The Cardiovascular system Done by Dr Abdullah Ahmad

The Cardiovascular system Done by Dr Abdullah Ahmad Obeid internal medicine specialist
 results from acute or subacute")
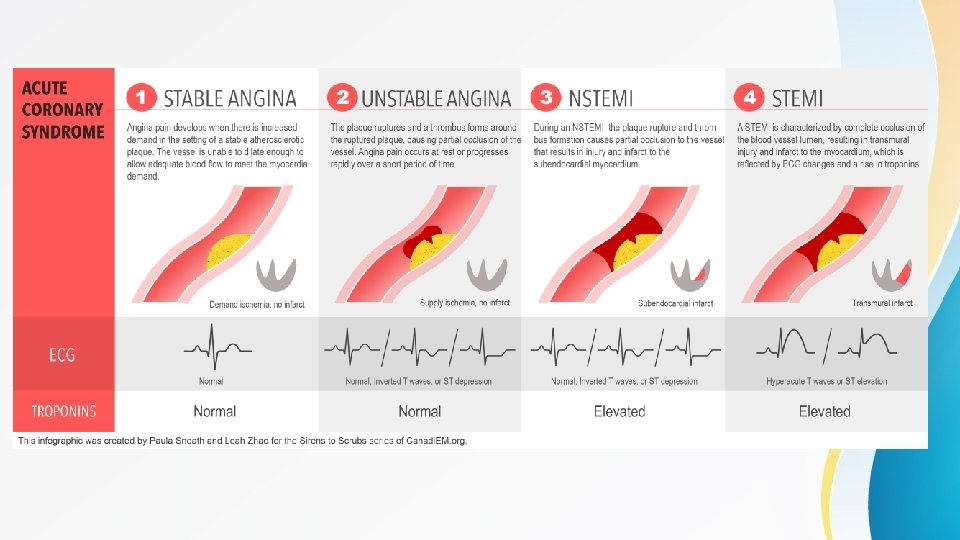
Acute Coronary syndromes • An acute coronary syndrome (ACS) results from acute or subacute disruption in coronary blood flow. • ACS is caused by acute plaque rupture or erosion , often in sections of the coronary artery with mild or moderate stenosis. • ACS is classified as ST elevation myocardial infarction (STEMI) or non-ST elevation acute coronary syndrome(NSTE ACS) (which involves Non-ST elevation myocardial infarction and Unstable angina) based on findings on ECG.

Acute Coronary syndromes
 • The hallmark ECG features of 1 are ST-segment")
ST elevation myocardial infarction (STEMI) • The hallmark ECG features of 1 are ST-segment elevation of 1 mm or more in two or more contiguous limb or chest leads. • An ST-elevation myocardial infarction occurs from occlusion of one or more of the coronary arteries that supply the heart with blood. The cause of this abrupt disruption of blood flow is usually plaque rupture, erosion, fissuring or dissection of coronary arteries that results in an obstructing thrombus. The major risk factors for ST-elevation myocardial infarction are dyslipidemia, diabetes mellitus, hypertension, smoking, and family history of coronary artery disease. • Coronary athersclerosis and presence of high risk thin cap fibroatheroma (TCFA) can result in sudden onset plaque rupture. This results in changes in vascular endothelium resulting in cascade of platelet adhesion , activation and aggregartion, resulting in thrombosis formation.
 • NSTE ACS is further categorized according to")
Non-ST elevation acute coronary syndrome(NSTE ACS) • NSTE ACS is further categorized according to the presence of biomarkers of cardiac injury (troponin T or 1) in the serum. • NSTEMI is defined as a biomarker positive presentation that does not meet the criteria for STEMI • Unstable angina is characterized by new or worsening angina, with or without ECG changes, and without detectable levels of cardiac injury markers. • Any new onset angina is unstable angina • Angina at rst or with minimal exertion is unstable angina • Crescendo(worsening) angina - in severity , duration and/or frequency is considered unstable angina • Any angina following an MI (first 2 weeks) is considered unstable angina

Presentation • Presentation of STEMI is often dramatic and clear , usually with severe retrosternal chest pain almost semilar to anginal pain radiating to left shoulder , left arm , neck , jaw or interscapular area associated with sweating , nausea and/or vomiting. • Epigastric pain is common especially with inferior MI • 10 -15% of patients have silent MI especially elderly and diabetics • Several diagnoses can mimic STEMI. These disease entities need to be distinguished from STEMI to minimize patient harm. • S 3 indicate acute LV failure / Murmurs can be heard due to complications like VSD or Vavular regurgitation due to papillary muscle rupture • Acute pericarditis presents with acute chest pain and ST segment elevation. The ST segment elevation of pericarditis tends to be diffuse and concave; and friction rub can be heard on auscultation however, ECG can be easily misinterpreted for STEMI on ECG

Contd • Myopericarditis resulting from viral infections or autoimmune conditions can cause cardiac enzyme release, further confusing the clinical picture • Left ventricular hypertrophy-induced ECG changes may also look similar to ST-segment elevation injury , however, these changes are typically concave in appearance. Comparison with previous ECG results is helpful in assessing for acute changes. • Lt ventricular aneurism can also cause persistent ST elevation on ECG , history of previous MI should raise the suspicion for this diagnosis • Aortic dissection cause ST-segment clevation if the dissection involves the left or right coronary artery. • Aortic dissection is a surgical emergency and must be recognized early because treatments are very different from those of MI - Diagnostic clues include blood pressure difference between Rt and Lt arms and mediastinal widening on CXR • Severe hypercalcemia and severe hyperkalemia also can cause ST elevation

Pericarditis

Left ventricular hypertrophy

Left ventricular aneurism

Evaluation • Initial evaluation should include a focused physical examination and a brief history. • Patients should be asked about the characteristics of the pain and associated symptoms, risk factors or history of cardiovascular disease, and recent drug use. • Risk factors for an ST-elevation myocardial infarction include age, gender, family history of premature coronary artery disease, tobacco use, dyslipidemia, diabetes mellitus, hypertension, abdominal obesity, sedentary lifestyle, a diet low in fruits and vegetables, psychosocial stressors. • Cocaine use can cause an ST-elevation myocardial infarction regardless of risk factors. • In Cocaine induced MI , it is contraindicated to use B-blockers • Evaluation of patients with acute onset of chest pain should begin with an electrocardiogram (ECG) and troponin level.
 : - New ST-segment elevation")
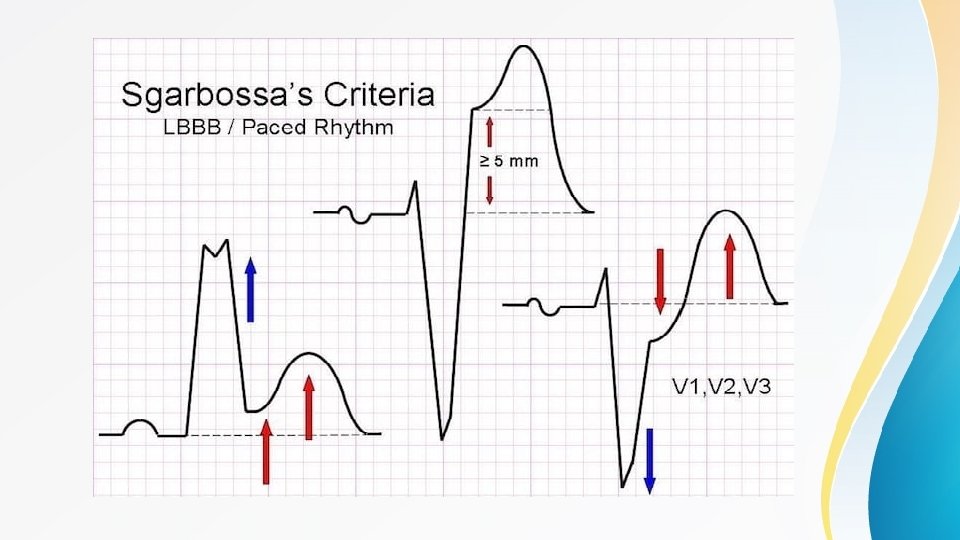
Contd • ECG criteria for ST-elevation myocardial infarction (STEMI) : - New ST-segment elevation at the J point in 2 contiguous leads with the cutoff point as greater than 0. 1 m. V in all leads other than V 2 or V 3 - In leads V 2 -V 3 the cutoff point is greater than 0. 2 m. V in men older than 40 years old and greater than 0. 25 in men younger than 40 years old, or greater than 0. 15 m. V in women - A new LBBB is commonly used for STEMI diagnosis • Patients with a pre-existing left bundle branch block can be further evaluated using Sgarbossa's criteria - ST-segment elevation of 1 mm or more that is concordant with (in the same direction as) the QRS complex - ST-segment depression of 1 mm or more in lead V 1, V 2, or V 3 - ST-segment elevation of 5 mm or more that is discordant with (in the opposite direction) the QRS complex

J point

STEMI

Contd • Findings suggestive of NSTEMI include transient ST elevation, ST depression, or new T wave inversions. ECG should be repeated at predetermined intervals or if symptoms return. • Q wave formation can be seen in ACS and usually indicate myocardial necrosis , can be a late feature or happen early after the acute insult • A normal ECG does not exclude ACS • Cardiac troponin is the cardiac biomarker of choice. • CK-MB is helpful to detect reinfarction as it has a short duration of detection • Most patients with true ischemia will have elevations in troponin within 6 hours, and negative troponins at this point effectively rule out infarct in most patients. • Troponin can be elevated in other cases rather than MI including : sepsis , renal failure , PE , heart failure , post PCI. . . etc , so the whole picture is important rather than taking every peice of the puzzle alone.
")
NSTEMI ( ST depression )
")
NSTEMI ( T wave inversion )

Q wave

Cardiac biomarkers

Cardiac biomarkers

Contd • Several tools and scores have been developed to assist in the workup of Non -elevation ACS • Two common tools available are the TIMI (Thrombolysis In Myocardial Infarction) risk score, the GRACE (Global Registry of Acute Coronary Events) risk score • NSTEMI is diagnosed in patients determined to have symptoms consistent with ACS and troponin elevation but without ECG changes consistent with STEMI. Unstable angina and NSTEMI differ primarily in the presence or absence of detectable troponin leak.
 risk score *Scores ranging from 0 -2 constitute a")
TIMI (Thrombolysis In Myocardial Infarction) risk score *Scores ranging from 0 -2 constitute a low risk. Scores from 3 -5 are considered intermediate risk. A score of 6 or 7 indicates high risk.

Localization of the MI on ECG

Management • Upon STEMI recognition, reperfusion with thrombolytic agents or primary percutaneous coronary intervention (PPCI) is necessary. PPCI is the preferred method of reperfusion in most cases. • PPCI is the emergent coronary angiography and PCI in patients with STEMI. • The amount of myocardial salvage is directly related to ischemic time therefore, the quicker the artery can be opened, the better the final outcome. • PPCI is recommended for STEMI patients when it can be done within 2 hors of first medical contact Thrombolytic therapy is recommended for patients with STEMI when symptom onset is within 12 hours and PPCI is not available within 120 minutes of first medical contact. • In addition all patients , without contraindications , should have a loading dose aspirin(162 -325) , intavenous heparin (enoxaparin or foundaparinox can be used) , clopidogrel (300 -600)mg , morphine or nitroglycerine for pain relief and oxygen in patients with O 2 saturation less than 94%

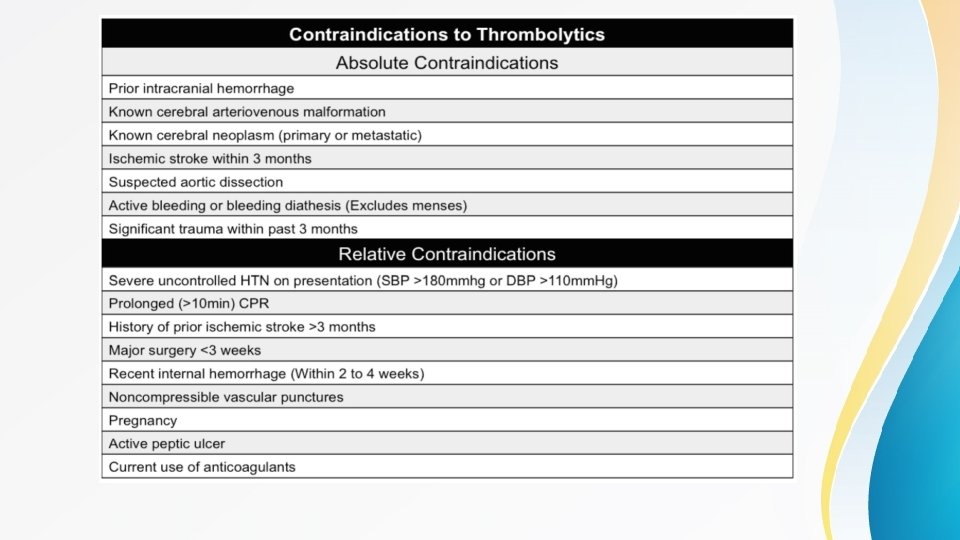
Contd • Nitroglycerin is contraindicated in patients with hypotension , Rt ventricular MI and in patients who have used PDE inhibitors(e. g : sildenifil) in the past 72 hours before presentation • After thrombolytic therapy is administered. the ECG should be repeated at 60 minutes and 90 minutes to confirm at least 50% improvement in maximal ST segment elevation. • In Non-ST elevation ACS there is no role for thrombolytics • Owing to the potential for thrombolytic failure, patients with STEMI treated with thrombolytic therapy should be subsequently transferred to a PCl capable hospital. Rescue PCI is associated with improved outcomes compared with conservative management in the event of failed reperfusion. • Intracerebral hemorrhage is the most catastrophic complication of thrombolytic therapy and occurs in approximately 1% of patients. • Coronary angiography is generally recommended in all patients before discharge, even after successful thrombolysis.

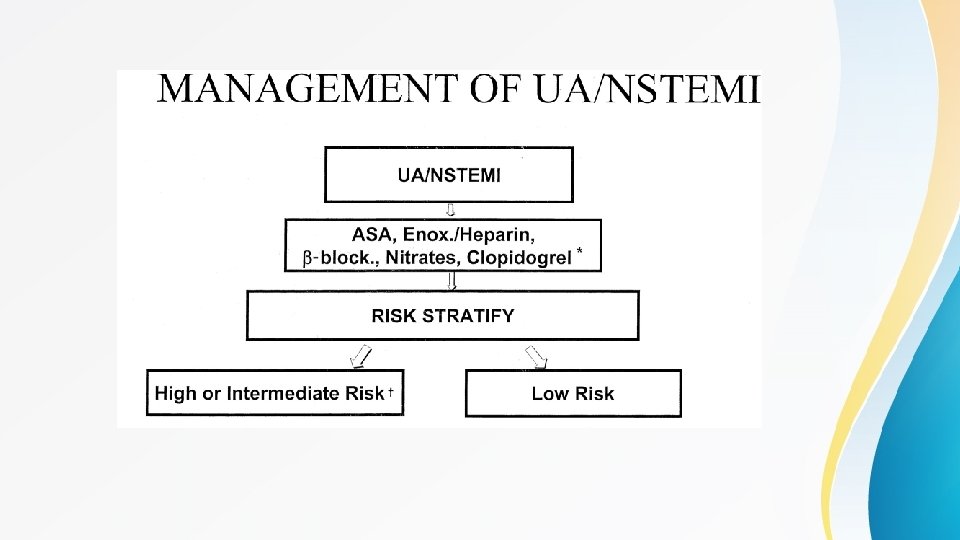
Contd • Patients with Non-ST elevation ACS undergo risk assessment according to previously mentioned scores (e. g : TIMI score) and managed accordingly • If the patient has high or intermediate risk for major cardiovascular events then he should be referred for PCI and treated as STEMI ( with the exception that he should not be treated with thrombolytics) • If the patient has low risk for major cardiovascular events then he should be treated consevatively and referred for elective cardiac catheterization and PCI • All ACS patients should be discharged on aspirin (lifelong) , clopidogrel (for at least one year) , B-blocker , statin , ACEI or ARB , unless there are contranindications , as these drugs are known to improve mortality in patients with ACS

Complications of MI • Arrhythmias : -ventricuar fibrillation is the most common cause of death after MI -sinus tachycardia although benign in itself but can increase oxygen demand -ventricular tachycardia / ventricular ectopy (PVC) -atrial fibrillation -bradyarrhythmia can be due MI involving the area of the AV node • Mechanical complications include -heart failure / cardiogenic shock -myocardial rupture / VSD -Ventricular aneurisms / Lt ventricular apical thrombus -papillary muscle rupture causing valvular regurgitation -Early (1 -3 days after MI) or Late pericarditis (usually after 2 weeks and called dressler syndrome)

Poor prognostic factors after MI • Advanced age • Diabetes mellitus • Previous vascular disease (eg, cerebrovascular disease or peripheral vascular disease) • Elevated thrombolysis in MI (TIMI) risk score • Delayed or unsuccessful reperfusion • Poorly preserved left ventricular function (the strongest predictor of outcome) • Evidence of congestive heart failure • Elevated B-type natriuretic peptide (BNP) levels • Elevated high sensitive C-reactive protein (hs-CRP) • Involvement of electrocardiograph (ECG) lead a. VR • Depression • Being a female

Thank you
- Slides: 33