The Bones and Soft Tissue Bones Consist of

The Bones and Soft Tissue
 • Made of: – 35% organic")
Bones • Consist of osteocytes (mature bone cells) • Made of: – 35% organic material – 65% inorganic mineral salts, and water 2
 • Formation: – Initially consists of collagenous protein fibers secreted by")
Bones (cont’d. ) • Formation: – Initially consists of collagenous protein fibers secreted by osteoblasts – During embryonic development, cartilage is deposited between fibers – During the eighth week of embryonic development, ossification begins • Mineral matter starts to replace previously formed cartilage, creating bone 3

Injury to Bones • Fractures – Simple or closed – Compound or open – Comminuted – Stress – Epiphyseal plate 4
 • Fracture signs and symptoms – Swelling, deformity, pain,")
Injury to Bones (cont’d. ) • Fracture signs and symptoms – Swelling, deformity, pain, tenderness, and discoloration • Treatment – Bones must sometimes be put back in proper position (i. e. , reduction) – Immobilization through use of a cast – Surgery 5

Muscles • Principal types of muscles: – Skeletal • Under voluntary control – Smooth • Involuntary – Cardiac • Only found in the heart • Involuntary 6

Characteristics of Muscles • Four common characteristics: – Contractibility – Excitability – Extensibility – Elasticity 7

Muscle Attachments and Functions • More than 600 muscles in the body • Muscles attached to bones by tendons – Bones are connected at joints • Muscles are attached at both ends to bones, cartilage, ligaments, tendons, skin, or other muscles 8
 • Origin: part of a skeletal muscle that")
Muscle Attachments and Functions (cont’d. ) • Origin: part of a skeletal muscle that is attached to a fixed structure or bone • Insertion: attached to a movable part • Belly: central body of the muscle • Prime mover: movement in a single direction – Antagonist: movement in the opposite direction 9

Sources of Energy and Heat • When muscles work, they move the body and produce heat • For muscles to contract and work, they need energy – Major source of energy is adenosine triphosphate • Cell requires oxygen, glucose, and other materials – When a muscle is stimulated, ATP is broken down, producing energy 10

Contraction of Skeletal Muscle • Muscle movement occurs as a result of: – Myoneural stimulation – Contraction of muscle proteins • Skeletal muscles must be stimulated by nerve impulses to contract – Begins with action potential, which travels along muscle fiber length – Basic source of energy is glucose 11

Muscle Fatigue • Caused by accumulation of lactic acid in muscles • During vigorous exercise, blood is unable to transport enough oxygen for complete oxidation of glucose in the muscles – Causes muscles to contract anaerobically (without oxygen) 12

Muscle Tone • Muscles should always be slightly contracted and ready to pull (muscle tone) • Muscle atrophy: – Wasting or loss of muscle tissue resulting from disease or lack of use • Hypertrophy: – Increase in the mass (size) of a muscle 13

Injuries to Muscles • Strain: – Caused by twisting or pulling a muscle or tendon – Acute or chronic • Symptoms: pain, muscle spasm, and muscle weakness • Treatment: reduce swelling, anti-inflammatory drugs, surgery, rehabilitation 14
 • Sprain: – Caused by sudden twist, or a")
Injuries to Muscles (cont’d. ) • Sprain: – Caused by sudden twist, or a blow to the body • Symptoms: pain, swelling, bruising, and loss of ability to move • Treatment is similar to care for a strain • Tendonitis: – Inflammation of the tendon • Symptoms: pain and inflammation along a tendon • Treatment: avoid aggravating movements, medications, rehabilitation 15
 • Bursitis – Inflammation of a bursa • Symptoms:")
Injuries to Muscles (cont’d. ) • Bursitis – Inflammation of a bursa • Symptoms: joint pain often mistaken for arthritis • Treatment: avoid aggravating movements, medications, rehabilitation 16
 • Contusion: – Direct blow that does not break")
Injuries to Muscles (cont’d. ) • Contusion: – Direct blow that does not break the skin • Symptoms: swelling, pain to the touch, redness, and ecchymosis • Treatment: monitoring, ice, medications, compressive dressing 17

Nerves • Nerve tissue consists of: – Neuroglia • Insulate, support, and protect neurons – Neurons • Sensory • Motor • Associative 18
 • Nerves carry impulses by creating electric charges through membrane excitability")
Nerves (cont’d. ) • Nerves carry impulses by creating electric charges through membrane excitability – A synapse is the space between adjacent neurons through the impulse is transmitted 19

Injury to Nerves • Nerves are fragile and can be damaged by pressure, stretching, or cutting – Injury to a nerve can stop signals to and from the brain • Causes muscles to become unresponsive and a loss of feeling in the injured area 20

Soft-Tissue Injuries • Classified as: – Open • Abrasions, lacerations, avulsions, and puncture wounds – Closed • Contusions, hematomas, ecchymoses, sprains, strains, tendonitis, bursitis, and stress-related injuries 21

The Body’s Response to Injury • Inflammation: – Reaction to invasion by an infectious agent or physical, chemical, or traumatic damage • Regeneration: – Act of wound healing • Cellular dedifferentiation: – Regeneration – Cells revert to an earlier stage of development 22
 • Transdifferentiation – Regeneration of cells with")
The Body’s Response to Injury (cont’d. ) • Transdifferentiation – Regeneration of cells with completely different functions than original • Tissue remodeling – Cells and molecules of tissue are modified and reassembled to yield a new composition of cell types and extracellular matrix 23

Conclusion • The skeleton – Provides support and protection to internal organs – Foundation for muscle attachment – Efficient factory for producing red blood cells • Many injuries associated with athletics are fractures – Other injuries involve muscles, attachments, and various surrounding tissues 24

Tissue Response to Injury

Inflammatory Response • Acute Inflammation – Short onset and duration – Change in hemodynamics, production of exudate, granular leukocytes • Chronic Inflammation – Long onset and duration – Presence of non-granular leukocytes and extensive scar tissue
 Tumor (swelling) Color (heat) Dolor")
Cardinal Signs of Inflammation • • • Rubor (redness) Tumor (swelling) Color (heat) Dolor (pain) Functio laesa (loss of function)
 • 1. Inflammatory response phase •")
Phases of the Inflammatory Response (3 separate phases) • 1. Inflammatory response phase • 2. Fibroblastic repair phase • 3. Maturation and remodeling phase

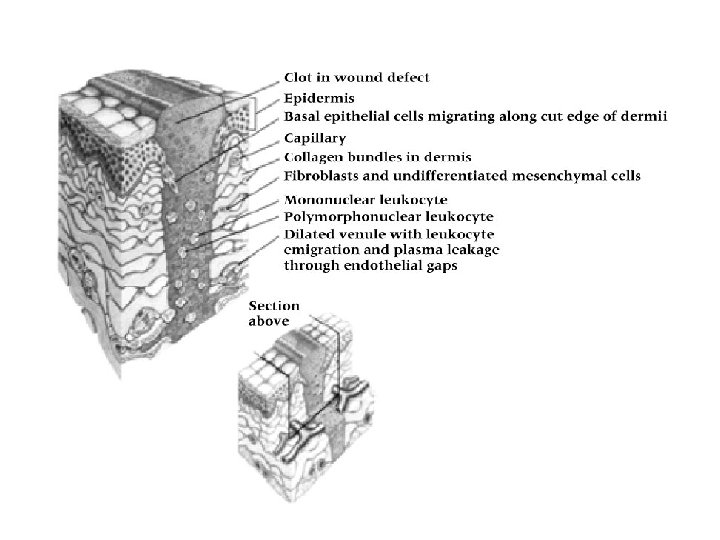
Phase I • Healing begins immediately • Injury results in altered metabolism and liberation of various materials • Initial reaction by leukocytes and phagocytic cells – Goal • • Protect Localize Decrease injurious agents Prepare for healing and repair
- local anemia and coagulation occur to seal")
• First hour – Vasoconstriction(15 min)- local anemia and coagulation occur to seal blood vessels and chemical mediators are released – Immediately followed by vasodilation(hyperemia: doesn’t last long) or blood vessel • Second hour – Vasodilation decreases – Blood flow slows – increased blood viscosity(thickness) resulting in edema (swelling that last 24 to ) – Chemical Mediators released

nd 2 Hr. Chemical mediators • Released to alter membrane permeability, dilatory responses, margination, and phagocytic activity • Histamine- vasodilation and permeability • Leukotrienes- margination • Cytokines- regulate Leukocyte traffic and attract phagocytes
 ØExudate increases: high concentration of RBC’s and protein rich")
• Second hour (continued) ØExudate increases: high concentration of RBC’s and protein rich fluid due to increased vessel permeability. (amount depends on damage) ØPermeability changes generally occur in capillary and venules ØMargination occurs causing leukocytes to fill the area and line endothelial walls ØThrough diapedesis(passage of blood cells) and chemotaxis(cell movement) leukocytes move to injured area

• Clot Formation – Platelets adhere to exposed collagen leading to formation of plug (clot) – Clots obstruct lymphatic fluid drainage and aid in localizing injury – Requires conversion of fibrinogen to fibrin • Initial stage: thromboplastin is formed • Second stage: Prothrombin is converted to thrombin due to interaction with thromboplastin • Third stage: thrombin changes from soluble fibrinogen to insoluble fibrin coagulating into a network localizing the injury

• Chronic Inflammation ØOccurs when acute inflammatory response does not eliminate injuring agent ØTissue not restored to normal physiologic state ØInvolves replacement of leukocytes with macrophages, lymphocytes and plasma cells ØCause for shift from acute to chronic is unknown ØTypically associated with overuse, overload, cumulative microtrauma

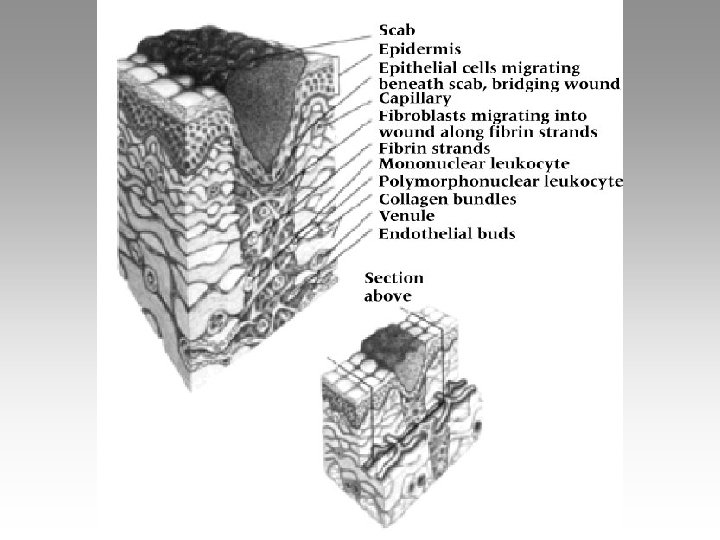
Phase II: Fibroblastic Repair Phase • Scar formation through 3 phases – Resolution (little tissue damage and normal restoration) – Restoration (if resolution is delayed) – Regeneration (replacement of tissue by same tissue) • Referred to as fibroplasia – Complaints of pain and tenderness which gradually subside during this period
")
• Scar formation – Formation of delicate connective tissue – With proliferation(rapid increases) of collagen(main structural protein) scar tensile strength(resistance of material breaking down under tension) increases • # of fibroblasts(cells producing collagen) gradually diminishes – Normal sequence = minimal scarring – Persistent inflammation = extended fibroplasia

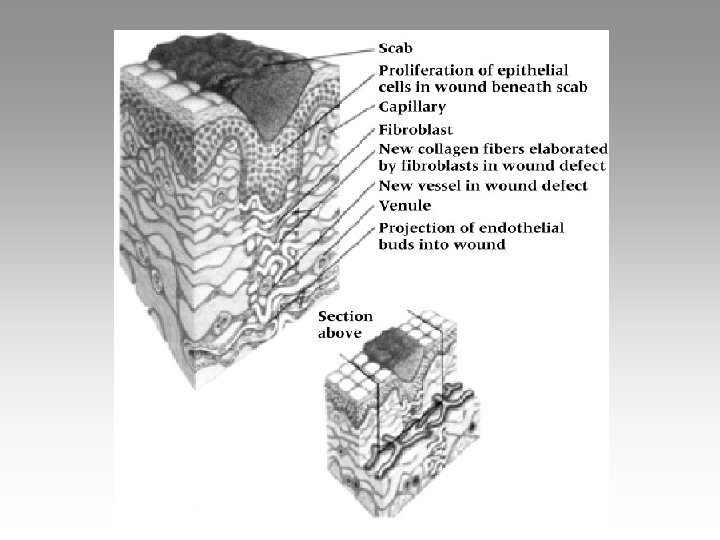
Phase III: Maturation & Remodeling • Long-term process • Realignment of collagen relative to applied tensile forces meaning the begin to look like normal tissues again • Continued breakdown and synthesis of collagen = increased strength • Tissue will gradually assume normal appearance • May require several years to complete

Role of Progressive Mobilization üInitially must maintain some immobilization in order to allow for initial healing üAs healing moves into repair phase controlled activity should be added Ø Work towards regaining normal flexibility and strength Ø Protective bracing should also be incorporated üDuring remodeling aggressive ROM and strength exercises should be incorporated Ø Facilitates remodeling and realignment üMust be aware of pain and other clinical signs – may be too much too soon

Factors That Impede Healing • • Extent of injury Edema Hemorrhage Poor Vascular Supply • Separation of Tissue • Muscle Spasm • Atrophy • Corticosteroids • Keloids and Hypertrophic Scars • Infection • Humidity, Climate, Oxygen Tension • Health, Age, and Nutrition

Cartilage Healing • Limited capacity to heal • Little or no direct blood supply • Failure to elicit clot formation and cellular response

Ligament Healing • Repair phase will involve random laying down of collagen which, as scar forms, will mature and realign in reaction to joint stresses and strain • Full healing may require 12 months

Skeletal Muscle Healing • Initial bleeding followed by proliferation of ground substance and fibroblast • Collagen will mature and orient along lines of tension • Healing could last 6 -8 weeks depending on muscle injured

Tendon Healing • Big problem • Abundance of collagen is required for good tensile strength – Too much = fibrosis – may interfere with gliding • Initially injured tendon will adhere to surrounding tissues (week 2) • Week 3 – tendon will gradually separate • Tissue not strong enough until weeks 4 -5

Management Concepts • Drug utilization – Anitprostaglandin agents used to combat inflammation – Non-steroidal antiinflammatory agents (NSAID’s) – Medications will work to decrease vasodilatation and capillary permeability

Management Concepts • Therapeutic Modalities – Thermal agents are utilized • Heat stimulates acute inflammation (but works as a depressant in chronic conditions) • Cold is utilized as an inhibitor – Electrical modalities • Treatment of inflammation • Ultrasound, microwave, electrical stimulation (includes transcutaneous electrical muscle stimulation and electrical muscle stimulation)

Therapeutic Exercise – Major aim involves pain free movement, full strength, power, and full extensibility of associated muscles – Immobilization, while sometimes necessary, can have a negative impact on an injury • Adverse biochemical changes can occur in collagen – Early mobilization (that is controlled) may enhance healing

Bone Healing • Less complex process • Acute fx have 5 stages ØHematoma formation ØCellular proliferation ØCallus formation ØOssification ØRemodeling

Bone Healing • Trauma to the periosteum and surrounding soft tissue occurs due to the initial bone trauma • During the first 48 hours a hematoma within the medullary cavity and the surrounding tissue develops • Ossification is complete when bone has been laid down and the excess callus has been resorbed by osteoclasts • Bone continually adapts to applied stresses(Wolff’s Law) – Balance between osteoblast and osteoclast activity • Time required is dependent on various factors – Severity and site of fracture – Age and extent of trauma • Time will range from 3 -12 weeks

Pain • Major indicator of injury • Pain is individual and subjective • Factors involved in pain – Anatomical structures – Physiological reactions – Psychological, social, cultural and cognitive factors

Pain sources – Cutaneous pain: is sharp, bright and burning with fast and slow onset – Deep somatic pain: originates in tendons, muscles, joints, periosteum and blood vessels – Visceral pain: begins in organs and is diffused at first and may become localized – Psychogenic pain: is felt by the individual but is emotional rather than physical

Types of Pain Fast versus Slow Pain – Fast pain localized – Slow pain is perceived as aching, throbbing, or burning Referred Pain – Pain which occurs away from actual site of injury/irritation – Unique to each individual and case – May elicit motor and/or sensory response

Psychological Aspects of Pain Ø Pain can be subjective and psychological Ø Pain thresholds vary per individual Ø Pain is often worse at night due to solitude and absence of external distractions Ø Personality differences can also have an impact Ø A number of theories relative to pain exist § Physiological and psychological components Ø Athlete, through conditioning are often able to endure pain and block sensations of minor injuries

Modalities in Rehab

most commonly used • • • cryotherapy thermotherapy electrical stimulation iontophoresis traction ultrasound

Modalities in Rehab • modalities are adjuncts to treatments not sole treatments. • most have limited evidence to support its use. – lots of anecdotal evidence

Cryotherapy • Indications – Acute or chronic pain, or muscle spasm – Acute inflammation – Post surgical pain or edema – Facilitate mobilization

Cryotherapy • Heat Abstraction • Depth of 5 cm can be cooled • Change in Temperature depends on: – Type of Agent – Temp. difference between agent and tissue – Amount of insulation • Thermal Conductivity • Limb circumference • Duration of application

Cryotherapy • • Leads to vasoconstriction Decreases tissue metabolism Decreases tissue permeability Decreases capillary permeability Decreases pain Decreases spasms Analgesic relief of pain
")
Types of Cryotherapy Applications • • Ice Massage Ice Packs Cryocuffs Ice Immersion (Whirlpool) Commercial Gel and Chemical Packs Controlled Cold-Compression Units Vapocoolant sprays

Thermotherapy • • • Increases circulation Increases cellular metabolism Produces analgesic or sedative effect Helps resolve pain and muscle spasm Vasodilatation: – Promotes Healing – Increases Oxygen concentration – Removes debris and waste products

Thermotherapy • Types of Applications – – – Moist heat packs Ultrasound Paraffin baths- hands (OT) Diathermy heat –not used clinically anymore Whirlpools - training rooms Hot tubs – training rooms

Electro Therapy

TENS Conventional Low Rate

Conventional / High Rate TENS Indications: • Any painful condition – Chronic typically • If Muscle contraction: – increases pain – contraindicated • Post-op management of pain Contraindications: • Known myocardial problems, pacemakers • Stimulation over anterior neck • Thrombophlebitis • Superficial skin lesions

Conventional / High Rate TENS Pulse duration: 50 -80μs Pulse freq: 100 -150 pps Intensity: low-submotor, tingling Treatment time: 30 min. to 24 hrs.

Low Rate TENS • Mechanism of action equated with acupuncture • More vigorous than high-rate • Used to treat sub-acute, chronic pain and trigger points • Pain modulation • Beta-endorphins- _____ suppressor

Low Rate TENS • Indications: – pain, now tolerates muscle contraction – trigger points – muscle guarding • Contraindications: – same as for conventional TENS

Low Rate TENS Pulse duration: 100 -200 microsec. Pulse freq: low: 2 -4 pps Intensity: strong, non-painful, visible muscle contraction Treatment time: 30 min.

Therapeutic Electrically Induced Muscle Contraction • Therapeutic gains: – muscle reeducation – muscle pump contractions – muscle strengthening

Muscle Reeducation • Primary indication: inhibition after injury or surgery • Theory for inhibition related to sensorimotor dysfunction • ES induces involuntary muscle contraction which increases sensory input from that muscle
. – More rapid recovery and")
Muscle Strengthening • Effectiveness with ES for weakness (post-surg). – More rapid recovery and greater gains than exercise alone • Mechanism: – Specificity: preferential recruitment of type II muscle fibers – Overload principle: • e-stim with ex – NO improved strength than either one alone • Significant strength gains in healthy individuals using ES

Russian Current

Russian Current • 1977 Yakov Kots • report during Canadian-Soviet exchange symposium on electrostimulation of skeletal muscle • 3 revolutionary claims – generates 30% more force than max vol contraction – painless current – lasting gains up to 40% strength increase in normals • Commercial reaction – production of “Russian” current stimulators

Indications for “Russian” current • Post knee lig surgery • Post arthroscopic knee surgery • ACL sprain (increase quad force during immobilization) • “PRIME” indication: strengthen the muscular apparatus of HEALTHY population
 •")
Muscle Pump Contractions Edema Reduction • ES to induce muscle contractions (pumping action) • Duplicates normal muscle pumping contractions • Stimulates circulation thru venous and lymphatic channels • Sensory level stimulation may be used for edema control – increase ionic movement – reported to decrease edema in vitro – effectiveness not found in humans in vivo

Interferential Current C 1 C 3 C 2

Interferential Biophysical Characteristics Methods of delivery quadripolar: 4 electrodes, each pair to separate channel Interference at level of TREATMENT AREA “ 4 leaf clover” shaped field
 quadripolar Target sweep: enlarge field Vector scan")
Interferential Biophysical Characteristics Methods of delivery (cont) quadripolar Target sweep: enlarge field Vector scan

Electrical Stimulation for Denervated Muscle

ES for Denervated Muscle • Utilized in PT for decades • Purpose: minimize atrophy during regeneration • Parameters depend on generator: – Can be DC or AC

ES for Denervated Muscle • Controversy over efficacy produced several in vitro studies in mid 80’s • Does Not effect improvement in rate of regeneration
 • Estim may retard motor")
ES for Denervated Muscle More controversy: (in vitro studies) • Estim may retard motor nerve sprouting and reinnervation (Schimrigk 1977) Bottom line • Delay of functional return from interference with reinnervation – ES induced contraction disrupts regenerating NMJ NOT – this retards reinnervation Recommended • Trauma to regenerating cell body ? ? • Definitely more research needed!

Iontophoresis

Introduction • Transcutaneous drug delivery has been used for centuries – herbal plasters, medicated baths, etc. • Iontophoresis -- the use of an electrical current for the transcutaneous delivery of ions into the body

Introduction • Fairly widespread use of iontophoresis past 20 -30 years • Very commonly used now in PT clinics • Iontophoresis offers a safe and painless way of “injecting” drugs through the skin into underlying target tissues • Alternative to oral or injection methods of drug delivery

Basic Principles of Application • Electrostatic repulsion of like charges is the driving force for iontophoresis • Knowledge of a drug’s or ion’s polarity is critical – dictates the polarity of the electrode needed to drive the drug to underlying Rx area

Ionto. Patch™ • “Patch” is both a current generator and electrodes • Applied in the clinic and the patient wears the patch home • Delivers a very low amplitude of current (0. 1 m. A) that is worn for 12 -24 hours • Manufacturer states that the low intensity current reduces the risk of skin irritation and burns
 Calcium")
Common Medications Used in Iontophoresis Ion Source Polarity Indications % Acetic acid (-) Calcium deposits 2. 5 -5. 0 Dex. Na 2 PO 3 (-) Inflammation 0. 4 Lidocaine (+) Pain 5 Acetate Dexamethasone Salicylate Na. Sal (-) Inflammation 2 Water -- (+/-) Hyperhydrosis NA Zinc Zn. O 2 (+) Wounds NA

Does it Work ? ? • Experimental evidence does exist to show that iontophoresis does enhance the transcutaneous delivery of ions into tissues • Limited depth of penetration (1 cm 1/2 in) • Lack of high-quality clinical evidence to support its use, but • Sufficient evidence from case studies and commentaries that suggest clinicians should consider iontophoresis for the treatment of superficial inflammatory conditions

Traction • Contraindications • Indications – – – Herniated disc Spinal nerve impingement Spinal nerve inflammation Joint hypo-mobility Narrowing of intervertebral foramen – Degenerative joint disease – Joint pain – Unstable vertebrae – Gross emphysema – Temperomandibular joint dysfunction – Patient discomfort

Ultrasound
 – Surgical (high intensity) – Therapeutic")
Introduction • Ultrasound uses: – Diagnostic (low intensity) – Surgical (high intensity) – Therapeutic • Therapeutic US widely used for deep heat
")
Introduction • Primary clinical use: – Soft tissue repair – Pain relief (analgesia)
 • Total area on surface of transducer producing soundwave •")
Effective Radiating Area (ERA) • Total area on surface of transducer producing soundwave • Ideally ERA should match size of transducer • Treatment area should not exceed 2 -3 times ERA

Frequency of Ultrasound • Determined by number of times crystal deformed/sec. • 2 most common utilized in U. S. – 1. 0 MHz – 3. 0 MHz • Determines depth of penetration, unlike ES

Frequency of Ultrasound • Inverse relationship between frequency and depth of penetration • Penetrating depths: – 1. 0 MHz: 2 -5 cm – 3. 0 MHz: 1 -2 cm • Absorption rate increases with higher frequency

Pulsed vs Continuous • Most new generators produce both • Both produce thermal & nonthermal effects

Pulsed vs Continuous • Continuous: – Sound intensity remains the same – Commonly used for thermal effects

Pulsed vs Continuous • Pulsed: – Intensity periodically interrupted – Average intensity reduced over time

Physiological Effects of Ultrasound • Thermal effects • Non-thermal effects – Cavitation – Acoustic microstreaming

Thermal Effects • Clinical effects: – Increased extensibility of collagen fibers • tendons • joint capsule – Decreased joint stiffness

Thermal Effects • Clinical effects: – Reduction in muscle spasm – Pain modulation – Increased blood flow – Increased nerve conduction

Thermal Effects • Primary advantage of US – Selective heating of tissues high in collagen – Non-thermal effects are occurring
 Effects • Primary physiological effects are cavitation and acoustic microstreaming • Cavitation:")
Non-thermal (Mechanical) Effects • Primary physiological effects are cavitation and acoustic microstreaming • Cavitation: – Formation of gas-filled bubbles in tissue fluids – Expansion/compression of bubbles either stable or unstable
 Effects • Acoustic microstreaming: – Unidirectional movement of fluids along cell membrane")
Non-thermal (Mechanical) Effects • Acoustic microstreaming: – Unidirectional movement of fluids along cell membrane boundaries – Produces high viscous stresses – Alters membrane structure & function – Increased permeability to ionic influx
 Effects • Potential therapeutic effects from cavitation & microstreaming – Stim. of")
Non-thermal (Mechanical) Effects • Potential therapeutic effects from cavitation & microstreaming – Stim. of fibroblast activity synthesis & tissue repair increases protein – Increased blood flow – bone healing & repair of non-union fractures

• Indications – – – Ultrasound • Contraindications Increase deep tissue heat Decrease inflammation Decrease muscle spasms Decrease pain Increase extensibility of collagen tissue – Decrease pain of neuromas – Decrease joint adhesions – Treat myositis ossificans – – – Hemorrhage Infection Thrombophlebitis Suspected malignancy Impaired circulation or sensation – Stress fracture sites – Epiphyseal growth plates – Over the Eyes, Heart, Spine, or genitals

Phonophoresis • Ultrasound with drugs, used to increase absorption and penetration of drugs • Anti-inflammatory’s – Cortisol – Dexamethasone – Salicylates • Analgesics – Lidocaine

Phonophoresis • in theory phonophoresis increases the permeability of the stratum corneum allowing better penetration of drug

Summary • modalities are best utilized as adjuncts not primary treatment • limited evidence – plenty of anecdotal proof – variable parameters • most utilized are ionto, traction heat/cold, and estim
- Slides: 113