The Case of Mr P By dietetic intern

The Case of Mr. P By dietetic intern: Julia Whelan

Objectives: • Clinical rotation site • Pathophysiology/MNT of diseases • Review Mr. P • Discuss formula types • Discuss kidney decline and end of life care • Review Prostat supplementation • Discuss challenges • Review overall goals

Clinical Rotation Site: VAMC Orlando Community Living Center 120 bed facility available for veterans eligible to receive nursing home care The CLC offers the following services: • Skilled Nursing Care • Rehabilitation • Dementia Special Care • Hospice/ End of Life Care • Dementia Respite Care • Spinal Cord Injury Care Mission Statement: Our goal is to provide Veterans the opportunity to achieve optimal function in order to maintain or improve the quality of their lives

VAMC Orlando Community Living Center The role of the RD: • 3 dietitians total • • Work with an interdisciplinary team to care for residents • Collect food preferences • • Write diet, supplements, and tube feeding orders • Determine nutritional status • Create special food carts • Provide education to staff on various nutrition-related topics • Participate in wound care rounds, behavior rounds, and enteral nutrition rounds Provide and advocate for proper dental care of residents And always advocating for our veterans!

What’s to come at the Orlando VA: Lake Nona Hospital Opening Fall 2015: 134 bed inpatient treatment and diagnostic hospital Outpatient Clinics State of the art facilities Campus includes the domiciliary, the community living center, and a nursing simulation center Located in “medical city” alongside Nemours Children’s Hospital and the UCF Medical Hospital The first VA hospital built in the US since 1995
 The kidney function: maintain the balance of fluids, electrolytes, and")
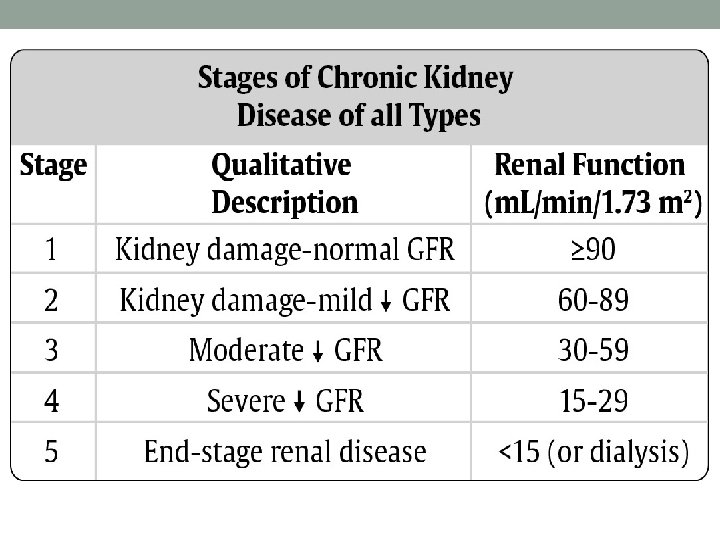
Chronic Kidney Disease (CKD) The kidney function: maintain the balance of fluids, electrolytes, and organic solutes in the body through the active process of reabsorption, filtration, and excretion
 Definition: the progressive decline of kidney function over time regardless")
Chronic Kidney Disease (CKD) Definition: the progressive decline of kidney function over time regardless of the underlying cause or disease Prevalence: 1 in 9 adults in the US Risk Factors: diabetes, hypertension, heart disease, obesity, high cholesterol, age, smoking Labs: Glomerular Filtration Rate (GFR); Blood Urea Nitrogen/ Creatine ratio

Chronic Kidney Disease MNT KDOQI Guidelines Limit Phosphorous 0. 8 -1. 7 g/d: balanced and excreted by the kidneys meats, dried beans, dairy, nuts, seeds, chocolate, colas, whole grains Limit Potassium 2. 4 -4 g/d: balanced and excreted by kidneys fruits, vegetables, dairy, meats, bread, pasta Limit Protein to 0. 6 -1 g/kg/d: dietary protein has been shows as a factor that increases glomerular pressure and leads to accelerated kidney decline Limit Sodium less than 2. 3 g/d: to minimize edema due to reduce fluid excretion

Secondary Hyperparathyroidism • Hyperparathyroidism secondary to a disease state such as CKD • An overproduction of PTH caused by several changes that occur in bone and mineral metabolism as a result of decreased kidney function which stimulate an increase in PTH synthesis and secretion 1. Deficiency of activated Vitamin D 2. Hyperkalemia • Leads to Renal Osteodystrophy- osteoclast activity, bone breakdown, and resorption leading to weakened bones
")
Cerebrovascular Accident (CVA)
 Definition: the blockage of blood to the brain that essentially starves")
Cerebrovascular Accident (CVA) Definition: the blockage of blood to the brain that essentially starves the brain of oxygen leading to dysfunction or death of tissue Prevalence: 3 rd most common death in the US, most common cause of disability in the US Risk Factors: old age, hypertension, smoking, obesity, coronary heart disease, diabetes, genetics, and lifestyle Diagnosing: CT scan, MRI, EKG
 MNT • Balanced diet- DASH • Limit saturated and trans fats")
Cerebrovascular Accident (CVA) MNT • Balanced diet- DASH • Limit saturated and trans fats • Promote fiber • Promote flavonoids, vitamins, and minerals • Provide adequate fluids • Assess and manage dysphagia • Enteral nutrition • Altered diet consistencies • Adaptive equipment

Mr. P • 73 year old male admitted to the CLC long-term continuous care on 12/29/14 • Transferred from Hunter’s Creek Skilled Nursing Facility • 100% Service Connected • Had 4 hospitalizations between 9/2014 -12/2014 • One for CVA • One for GI Bleed • Two for CHF exacerbation • Needed assistance completing majority of ADL’s • Goal at CLC: “receive continuous medical care in a safe environment”

Social History • Divorced from 1 st wife, widowed from 2 nd wife • Quit smoking cigarettes in 2004 • Previously smoked 1 pack/day for 10 years • Social drinker • Completed 1 -1 ½ years of college • Career: Military (Air Force 1959 -79) and Post Office • Hobby: building model airplanes • Power of Attorney: Daughter

Medical History 1. 2. 3. 4. 5. 6. 7. 8. CVA CHF HTN Diabetes Mellitus with Neuropathy Chronic Kidney Disease with Secondary Hyperparathyroidism GI Bleeding (hospitalized in last 3 months) Anemia of Chronic Disease Dyslipidemia 5. Hypothyroidism 6. Gout 7. GERD 8. Sleep Apnea--declines use of CPAP 9. Depression 10. Environmental Allergies 11. Constipation 12. Hx. of Falls 13. Hearing Impairment/Tinnitus 14. Folate Deficiency

Nutrition Assessment: Admission • Current Diet: No Concentrated Sweets, No Added Salt with Boost BID • Food Allergy: Shellfish • No diarrhea/constipation, nausea/vomiting, chewing/swallowing issues reported • Previous diet education unknown • Mild Nutritional Risk • Resident reported poor PO intake • BMI= 26 kg/m 2 • Wt= 175. 4 lbs (110% TBW) • Labs: • BG- low • BUN/Creat- low • K+- high • PO 4 - high

Weights:

Mr. P Timeline • January 2015 • 2 Falls- no injury • Shingles • Resident requested decreased medication load • Oxybutynin, Sennosides/Docusate, MVI, Folic Acid, Cholecalciferol, and Citalopram discontinued • F/U with Cardiology Clinic- noted chronic systolic compensated HF • Declined long-term dialysis • Labs: • H&H- low • Creat/BUN- high • Glucose- high

Mr. P Timeline • February 2015 • Right eye cataract surgery completed • Labs: • BG- wnl • March 2015 • Decreased insulin dose • Restarted anti-depressant • Started on laxative- constipation • Fall-no injury • Labs: H&H- low HDL- low BUN/Creat- high BG and A 1 C- wnl

Mr. P Timeline • April 2015 • Decreased insulin dosage • Decreased antihypertensive medication • 3 teeth extracted • CHF worsened • F/U with Cardiology Clinic: compensated with evidence of slight volume overload • cardiomegaly, mild prominence of pulmonary vasculature, left pleural effusion • 1 VT episode and 4 non-sustained VT episodes • Declines long term dialysis • Increasing edema and shortness of breath • Labs: BG- wnl Na/Cl- high BUN/Creat- high H&H- low

Mr. P Timeline • May 2015 • Fall- left ankle pain and swelling • Redness and 2+ edema; soft tissue swelling • Increased incontinence and urgency • Small non-infected blister of left big toe • Declined long-term dialysis • Strange behavior “not acting his normal, staring in space, and speech not clear” • Labs: • BG- wnl • Admitted to Osceola Regional Medical Center 5/26 • Dx CVA and Hyperkalemia

Mr. P Timeline • June 2015 • Resident returned to unit 6/5: • Right upper and lower extremity, left lower extremity • • weakness Speech minimal Left facial droop Incontinent Multiple skin issues: stage I pressure ulcers on heels and foot; and stage II on buttocks No swallowing issues with medications DNR Puree/Dysphagia diet, No Added Salt, No Concentrated Sweets, Honey Thick liquids • Mild Moderate Nutritional Risk

Mr. P Timeline • June 2015 • Not tolerating anything by mouth 6/6 • Vomiting, retching when meal arrived • Shortness of breath and dyspnea • Admitted to Osceola Regional Medical Center 6/6 • Aspiration Pneumonia • PEG tube placed- Nepro 30 ml/hr with a goal of 50 ml/hr • 20 Fr with mushroom internal fixator • Re-Admitted to CLC 6/12 • PEG tube: Nepro 40 ml/hr with 20 ml sterile water flushes • Tube insertion site at 4 cm • Positive for bowel sounds- last BM 6/11, incontinent • Soft, non-tender abdomen • Skin- left and right hand edema, right heel pressure ulcer, left buttock & right buttock erythema

Mr. P Timeline • June 2015 • Nepro rate increased to 50 ml/hr x 22 hrs on 6/13 • Frequent mouth care • Synthroid therapy • Residuals checks at each med pass- range 1 ml-12 ml • Normal BM 6/13, 6/16 • Edema continued in right hand • Increased water flushes to 30 ml/hr, continued 10 ml water flush with each medication to meet fluid needs on 6/15 • Wounds stable- no prostat • Meds clogging feeding tube: increased water via med pass to 20 ml with each medication; decreased automatic water flush to 25 ml/hr on 6/16 • Med pass- 10 ml to dilute, 10 ml to flush ~15 meds/day

Nepro at 50 ml/hr x 22 hrs with automatic sterile water flushes 25 ml/hr and 20 ml with each medication Nepro: 1. 8 kcal/ml; 81 g pro/L; 727 ml water/L • • 50 ml/hr x 22 hrs = 1100 ml/day = 1. 1 L/day 1. 8 kcal/ml x 1100 ml/day = 1980 kcals/day 81 g pro/L x 1. 1 L/day = 89. 1 g pro/day 727 ml water/L x 1. 1 L/day = 800 ml water/day Automatic Flushes: 25 ml/hr • 25 ml/hr x 22 hrs = 550 ml/day sterile water flushes Medications: 20 ml/medication • 20 ml/medication x 15 medications/day = 300 ml water/day Total: 1980 kcals; 89. 1 g pro; 1650 ml water Needs: Mr. P = 183. 5 lbs (83. 4 kg) 20 -25 kcal/kg = 1668 -2085 kcals/day 0. 9 -1. 1 g pro/kg = 75 -91. 74 g pro/day 20 -25 ml water/kg = 1668 -2085 ml water/day

Mr. P Timeline • June 2015 • Diarrhea 6/16 -6/18 about 5 x/day • Residuals averaged 0 ml • Lead to opening of wounds to left, right and middle of buttocks • 6/18 began Osmolite 1. 5 at 50 ml/hr x 22 hrs with 25 ml/hr automatic sterile water flush • Increase rate to 60 ml/hr on 6/22 • 6/23 Hospice care • Constipation 6/20 (small)-6/24 • Sorbitol administered 6/23 • BM 6/24

Osmolite 1. 5 at 60 ml/hr x 22 hrs with 25 ml/hr automatic sterile water flush Osmolite 1. 5: 1. 5 kcal/ml; 55. 5 g pro/L; 762 ml water/L • • 60 ml/hr x 22 hrs = 1320 ml/day = 1. 32 L/day 1. 5 kcal/ml x 1320 ml/day = 1980 kcals/day 55. 5 g pro/L x 1. 32 L/day = 73. 3 g pro/day 762 ml water/L x 1. 32 L/day = 1006 ml water/day Automatic Flushes: 25 ml/hr • 25 ml/hr x 22 hrs = 550 ml/day sterile water flushes Medications: 20 ml/medication • 20 ml/medication x 15 medications/day = 300 ml water/day Total: 1980 kcals; 73. 3 g pro; 1856 ml water Needs: Mr. P = 183. 5 lbs (83. 4 kg) 20 -25 kcal/kg = 1668 -2085 kcals/day 0. 9 -1. 1 g pro/kg = 75 -91. 74 g pro/day 20 -25 ml water/kg = 1668 -2085 ml water/day

Mr. P Timeline • June 2015 • 6/25 Jevity 1. 5 at 60 ml/hr x 22 hrs with 25 ml automatic sterile water flushes (out of stock) • Labs: • H&H- low • BG-high • BUN/Creat- high • CL- high • Loose stools switch to Jevity 1. 5 due to increased fiber

Jevity 1. 5 at 60 ml/hr x 22 hrs with 25 ml/hr automatic sterile water flush Jevity 1. 5: 1. 5 kcal/ml; 63. 9 g pro/L; 760 ml water/L • • 60 ml/hr x 22 hrs = 1320 ml/day = 1. 32 L/day 1. 5 kcal/ml x 1320 ml/day = 1980 kcals/day 63. 9 g pro/L x 1. 32 L/day = 84. 3 g pro/day 760 ml water/L x 1. 32 L/day = 1003 ml water/day Automatic Flushes: 25 ml/hr • 25 ml/hr x 22 hrs = 550 ml/day sterile water flushes Medications: 20 ml/medication • 20 ml/medication x 15 medications/day = 300 ml water/day Total: 1980 kcals; 84. 3 g pro; 1853 ml water Needs: Mr. P = 183. 5 lbs (83. 4 kg) 20 -25 kcal/kg = 1668 -2085 kcals/day 0. 9 -1. 1 g pro/kg = 75 -91. 74 g pro/day 20 -25 ml water/kg = 1668 -2085 ml water/day

Mr. P Timeline • July 2015 • Wounds resolving • Continuing oral care • 7/10: Vomiting tube feeding held • 7/15: Switched to Nepro 50 ml x 22 hrs • 7/16: Vomiting due to “car sickness” • 7/22 & 7/23: Nausea & vomiting during care tube feeding held • 7/24: Resistant to care, depressive mood, disconnecting tube feeding • 7/26 & 7/27: Vomiting continued tube feeding held • 7/28: Resident passed away

Nepro at 50 ml/hr x 22 hrs with automatic sterile water flushes 25 ml/hr and 20 ml with each medication Nepro: 1. 8 kcal/ml; 81 g pro/L; 727 ml water/L • • 50 ml/hr x 22 hrs = 1100 ml/day = 1. 1 L/day 1. 8 kcal/ml x 1100 ml/day = 1980 kcals/day 81 g pro/L x 1. 1 L/day = 89. 1 g pro/day 727 ml water/L x 1. 1 L/day = 800 ml water/day Automatic Flushes: 25 ml/hr • 25 ml/hr x 22 hrs = 550 ml/day sterile water flushes Medications: 20 ml/medication • 20 ml/medication x 15 medications/day = 300 ml water/day Total: 1980 kcals; 89. 1 g pro; 1650 ml water Needs: Mr. P = 183. 5 lbs (83. 4 kg) 20 -25 kcal/kg = 1668 -2085 kcals/day 0. 9 -1. 1 g pro/kg = 75 -91. 74 g pro/day 20 -25 ml water/kg = 1668 -2085 ml water/day

The Formulas: Formula Name Uses Nepro For dialysis patients, high in protein and fiber, steady carb release low in phosphorous, calcium and sodium Osmolite 1. 5 High in protein and calories, low fiber and low volume Jevity 1. 5 Soluble/insoluble fiber blend, contains prebiotics, standard Isotonic

Kidney Decline & End of Life Care Symptoms of end of life: • Retained secretions • Shortness of breath • Agitation • Nausea & Vomiting • Pain • Pruritus Alleviating kidney stress: • Limit sodium and reduce fluid intake edema • Limit potassium hyperkalemia • Limit phosphorous renal osteodystrophy

Why no Prostat protein supplement? • Wounds stable • Comfort care only • Formula providing adequate protein for basal needs • Resident refuses dialysis- need to limit burden on kidneys • BUN/Creat elevated- avg. ratio 32: 1 • Electrolytes elevated

Current PES Statement: Moderate Nutrition Status: Swallowing difficulty related to declined functioning s/p CVA as evidence by history of aspiration pneumonia and PEG tube placement.

Challenges: • Rapidly declining cognitive function and ADL ability • Formula tolerance and kidney stress • Diarrhea vs. Constipation • Potassium, phosphorous, and protein amounts • Edema and wound status • Hydration status and protein needs • Drug interactions • Antibiotics cause diarrhea?

Goals: • Hospice: comfort care • Provide adequate nutrition to sustain basal needs while limiting stress on the kidneys and heart: met
. Krause's food & the nutrition care process (13 th")
References • Mahan, L. (2012). Krause's food & the nutrition care process (13 th • • • ed. ). St. Louis, Mo. : Elsevier/Saunders. Stump, S. (2012). Nutrition and diagnosis-related care (7 th ed. ). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. The National Kidney Foundation. (n. d. ). Retrieved July 3, 2015. www. kidney. org The National Stroke Assocation. (n. d. ). Retrieved July 3, 2015. www. stroke. org Russon, Lynne, and Andrew Mooney. "Palliative and End-of-life Care in Advanced Renal Failure. " Clinical Medicine 10. 3 (2010): 279 -81. Print. Noble, H. , & Lewis, R. (2008). Assessing palliative care needs in endstage kidney disease. Nursing Times, 104(23), 26 -27.

QUESTIONS? Thank you!!
- Slides: 40