The Bleeding Patient Brian C Boulmay MD Section

The Bleeding Patient Brian C Boulmay, MD Section of Hem. Onc

Case 1 • Forty seven year old healthy woman has a lap chole converted to an open procedure due to oozing of blood from small ligated arteries; several need to be re-tied. • Post-operatively, she is noted to have oozing of blood around the surgical site. There is ecchymosis around the wound that worsens over 2 days. • A hematology consult is requested.

Case 2 • 64 year old man Korean War veteran has a TURBT for a T 1 bladder tumor. The patient is readmitted two days after the procedure with hematuria. • Repeat cystoscopy shows small amount of bleeding at the resection site. • Foley catheter remians in place. The patient continues to have hematuria, requiring PRBCs every 3 days. Urology confident there are no arterial bleeders. • A hematology consultation is requested after a three week hospitalization.

Case 2 b • 48 year old man is readmitted with his 3 rd subdural hematoma in 8 weeks. • PMH: ▫ History starts post-MVA, he was unrestrained passenger. Post-MVA imaging showed a right subdural, drained surgically. The patient went home 3 days later. ▫ Readmitted 4 weeks later with recurrent right subdural. Again, drained, discharged home 3 days later. ▫ 3 weeks later readmitted with recurrence of right subdural. Again, drained. ▫ NSG confident immediate hemostasis is achieved with each procedure. ▫ A hematology consultation is requested.

The Evaluation • History ▫ Family History and Personal History • Detailed physical examination • Laboratory evaluation ▫ Tailored to the history

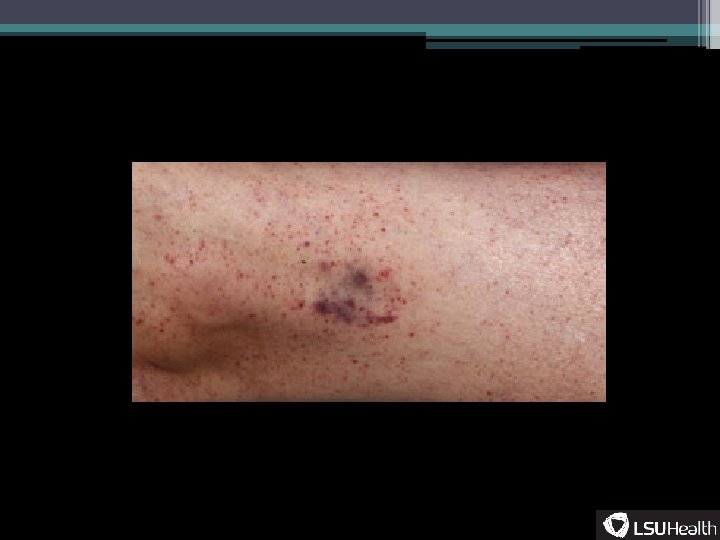
Terminology • Purpura- ▫ Non-blanching purple or bluish lesion from extravasated blood • Petechia- ▫ A specific type of purpura, pinpoint lesions (<5 mm), well demarcated • Ecchymosis- ▫ Larger purpura, can be either confluent petechiae or one hemorrhagic lesion • Hematoma- ▫ 1 cm or larger mass due to bleeding between tissue planes • Palpable purpura- ▫ Raised purpura usually due to leukocyte infiltration

Terminology • Purpura- ▫ Non-blanching purple or bluish lesion from extravasated blood • Petechia- ▫ A specific type of purpura, pinpoint lesions (<5 mm), well demarcated • Ecchymosis- ▫ Larger purpura, can be either confluent petechiae or one hemorrhagic lesion • Hematoma- ▫ 1 cm or larger mass due to bleeding between tissue planes • Palpable purpura- ▫ Raised purpura usually due to leukocyte infiltration

Dermatology accessed 2013

Logical Images accessed 2013

Al Bello/ Getty images, espn. com accessed 2013

medscape. com, accessed 2013

Terminology • Bruise-

Terminology • Bruise▫ This word should be stricken from your vocabulary.

Terminology- Homeostatis Mechanisms • Primary hemostasis: ▫ Problems with formation of the platelet plug ▫ Usual cause of immediate bleeding • Secondary hemostasis: ▫ Humoral coagulation, coagulation that takes place after the platelet clot ▫ Usual cause of delayed bleeding
 May-Hegglin")
Primary Hemostasis Inherited Acquired Iatrogenic von Willebrand disease DIC Drug induced (HIT, quinine) May-Hegglin anomaly Amyloidosis Qualitative platelet disorders (NSAIDS) Glanzmann thrombasthenia Aplastic anemia Post-transfusion purpura Bernard-Soulier syndrome Hypersplenism Gray platelet syndrome Uremia, Turbulent Circulation

Secondary Hemostasis Coag Factor Abnormalities Fibrogen Disorders Connective tissue Factor VIII Deficiency Hypofibroginemia Scurvy Factor IX Deficiency Afibrogenemia Ehlers-Danlos Acquired inhibitors. Factor VIII Inherited dysfibrogenemias Osler-Weber-Rendu Factor II, V, VII, X Deficiency Consumptive fibrogenemias (pit viper envenomation) Factor XI Deficiency

Clinical History • Each case of the bleeding patient much be approached individually ▫ There are no NCCN algorithms for bleeding. • Some clinical situations do not allow for a detailed history. ▫ The intubated patient ▫ The patient with head trauma

Common Bleeding Consultations • The outpatient setting ▫ The patient with an incidental abnormal coagulation test • The inpatient setting ▫ ICU patient ▫ The surgical patient ▫ The immediate pre or post-partum patient

Clinical History • The most predictive factor future bleeding is past bleeding. • Tailor the HPI and data gathering around this point.

Clinical History • Patient surgical history: ▫ What kind of wound? ▫ Bleeding in the peri-operative period? �Timing of peri-operative hemorrhage �Primary v secondary defect �Was transfusion necessary? �How much blood? �What kind of surgery: Cataract ‹--› open AAA repair

Clinical History • Bleeding in the perioperative period? ▫ What were the laboratory abnormalities at the time of bleeding? �PT/PTT, platelet count ▫ How was bleeding stopped?

Easy bruising? • “Yes” is very non-sensitive • Red flags: ▫ Hematomas develop after minor trauma ▫ More than 4 bruises on a baby/toddler �Areas not overlying bony prominences �Axillary lines overlying rib cage �Soles/palms (abuse) • Lateral aspects of arms, 3 foot high bruises on legs Carpenter 1999

Pregnancy • Bleeding before 20 weeks: ▫ Miscarriage ▫ Ectopic pregnancy • Bleeding during delivery: ▫ Placental abruption ▫ Uterine rupure • Bleeding after 20 weeks: ▫ Placenta abruption ▫ Placenta previa • Post-partum hemorrhage: ▫ Uterine atony ▫ Laceration ▫ Retained placenta ▫ defined as : �>500 ml in vaginal delivery �>1000 ml in C-section

Pregnancy • Disseminated intravascular coagulation: ▫ Most common cause of bleeding around delivery �Abruptio placentae �Eclampsia �Retention of dead fetus �Amniotic fluid embolism �Placental retention �Sepsis • Mild to moderate v. WD do not bleed in the puerperium

Menorrhagia • Difficult to quantitate ▫ Heavy menstrual flow for >3 days ▫ Menstruation lasting >7 days • OCPs to control menstrual bleeding in the absence of anatomic defects? ▫ OCPs may make v. WD diagnosis challenging

Excessive bleeding • Teeth extractions • Loss of deciduous teeth • Razor cuts ▫ Crude bleeding time • Delayed wound healing ▫ Factor XIII deficiency ▫ Dysfibrogenemia

Prothrombin Thrombin Fibrinogen Fibrin

Factor XIII Prothrombin Thrombin Activated Factor XIII Fibrinogen Fibrin Mature. crosslinked fibrin clot

Nose bleeds • Non-traumatic nosebleeds post-pubertal patients lasting more than 5 minutes. • Epistaxis is reported in 5 -40% of all patients • Only 27% have an indentifiable bleeding disorder • True excess epistaxis: ▫ v. WD, hereditary telangectasia Sadler Blood 2003

Medications • Warfarin, DTIs, Heparin • NSAIDS • IIb/IIIa inhibitors

Medications • Warfarin, DTIs, Heparin • NSAIDS • IIb/IIIa inhibitors • • • Garlic excess Vitamin E, Vitamin C, ginger Black tree fungus Antibiotics Iron supplments (DUH)

Medications • Warfarin, DTIs, Heparin • NSAIDS • IIb/IIIa inhibitors • Garlic excess • Vitamin E, Vitamin C, ginger • Black tree fungus • Antibiotics? ? ? • Iron supplments (DUH)

Family History • Sex-linked recessive: ▫ Hemophilia A+B ▫ Wiskott-Aldrich Syndrome (thrombocytopenia, small plts, eczema) • Autosomal dominant: ▫ v. WD ▫ Osler-Weber-Rendu ▫ Dysfibrogenemia • Autosomal recessive: ▫ Factor VII deficiency ▫ Bernard-Soulier Syndrome (thrombocytopenia, BIG plts, Ib-IX defect)

Physical Exam Findings Diagnosis Finding Scurvy Subcutaneous bleeding, perifollicular purpura Thrombocytopenia Petechia Hemophilia Hemarthosis, uncontrolled, delayed post-op bleeding. Extensive, uncontrolled bleeding (acquired) Vitamin K Deficiency Hematuria, soft tissue hemorrhage Hyperfibrinolysis (APL) Ecchymoses Warfarin ingestion Hematuria, soft tissue hemorrhage Amyloidosis Soft tissue hemorrhage Adapted from Kessler 2007

Laboratory assessment • History and physical examination non-specific • Many patients will not be able to provide history • Many patients may never had a hemostatic challenges

Laboratory tests to start with in a bleeder • • • CBC, peripheral smear Prothrombin time activated Partial Thromboplastin Time Thrombin Time Fibrinogen concentration Bleeding time or PFA

Case 1 • Forty seven year old healthy woman has a lap chole converted to an open procedure due to oozing of blood from small ligated arteries; several need to be re-tied. • Post-operatively, she is noted to have oozing of blood around the surgical site. There is ecchymosis around the wound that worsens over 2 days. • A hematology consult is requested.

Case 1 • Hemostatic defect? • CBC normal. ▫ Normal platelet count, normal sized platelets ▫ Hgb normal • PT/PTT were normal • Fibrinogen concentration normal • Platelet function assay was normal • What next?
. ▫ 10 minutes, via the")
Case 1 • Bleeding time was obtained (with difficulty). ▫ 10 minutes, via the Duke method ▫ Prolonged • Diagnosis?

Case 1 • On more detailed it is noted the patient is able to extend the distal aspect of her thumb past 90 degrees. • Skin ‘translucent’

Case 1 • Ehlers-Danlos

Case 2 • 64 year old man Korean War veteran has a TURBT for a T 1 bladder tumor. The patient is readmitted two days after the procedure with hematuria. • Repeat cystoscopy shows small amount of bleeding at the resection site. • Foley catheter remians in place. The patient continue to have hematuria, requiring PRBCs every 3 days. Urology confident there are no arterial bleeders. • A hematology consultation is requested after a three week hospitalization.

Case 2 • Hemostatic defect? • CBC : mild thrombocytopenia, platelet count 98 K. Normal otherwise. • PT 11 s • PTT 40 s • PFA normal.

Case 2 • Next step?

Case 2 • PTT 1: 1 mix: ▫ 33 seconds • Possible diagnoses?

Case 2 • VWF Ag: normal • Factor IX activity: 110% • Factor VIII activity: 13% • Diagnosis ?

Case 2 • Mild hemophilia VIII unmasked by unusual hemostatic challenge • Further review of history: ▫ Mother’s brother died after falling from a tractor at 13 years old in 1930 s ▫ PTTs checked multiple times at VA. �At least 20 results available in CPRS before heme consult requested

Case 2 b • Hemostatic defect? • CBC was normal. • PT normal every admission • PTT 39 s

Case 2 b • PTT 1: 1 mix: Normal • Possible diagnoses?

Case 2 b • v. WF antigen: normal • Factor IX activity: 90% • Factor VIII activity: 19%

Case 2 b • Mild Factor VIII deficiency • On extensive review of the history: ▫ The patient had a PTTs of 39 -40 s throughout his multiple hospitalizations. ▫ No family history of bleeding.

PTT Elevation- Clinical correlates **There is no such thing as barely abnormal. **High does not always equal bleeding potential Factor VII deficiency: no effect on PTT, only PT Factor VIII deficiency: 36 -45 s Factor IX deficiency: 36 -45 s Factor X deficiency (think amyloid!): variable, can be very high, PT also elevated Type I v. WF: 36 -45 s Factory XI Deficiency 70 -90 s Factor XII Deficiency (rare, no bleeding): >100 s The lupus anticoagulant: >100 s Heparin contamination: Undetectably high no reference, experiential

Case 3 • 33 year old man sent to you to evaluate for a bleeding disorder before an excisional lymph node biopsy. • Has had nose bleeds on occasion lasting 10 -15 minutes at least 3 times per month. ▫ (Admits, reluctantly, to being a picker. ) • He did not play sports. • He was circumcised at birth. No other surgeries. He is an only child. • His family history was the red flag: his mother bled ‘a lot’ with periods and had a hysterectomy at 32. ▫ He remembers his mother stayed in the hospital for ‘a while’ after surgery. He does not remember much else as he was 5 years old. ▫ His mother had a cholecystectomy 6 years later with an extended hospitalization, received blood.

Case 3 • CBC is normal • PTT is normal today, was 38 s three weeks ago. • Fibrinogen normal • Next step?

Case 3 • PFA or Bleeding time. ▫ PFA abnormal: 180 seconds (normal <116 s) • Thoughts, next step?

Case 3 • v. WF antigen: 40% • v. WF activity (ristocetin cofactor and collagen binding): 45% • Factor VIII activity: 42% • v. WF multimers: normal distribution

Case 4 • You called to see an ICU patient for bleeding. The patient is intubated and sedated. He was in a car wreck 3 weeks ago and is now bleeding per rectum. • The overnight critical care intern tells you the patient is on no ‘blood thinners’ and no antiplatelet drugs. • He thinks some of the labs are abnormal, but he can’t recall: “The patient isn’t mine, I’m just cross covering. ”

Case 4 • Since the resident does seem to know what is going on you elect to leave a fascinating noon conference to see the patient. • On exam the patient is oozing serosanginous fluid from three venipuncture and once central line site. The patient has a femoral line in place. He is febrile and on two pressors. • The MAR is poorly maintained but shows the patient to only be on cefepime and vanc. • Labs from this AM show a normal CBC. PT/PTT from 2 weeks ago were normal. • Creatinine is 4. 5, but patient not yet on dialysis

Case 4 • You send a stat PT/PTT and the results show a PT of 11 seconds and a PTT of 150 seconds.

Case 4 • You send a stat PT/PTT and the results show a PT of 11 seconds and a PTT of 150 seconds. • PTT 1: 1 mix 150 seconds

Case 4 • You send a stat PT/PTT and the results show a PT of 11 seconds and a PTT of 150 seconds. • PTT 1: 1 mix 150 seconds • Thrombin time: ∞ • Diagnosis:

Case 4 • You send a stat PT/PTT, fibrinogen and the results show a PT of 11 seconds and a PTT of 150 seconds, fibrinogen is normal. • PTT 1: 1 mix 150 seconds • Thrombin time: ∞ • Diagnosis: Heparin

Thrombin Time • Excess thrombin added to patient’s plasma • • Heparin Fibrin split products Factor XIII deficiency Fibrinogen deficiency

Case 4 • You contact the pharmacy to verify every drug being dispensed to the patient. • He has been getting Heparin 5000 units sq every 8 hours as part of the ICU protocol. ▫ Not listed on the MAR in the ICU.

Abnormality Platelet count Bleeding time PT PTT Platelet Aggreg Mixing Studies Fibrinogen DIC Low Elevated Normal Corrects Low ITP Low Elevated Normal Normal v. WD Normal Elevated or Normal Abnormal Corrects Nornal Heparin Excess Elevated Does not correct
- Slides: 66