to have a painrelieving effect in one randomized trial in patients with painful diabetic peripheral neuropathybut no data is available for stage 4 -5 CKD

Non-Pharmacological Therapies • Electrical nerve stimulation

A Patient We All See • 70 year old male with a 20 year h/o poorly controlled type 2 DM and HTN, dyslipidemia • 5 years ago diagnosed with nephropathy after urine screening positive for protein, last e. GFR 60 ml/min/1. 73 m 2 • Proliferative retinopathy sp laser photocoagulation 2 years ago • Developed an ulcer to right foot 1 year ago- has had recurrent debridements • Meds: Metformin 1 gm bid, 70/30 insulin 10 units sc bid, Lisinopril 40 mg od, carvedilol 3. 125 mg bid, ASA 81 mg od, Lasix 40 mg od • Main complaint at every clinic visit is numbness and tingling to both legs with occasional shooting pains.
- Slides: 36