The Confusion about Confusion Its Not all Alzheimers

The Confusion about Confusion: It’s Not all Alzheimer’s Disease Marianne Smith, Ph. D, RN, FAAN Associate Professor, University of Iowa College of Nursing

Goals for Today v List 2 key characteristics of common types of dementia v Identify which types don’t have memory loss as an initial problem v Discuss type of dementia in the context of the Need-Driven Dementia model v Increase awareness that ASSESSMENT is key to problem-solving!!!
 üBehaviors rarely “come out of nowhere”")
“Reframe” BPSD v Need-Driven Dementia-Compromised Behavior Model (NDB) üBehaviors rarely “come out of nowhere” üBehavior is “communication” of unmet needs üCaregivers must “listen” with all senses üConsider impact of ENVIRONMENT v. Ask: What is really going on?
 Model Background/ Individual factors ü Cognitive function ü Physical function")
Need-Driven Dementia-Compromised Behavior (NDB) Model Background/ Individual factors ü Cognitive function ü Physical function ü Longstanding personality ü Habits, traits Proximal/ Environmental factors ü Physical needs ü Psychological needs ü Social environment ü Physical environment Behavioral & Psychological Symptoms

NDB: Two domains interact v Relatively stable Individual Factors üLong-standing personality üIndividual coping üDisease-related losses, health status v Fluctuating üPersonal üSocial üPhysical Environmental Factors Hmmm… sounds like basis for “Person Appropriate” care!

Take time to assess unmet needs! v Determine and document frequency, duration, intensity, and characteristics of each problem behavior v Identify, assess, treat or eliminate ANTECEDENTS and TRIGGERS

Normal Aging: Memory Three main components interact. . . v Attention v Working memory (aka short-term memory) v Long-term memory Remember!! Cognition is much more than memory!!!!

Memory at work Can they see and hear well enough to get the information in the first place? ? ?

Normal Aging v Attention: Attending to some stimuli while disregarding others v Think of attention as a “highlighter” ü Highlighted section stands out You focus on that area ü You "tune out" information that isn’t relevant v Normal aging changes ü Slower in responding to “target” ü Slower to divide or switch attention ü Difficulties with tasks that require flexible control of attention

Normal Aging Working memory: Active manipulation of information; aka shortterm memory v Normal aging changes v ü General slowing of information processing ü Interferes with complex everyday tasks

Cognition: Normal Aging v Long-term memory: Retrieval of information no longer present or in an active state ü Several components to long-term memory ü Some aspects decline and others stay the same v Normal aging changes ü Episodic memory: personally experienced events «What, where, when of our daily lives «Encoding, storage, retrieval decline over time = forgetfulness
 v")
Normal Aging Most common challenges v Learning something new (takes more time, repetition) v Doing more than one task at a time v Shifting focus between tasks v Forgetfulness due to changes in episodic memory

Normal Aging Leads to memory “problems” v. Where I parked the car v. Name of people, places v. Intended task (go upstairs, forget why there) v. Memory often “returns” with time (e. g. , go back downstairs and you remember what you were trying to retrieve upstairs!) Annoying, but not disabling!

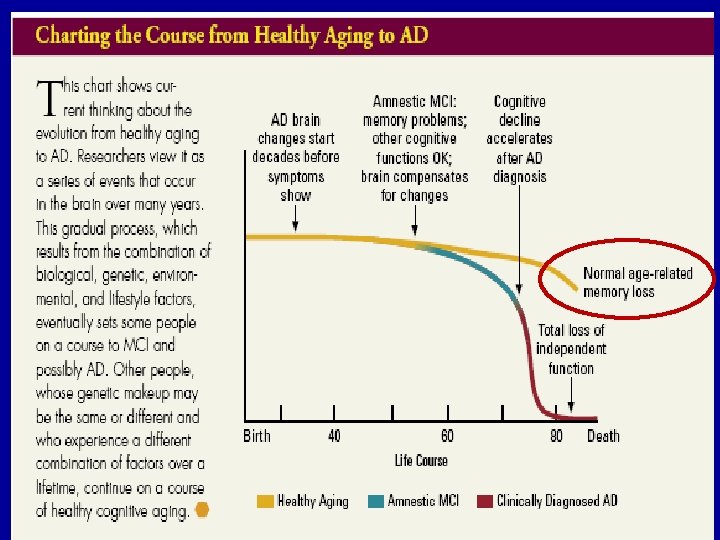
Normal age-related memory changes Symptoms that may indicate dementia Able to function independently and pursue normal activities, despite occasional memory lapses Difficulty performing simple tasks (paying bills, dressing appropriately, washing up); forgetting how to do things you’ve done many times Able to recall and describe incidents of forgetfulness Unable to recall or describe specific instances where memory loss caused problems May pause to remember directions, but doesn’t get lost in familiar places Gets lost or disoriented even in familiar places; unable to follow directions Occasional difficulty finding the right word, but no trouble holding a conversation Words are frequently forgotten, misused, or garbled; Repeats phrases and stories in same conversation Judgment and decision-making ability the same as always Trouble making choices; May show poor judgment or behave in socially inappropriate ways

Normal Aging Most compelling fact about age-related cognitive change VARIBILITY v Cognitive DECLINE is not inevitable v Many factors contribute v ü Biological ü Psychological ü Health-related ü Environmental ü Lifestyle Active lifestyles are generally associated with better outcomes! Aerobic exercise benefits cognition!

Dementia v Permanent loss of mental abilities caused by damage to brain cells v NOT a “normal” part of aging! v The common end result of many entities üdiseases ütraumas üinfections üdrugs
 v MEMORY impairment AND one or more of the following üAgnosia:")
DSM-IV Criteria (2000) v MEMORY impairment AND one or more of the following üAgnosia: recognition of objects üApraxia: ability to move üAphasia: use of language üDisturbance in executive functioning: ability to organize, plan, sequence, abstract v Gradual onset; impaired function

Neurocognitive disorders: DSM 5 v NCD replaces the DSM-IV category “Dementia, Delirium, Amnestic, and Other Cognitive Disorders” üTerm Dementia replaced with Major Neurocognitive disorder üMinor Neurocognitive disorder added (formerly called Mild Cognitive Impairment) üTerm “dementia” is retained in DSM-5 and not precluded from use in clinical practice

Mild and Major NCD v Memory is not the primary symptom v Six main domains of function üComplex attention üExecutive function üLearning and memory üLanguage üPerceptual-motor üSocial cognition Important to understand in order to recognize changes that AREN’T MEMORY!!

Neurocognitive Domains Complex Attention v Sustained attention v Divided attention v Selective attention v Processing speed Early Observations v Easily distracted v Difficulty in settings with multiple stimuli v Problems holding information in mind, repeating what was just said v Difficulties focusing

Neurocognitive Domains Executive Function v Planning v Decision-making v Working memory v Responding to feedback/error correction v Overriding habits/inhibition v Mental flexibility Early Observations v Gives up on/ withdraws from complex projects v Needs to focus on one task at a time v Relies on others for planning, making decisions

Neurocognitive Domains Learning & Memory v Immediate memory v Recent memory ü Free recall ü Cued recall ü Recognition memory v Long-term memory ü Semantic facts ü Autobiographical personal events, people ü Implicit/procedural unconscious learning of skills Early Observations v Repeats self, often in same conversation v Tracking problems, even with lists v Needs frequent reminders, cues v Difficulty recalling events v Loses track of dates, events, payments

Neurocognitive Domains Language v Expressive Language ü Naming ü Word-finding ü Fluency ü Grammar/syntax omissions or incorrect use of words v Receptive Language ü Comprehension: actions in response to verbal command EARLY OBSERVATIONS v. Uses general phrases “that thing” v. Pronouns vs. names “her/him” vs. family member’s name v. Stereotypical, idiosyncratic language what-cha-macall-it; thing-a-ma-jig
![Neurocognitive Domains Perceptual-Motor v Visual perception v Visuo-constructional v Perceptual-motor v Praxis [learned movements]](http://slidetodoc.com/presentation_image_h2/99cb494f642c093bec655039874cf6ac/image-25.jpg "Neurocognitive Domains Perceptual-Motor v Visual perception v Visuo-constructional v Perceptual-motor v Praxis [learned movements]")
Neurocognitive Domains Perceptual-Motor v Visual perception v Visuo-constructional v Perceptual-motor v Praxis [learned movements] v Gnosis [awareness, recognition, such as faces, colors] Early Observations v Difficulties with previously familiar activities tools, hobbies, driving v Problems navigating familiar environments v Misperceptions in low light

Neurocognitive Domains SOCIAL COGNITION v. Recognition of emotions v. Ability to understand another person’s mental state Early Observations v Behavior clearly outside acceptable social range v Insensitivity to social standards ü Modesty of dress ü Political, religious, sexual topics v v Disregards feedback Lack of insight

Minor Neurocognitive Disorder v Evidence of modest cognitive decline from previous level in one or cognitive domain v Deficits don’t interfere with independence üComplex IADL function is preserved üCompensatory strategies, greater effort or accommodation may be required v May/may not signal onset of more severe decline (e. g. Major NCD)
 üRecognized for over a decade üPersistent,")
Mild Cognitive Impairment v Mild Cognitive Impairment (MCI) üRecognized for over a decade üPersistent, troublesome problems; forgets facts quickly; poor recall of reading or poor recall of details of simple drawings; forgets important events repeatedly üNo changes in judgment or reasoning

Mild Cognitive Impairment M v Subjective complaints of defective memory v Objective tests show abnormal memory, compared to normal elderly adults v Normal ADL and other cognitive function v No evidence of delirium or dementia v High risk of progressing to Alzheimer’s disease!

Major Neurocognitive Disorder v Evidence of significant cognitive decline from previous level of performance in one or more domains: ü Complex attention ü Executive function ü Learning and memory ü Language ü Perceptual motor ü Social cognition v Interfere with independence in everyday activities (IADLs)

Confusion about AD vs. dementia v ALL Alzheimer’s Disease is dementia v NOT ALL dementia is Alzheimer’s type v Risk increases with advancing age ü 1 -2% of 65 year olds, but ü 30% of 85 year olds ü 50% of 90 year olds

NCD due to. . . Alzheimer’s disease v Vascular disease v Frontotemporal lobar degeneration v Lewy-Body disease v Traumatic brain injury v Types HIV disease v Prion disease v Parkinson’s disease v Huntington’s disease v Substance/ medication use v Another medical condition v Multiple etiologies v Unspecified v
 v Most common ~ 50 -60% of all dementias v Pathology:")
Alzheimer’s Disease (AD) v Most common ~ 50 -60% of all dementias v Pathology: üNeurofibrillary tangles, Beta-amyloid plaques üProgressive decline due to cell death

Degenerative Changes
 criteria v Early Decline in memory & learning v Steadily progressive,")
Alzheimer’s disease (AD) criteria v Early Decline in memory & learning v Steadily progressive, gradual decline in cognition, without plateaus ü Early: Forgetful ü Confused: Disoriented, more memory ü Ambulatory: Increasing self-care deficits, behaviors ü Late: Loss of ability to speak, walk, swallow

Alzheimer’s Course Early Confused Ambulatory Memory changes are noticed by others! Late

Confused: Example v “Helen” croquets using a single simple stitch but doesn’t remember that she is retired - and sometimes puts her bra on over her blouse. v “Harold” greets everyone like his oldest friend (“Nice to see you! So good of you to drop by! I’m great! How are you? ”) but doesn’t know his own wife.

Confused: Example v “Mildred” avoids the question “How old are you” with “Jack Benny and I are both 29. ” When asked what she had for lunch, she replied, “I went to the Riviera and had pink champagne and caviar. ” v “George” got lost walking in his neighborhood of 30 years -- as soon as he could no longer see his own house.
 v Early Impaired judgement; problems making decisions, planning, and/or organizing")
Vascular disease (Va. D) v Early Impaired judgement; problems making decisions, planning, and/or organizing vs. memory loss v Hallmark brain changes üLarge vessel stroke to microvascular disease üLocation, size, number effect presentation «Step-wise decline with plateaus for some «Progressive decline for others

Vascular Dementia Cerebrovascular, cardiovascular disease Ischemic, hypo- perfusive, or hemorrhagic brain lesions Small brain attacks (infarcts) Loss of brain tissue Dementia Risk factors v Smoking v Obesity v Hypertension v CVA v Arteriosclerosis v Atrial fibrillation v Cardiac valve replacement v Diabetes
 v Early üFluctuating attention, alertness, ability to understand visual information üVisual")
Lewy-Body Disease (LBD) v Early üFluctuating attention, alertness, ability to understand visual information üVisual hallucinations üMovement changes: tremors, stiffness, slowness, difficulty walking üSleep disturbance (acting out during sleep)

Lewy Body Disease v Hallmark brain changes ü Lewy bodies: Abnormal protein depletes dopamine ü Progressive course v Three common presentations ü Parkinson’s disease is first, then cognitive impairment = NCD due to Parkinson’s disease ü Distinctive features lead to early LBD dx ü Mistaken for AD; later diagnosed as LBD

Lewy Body Disease v Other considerations üAutonomic nervous system changes «Blood pressure control «Temperature regulation «Bladder/bowel function üAntipsychotic medications are not tolerated «Severe worsening of movement «Potentially fatal neuroleptic malignant syndrome (NMS) risk üSignificant fall risk d/t gait changes

Characteristics of Dementia Subtypes Dementia type Memory Executive Visuospatial Attention Parkinsonia Impairment deficit n signs AD +++ + ++ - - Va. D + +++ -/+ - + Lewy body dementia + + +++ +++

Frontotemporal Dementia v Early ü Significant personality and behavior changes vs. memory ü Impaired judgment, self-care, empathy, insight, language ü Learning/memory and perceptual-motor function spared v Hallmark brain changes ü No distinguishing microscopic abnormalities in ALL ü Pick cells (Pick’s disease) in some ü Evidence of disproportionate frontal and/or temoral lobe involvement from neuroimaging
 ü")
Frontotemporal Dementia v Other considerations ü Younger age at onset (40 -60 years) ü Shorter survival compared to AD ü Considered the most stressful type of dementia v Behavioral variant ü Behavioral disinhibition ü Apathy or inertia ü Loss of sympathy or empathy ü Perseveration, stereotyped, or compulsive/ritualistic behavior ü Hyperorality and dietary changes

Frontotemporal Dementia v Language variant: Prominent decline in language ability ü Speech production ü Word finding ü Object naming ü Grammar ü Word comprehension v Like AD Insidious onset, progressive course

NCD due to. . . Alzheimer’s disease v Vascular disease v Frontotemporal lobar degeneration v Lewy-Body disease v Traumatic brain injury v Types HIV disease v Prion disease v Parkinson’s disease v Huntington’s disease v Substance/ medication use v Another medical condition v Multiple etiologies v Unspecified v

NCD due to Traumatic Brain Injury v Impact to the head; other rapid movement/displacement of the brain within the skull, resulting in üLoss of consciousness üPost-trauma amnesia üDisorientation and confusion üNeurological signs [positive neuroimaging] v Presents immediately and persists past acute injury recovery

NCD due to Traumatic Brain Injury v Key considerations üOnset is clear: time of injury üEmotional issues Irritability, frustration, tension, anxiety, lability üPersonality changes Disinhibition, apathy, suspiciousness, aggression üPhysical Headache, fatigue, sleep disturbance, dizziness, reduced tolerance to psychotropic medications

Substance/medication induced NCD v Involved substance or medication AND duration of use are capable of producing impairment üAlcohol üInhalants üSedative, hypnotic, anxiolytic üOther (or unknown) substance v Impairment persists beyond usual duration of intoxication/acute withdrawal

Substance/medication induced NCD v Key considerations üPrevalence is not known üEmotional Irritability, anxiety, sleep disturbance, dysphoria üNeuromotor Incoordination, ataxia, motor slowing üLoss of emotional control Aggressive or inappropriate affect, apathy

NCD due to. . . Alzheimer’s disease v Vascular disease v Frontotemporal lobar degeneration v Lewy-Body disease v Traumatic brain injury v Types HIV disease v Prion disease v Parkinson’s disease v Huntington’s disease v Substance/ medication use v Another medical condition v Multiple etiologies v Unspecified v

Dementia: Types v LOTs of variability in presentation! üWithin specific types. . . üBETWEEN types. . . v Overlapping syndromes are common üDementia AND delirium üDementia AND depression üMixed dementia

Dementia Onset v Memory impairment is NOT the first change in all types of dementia! üVa. D: Judgment; making decisions; planning, organizing üLBD: Fluctuating confusion, hallucinations, tremor, stiffness, slowness üFTD: Personality and behavioral disturbances

But FIRST, is the problem dementia? ? ? Background/ Individual factors ü Cognitive function ü Physical function ü Longstanding personality ü Habits, traits Proximal/ Environmental factors ü Physical needs ü Psychological needs ü Social environment ü Physical environment Behavioral & Psychological Symptoms

“Reversible” Dementia v Multiple health problems may cause “confusion” v Always explore alternative causes v Treatment of underlying physical problem may arrest losses v Problems not fully “reversible” but remaining capacity may be preserved

D-E-M-E-N-T-I-A D rugs E motion M etabolic E ndocine N utrition T rauma I nfection A lcoholism Like working a puzzle. . .

Always consider delirium! v Delirium can overlap on dementia! Check it out! üInfection üHypoxia üMetabolic üEndocrine üSensory deficits üMedications Dementia Delirium “Reversible” dementia is often caused by delirium!!

Delirium: Contributing factors v Predisposing factors = put elders at risk! üCognitive impairment/Dementia üMultiple health problems So on a “good üAdvanced age day” most üDehydration LTC residents are at risk for üMalnutrition delirium!!! üVision/hearing impairment üImmobilization üFunctional impairments

Delirium: Contributing factors v Precipitating factors = Triggers üMedications üInfections üPain üUnfamiliar environment üElectrolyte imbalance üProcedures/surgery üRestraints And every new health problem or change can tip the balance!!!
 v")
Delirium: Criteria v Disturbance in ATTENTION and awareness (reduced orientation to the environment) v RAPID ONSET of symptoms representing a change from baseline attention & awareness v Symptoms tend to FLUCTUATE in severity during the course of the day

Delirium: Criteria v COGNITION disturbance üMemory deficit üDisorientation üLanguage disturbance üVisuospatial disturbance üPerception (hallucinations, delusions, illusions) v Consequence of medical condition, substance, toxin, or multiple etiologies
 Symptoms (+) Delirium: Fluctuating course")
De Lira = Latin for “Off the track” (-) Symptoms (+) Delirium: Fluctuating course Morning Afternoon Night

Causes: I-WATCH-DEATH I nfections W ithdrawal A cute metabolic T rama C entral nervous system pathology H ypoxia D eficiencies E ndocrinopathies A cute vascular T oxins/drugs H eavy metals
 üItems reflect diagnostic criteria üTry This v Delirium")
Assessment v Confusion Assessment Method (CAM) üItems reflect diagnostic criteria üTry This v Delirium Observation Scale üChecklist format preferred by UIHC nurses v Goal is to understand how to use the scale and use it consistently!!
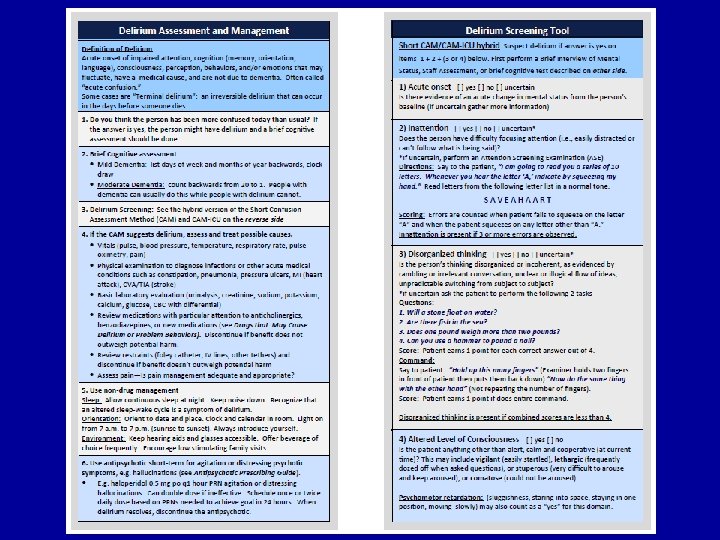

Try this: CAM http: //consultgerirn. org/resources
 69 13 items observed each of 3 shifts: day, evening,")
Delirium Observation Scale (DOS) 69 13 items observed each of 3 shifts: day, evening, night: ü Dozes off during conversation or activities ü Is easily distracted by stimuli from the environment ü Maintains attention to conversation or action** ü Does not finish question or answer ü Gives answers that do not fit the question ü Reacts slowly to instructions ü Thinks he/she is somewhere else ü Knows which part of the day it is ** ü Remembers recent events ** ü Is picking, disorderly, restless ü Pulls IV tubes, feeding tubes, catheters etc. ü Is easily or suddenly emotional (frightened, angry, irritated) ü Sees/hears things which are not there Scoring: ü Never = 0 points; Sometimes or always = 1 point. ** items are reverse scored ü A total score of three or more points indicate a delirium

Growing evidence for 1 question Is the person more confused today than USUAL? If Yes, then use CAM!!! (Or other full assessment!)

71

Depression DEMENTIA DEPRESSION 30% with both! Depressive Disorder Alone or overlapping with dementia

Key Differences DEPRESSION DEMENTIA Onset Weeks/months Months to years Course Persistent 1 Slow, progressive Reversible Most (80%) Not reversible Affects Mood Memory Cognitive Focal Global Cause Stress, genetics AD, vascular Tx Immediate 2 Ongoing 1. Often chronic in the absence of treatment 2. May be ongoing for those with severe/recurrent episodes

Dementia & Depression Problems that are common to both v Loss of interest in once-enjoyable activities and hobbies v Social withdrawal DEMENTIA v Memory problems v Sleep disturbance v Impaired concentration DEPRESSION (30%)
 Symptoms (-) Depression: Course Weeks to Months (up to 2 years)")
(+) Symptoms (-) Depression: Course Weeks to Months (up to 2 years)
")
Depression Screening Tools Geriatric Depression Rating Scale: 15 -30 yes/no items (Try This series) v Cornell Scale for Depression in Dementia: 19 items v Patient Health Questionnaire: 9 item OR 2 -item v

Patient Health Questionnaire 1. 2. 3. 4. 5. 6. 7. 8. 9. Little interest or pleasure in doing things Feeling down, depressed or hopeless Trouble falling or staying asleep, sleeping too much Feeling tired or having little energy Poor appetite or overeating Feeling bad about yourself, feeling like a failure Trouble concentrating on things, such as reading the newspaper or watching television Moving or speaking slowly, or being restless and moving around more than usual Thoughts that you would be better off dead or of hurting yourself in some way

PHQ-9 Scoring Score each item: 0=Not at all 1=Several days 2=More than half the days 3=Nearly every day v Total each column (0 to 3) v Add across columns to get a total score: 0 to 27 v v Apply cut-points: ü 0 to 4 – depression is not significant ü 5 to 9 – mild depression ü 10 to 14 – moderate depression; any score over 10 is considered clinically significant/ worthy of treatment ü 15 or greater – severe depression

Assessment: What is going on? ! v First and foremost How well do you know the person? üDetecting change in status relies on knowing BASELINE!! üWhat is typical? Usual? Common? For this person! üIf you don’t know, who does?

Assessment: What is going on? v New physical health problem? v Reoccurring health problem? v Fluctuating problem? v Persistent problem? v Part of “normal range” for this person? v “Not at all like” the person? v What additional information is needed?

Assessment: More than cognition! History: past psychiatric, medical disorders v Symptoms: onset, duration, change v Medication history v Physical exam v Mental status exam v CBC v Urinalysis v T 3, T 4, TSH v B 12 and folate v Chem screen: Na, Cl, K, BUN, Ca, Glucose, Creatinine v Electrocardiogram v Rule out reversible causes of confusion! (Delirium)
 ü")
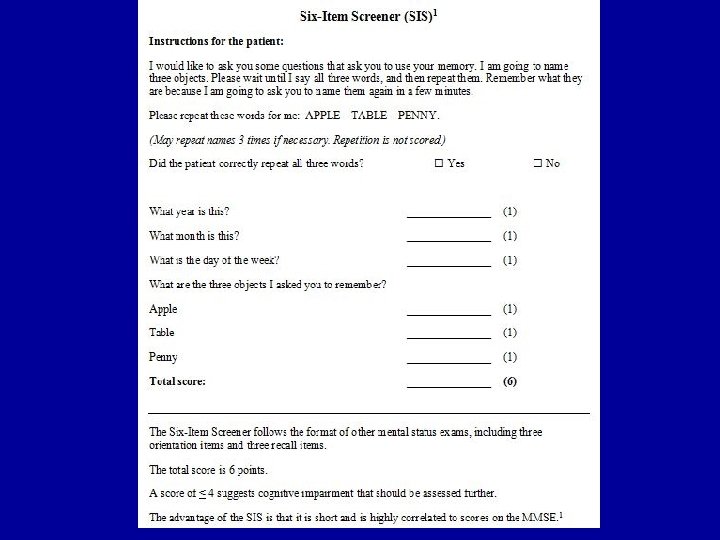
Screening tools v Mini-Cog: ü Three item recall ü Clock Drawing Test (CDT) ü http: //alzheimers. about. com/od/diagnosisissues/a/Mini _Cog. htm (quick info with additional links) Clock drawing v Six item screener: v ü Three item recall (apple, table, penny) ü Three orientation items (year, month, day)

Clock Drawing Test v Construction: ability to accurately reproduce simple objects v Visual fields: visual-spatial changes v Abstraction: conceptualization: “time” is an abstract concept

Sunderland, T, Hill, JL, Mellow, AM, Lawlor, BA, Gundersheimer, J, Newhouse, PA, & Grafman, JH. (1989) Clock Drawing in Alzheimer’s Disease. A Novel Measure of Dementia Severity. J AM Geriatri Soc. Aug: 37(8): 725 -9.

MMSE is widely used in practice Gold standard for brief cognitive evaluations Challenges are associated with copyright issues that were not imposed early, but are an increasing concern!
 Scoring: • 0 -30 possible • ≥ 26")
Montreal Cognitive Assessment Tool (Mo. CA) Scoring: • 0 -30 possible • ≥ 26 normal

Further Diagnostic Assessments v Repeated assessments: Deficits/strengths üNeuropsychological testing related to performance on specific test of ability üImaging studies to identify brain changes that are consistent with dementia/types or stages of dementia üOccupational therapy assessments related to abilities/safety to perform ADL/IADLs and strategies to support living alone
 What additional information would")
Case Studies Read the cases and answer these questions: 1) What additional information would you like to have to understand the person’s health status/behavior? 2) Which signs/symptoms are characteristic of cognitive decline/impairment? Is there another possible explanation? 3) Which signs/symptoms would you report to the primary care provider and/or discuss with family?

Summary: Think about interactions!!! Background/ Individual factors ü Cognitive function ü Physical function ü Longstanding personality ü Habits, traits Proximal/ Environmental factors ü Physical needs ü Psychological needs ü Social environment ü Physical environment Behavioral & Psychological Symptoms
- Slides: 90