The danger Numero Uno Thats how it reaches























 • Because the effect of patient adherence on the")











 with isoniazid")



- Slides: 40
The danger Numero Uno
That’s how it reaches you • Unprotected sexual intercourse • Intravenous drug abuse and shared needles • From a HIV positive mother to her infant during breastfeeding
No , Not this way
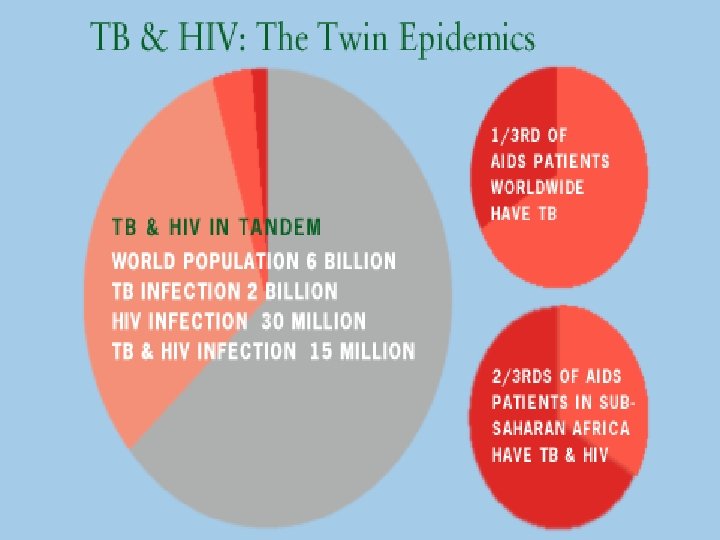
I am no less • World Population is six billion • Two billion have me • The Tubercle Bacilli.
Transmission and Pathogenesis • Prospective cohort studies have documented high rates of TB (5 -10% per year) among HIV infected populations, particularly injection drug users. Exogenous re infection with another strain of M. tuberculosis has been documented in patients with advanced HIV disease.
• The risk of TB has been estimated to be over 9 times greater in HIV positive compared with HIV negative persons who have a positive tuberculin test. • Outbreaks of TB, including multi-drug resistant disease, have highlighted the speed with which HIV infected patients progress to active TB after recent infection with M. tuberculosis.
Double Trouble HIV alters the pathogenesis and clinical presentation of TB. The frequency of extra pulmonary TB increases with low Cd 4 (70% with less than 100 count) The clinical and radiographic presentation may be atypical.
TB and HIV • HIV positive patients with TB have a significantly higher mortality when compared to HIV negative cases. • Delays in the diagnosis of TB have been associated with worse outcomes, so initiation of treatment as soon as TB is suspected is very important.
TB and HIV • While initial studies emphasized the impact of HIV on the natural progression of TB, recent studies have demonstrated that TB may alter the natural history of HIV disease. • Viral load has been shown to increase in the setting of active TB and decrease with appropriate therapy. Furthermore, HIV patients with TB have been shown to die sooner and develop AIDS faster than HIV-1 -infected controls without TB.
When to Suspect • All patients should be questioned regarding : • close contact with a person who has MDR TB • previous residence in a country where drugresistant TB is common; • previous treatment for TB, especially if it was incomplete; • previous residence in an institution (e. g. prison, homeless shelter) with documented transmission of a drug-resistant strain of TB.
Mantoux Screening • Tuberculin skin testing should be done using the Mantoux method in all HIV patients. • A tuberculin reaction of > 5 mm of indurations is classified as positive in persons known to have or suspected of having HIV infection.
Mantoux Screening • Unfortunately, as the CD 4 lymphocyte count declines with progression of HIV , many patients no longer react to delayed-type hypersensitivity testing. • More than 60% of persons with CD 4 lymphocyte counts of < 200 cells/µl may have skin test reactions of < 5 mm. • Thus, it is impossible to detect the presence of tuberculosis infection in many HIV.
Anergy Testing • In the past, anergy testing has been used to try to distinguish false negative from true negative tuberculin reactions. • However, recent data have documented limitations in the usefulness of anergy testing in public health tuberculosis screening programs. • Therefore, anergy testing in conjunction with tuberculin skin testing is no longer recommended for inclusion in screening programs for M. tuberculosis infection among HIV infected persons.
Evaluation • All patients who have a positive tuberculin skin test should have a chest radiograph performed to rule out active disease. • Patients should be asked about any symptoms which suggest the presence of active TB. • Persons who are found to have an abnormal chest radiograph and/or are symptomatic should be evaluated for the possibility of active disease by sending three sputum specimens for AFB smear and culture.
TB and HIV • Patients with advanced HIV-1 disease are more likely to have an extrapulmonary site involved and atypical radiographic presentation such as lower lobe involvement and intrathoracic adenopathy. It is important to note that HIV-1 infected patients with pulmonary TB may have a normal chest radiograph.
Lymphadenopathy
Large right paratracheal lymphadenopathy
Bilateral diffuse small nodules
Radiological Picture
Radiological Picture
Bilateral diffuse opacities with hilar adenopathy
Post Primary disease
Treating TB • HIV infected patients with TB respond well to ATT, as long as the regimen contains INH and rifampin. • A 6 -month regimen consisting of INH, rifampin, pyrazinamide, and either ethambutol or streptomycin given for 2 months followed by INH and rifampin for 4 months is the preferred treatment for drug-susceptible organisms. • Pyrazinamide should be continued for the first 2 months regardless of the results of drug-susceptibility testing, whereas ethambutol can be stopped after drug susceptibility test results indicate that M. tuberculosis is sensitive to INH and rifampin.
Treatment of TB (Contd. ) • Because the effect of patient adherence on the outcome is much more critical, directly observed therapy (DOT) is strongly recommended for persons with HIV infection. • ATT should be supplemented with pyridoxine (B 6). • Patients should be monitored closely for adverse reactions
ARV and ATT • Ask HIV infected about antiretroviral therapy use and specifically whether they are currently taking protease inhibitors (PIs) or non-nucleoside reverse transcriptase inhibitors (NNRTIs). • CD 4 lymphocyte count and viral load should be measured to assist with the treatment of the underlying HIV infection.
Paradoxical Reaction • Occasionally, patients with TB may experience a temporary exacerbation of symptoms after beginning TB treatment. • This is known as a paradoxical reaction (or immune reconstitution syndrome) These reactions are often related to the simultaneous administration of both ARV and ATT’s.
Paradoxical reaction-diagnosis • The diagnosis of a paradoxical reaction should be made only after a thorough evaluation has been made to exclude other etiologies. • Some patients have required the use of corticosteroids (in addition to TB treatment) to treat these reactions. • The decision to use corticosteroids must be made on a case-by-case basis. • Indications may include severe hypoxemia, airway obstruction, neurologic impairment, or possibly enlarged painful lymph nodes.
Monitoring Response to Treatment • Because the margin of error for treatment failure and relapse is probably less in HIV, the 6 -month regimen should be considered the minimum duration of treatment.
Monitoring Response to Treatment • Patients having a delayed response to treatment should have treatment prolonged from 6 to 9 months. • Malabsorption of the ATT drugs should be considered as a possible cause of treatment failure or the acquisition of drug resistance, particularly if gastrointestinal symptoms or chronic diarrhea is present.
Treatment of TB in Patients with CD-4 count<100/µL • They should NOT be treated with once- or twiceweekly regimens. • These patients should receive daily therapy during the first 2 months, and then daily or threetimes weekly therapy during the next 4 months. • This recommendation is based on a recent study showing an increased rate of acquired rifamycin resistance among patients who received twiceweekly therapy. • All patients with advanced AIDS and TB should be treated by DOT.
TB Treatment & Antiretroviral Treatment • Potent antiretroviral agents are now available for the treatment of HIV infection. These agents are classified as nucleoside/nucleotide (NRTI/Nt. RTI) or nonnucleoside reverse transcriptase inhibitors (NNRTI) , protease inhibitors (PI)and Fusion inhibitors. • The nucleoside agents do not have clinically significant drug interactions with the standard antituberculosis medications. • However, the PIs and NNRTIs may inhibit or induce cytochrome P-450 isoenzymes (CYP 450) and thus, these drugs may alter the serum concentration of the rifamycins.
ATT and ARV • The rifamycins induce CYP 450 and may substantially decrease blood levels of the antiretroviral drugs resulting in the potential development of resistance to these important agents. • The potential benefit of the antiretroviral drugs must be weighed against the importance of rifamycins in treating HIV related tuberculosis. • The loss of a rifamycin from the treatment regimen is likely to delay sputum conversion, prolong the duration of therapy, and possibly result in a poorer outcome
ATT and ARV • Previous guidelines specifically stated that rifampin was contraindicated for patients who were taking any PI or NNRTI. • New data indicate that rifampin can be used for the treatment of tuberculosis in several situations
ATT and ARV • Other issues in the guidelines to be aware of are: • the rifabutin dose should be reduced to 150 mg two or three times per week when given with ritonavir • The dose of rifabutin should be increased to 450 mg or 600 mg daily or 600 mg two or three times per week when rifabutin is used concurrently with efavirenz • Rifabutin can be used with many protease inhibitors, but doses of both the protease inhibitors and rifabutin may need to be altered.
ATT and ARV • In some patients, use of ATT regimens containing no rifamycins may be considered. • For such patients, a 9 -month, largely intermittent, regimen consisting of isoniazid, streptomycin, pyrazinamide and ethambutol for 2 months then isoniazid, streptomycin, and pyrazinamide for 7 months is an option.
Treatment of Latent TB Infection • Treatment of latent tuberculosis infection (LTBI) with isoniazid (INH) is very effective in preventing persons infected with M. tuberculosis from developing tuberculosis, regardless of HIV. Rifampin and pyrazinamide is not recommended for reasons of heptotoxicity • Recent studies have also documented no significant reduction in TB among anergic individuals who took INH. • HIV persons should be treated for LTBI if they have a tuberculin skin test > 5 mm and have not previously received treatment for LTBI.
Treatment of LTBI • In certain cases, treatment of LTBI in persons who are not tuberculin positive may also be considered. Such therapy may be beneficial for: • close contact to an infectious case • persons with a history of prior untreated or inadequately treated TB who have fibro nodular opacities on a chest radiograph (if active TB is ruled out) • HIV infected adults who reside or work in institutions and are continually and unavoidably exposed to patients who have infectious TB
Treatment of LTBI • The current CDC recommendations include several options for treatment of LTBI in HIV-1 -infected persons: • INH (300 mg/day) for 9 months, either daily or twiceweekly (900 mg biw) • Therapy should be supplemented with pyridoxine (25 -50 mg a day) to help prevent peripheral neuropathy • rifampin daily for 4 months. Rifabutin may be substituted for rifampin • When treatment is provided with isoniazid twice a week, therapy should be given under direct observation. delavirdine cannot be given with either rifampin or rifabutin.
Thank You Dr. Rakesh Bharti, MD, rakeshbharti 1@rediffmail. com