The bleeding obvious Anticoagulation in Trauma Ben Bailiff

The bleeding obvious: Anticoagulation in Trauma Ben Bailiff Consultant Haematologist UHCW

Agenda • • 30 mins Anticoagulation 2019 General principles Reversal agents Direct oral anticoagulant (DOAC) levels Effective pathways Dos and don’ts Questions

TARN data Age n % Under 16 yrs 2407 4. 9% 16 -65 yrs 24093 48. 6% Over 65 yrs 23037 46. 5% ~1. 5% population receiving anticoagulation 18% population > 80 predicted to have AF 3 x number of patients on DOACs in last 2 years Indications for anticoagulation are widening Reversal agents available – at a price and to what effect?

Historical DVT service New DVT - ambulatory pathway/inpatient 6 months anticoagulation - VKA End of story 2 nd VTE - Life long anticoagulation

Risk of recurrent VTE based on history of index event Unprovoked Risk of recurrence after unprovoked VTE 30 -40% after 5 -10 years Non-surgical risk factor Post-surgery Cambridge cohort Baglin et al Lancet 2003; 362: 523– 26

AF patients – anticoag clinic DVT service 2019 New DVT - ambulatory pathway/inpatient DVT nurse review 3 weeks Concerning patients 3/6 months anticoagulation - DOACs Thrombosis clinic review +/PVD review STOP Long term anticoagulation General practice Long term follow up

Amplify-Ext: Apixaban for VTE Apixaban 2. 5 mg bd Apixaban 5 mg bd Placebo Recurrent VTE 1. 7% 8. 8% Major bleeding 0. 2% 0. 1% 0. 5% 3% 4. 2% 2. 3% Non-major bleeding Major or Clinically Relevant Non-major Bleeding n = 813 n = 840 n= 829 N Eng J Med 2013; 368: 699 -708

Atrial Fibrillation • Rapid diagnosis clinics • Greater awareness • Technology • Clinician interest • Decreasing the number of undiagnosed patients? Increasing number of patients of anticoagulation

Trends DOACS Warfarin/VKA Why? Plethora of trial data suggesting equal efficacy yet decreased risk of bleeding (47% RR) + mortality rate is decreased if you bleed on a DOAC vs VKA (~30% RR) Chai‐Adisaksopha C, Hillis C, Isayama T, Lim W, Iorio A, Crowther M. Mortality outcomes in patients receiving direct oral anticoagulants: a systematic review and meta‐analysis of randomized controlled trials. J Thromb Haemost. 2015; 13: 2012‐ 2020. Xu Y, Schulman S, Dowlatshahi D, Holbrook AM, et al. bleeding effected by direct Oral anticoagulants (BLED‐AC) study group. Chest. 2017; 152: 81‐ 91.

New indications • Long term secondary prevention VTE • Dual antiplatelet + anticoagulant therapy (COMPASS) • Post CNS haemorrhage (RESTART) • Cancer associated thrombosis (CAT) • CAT prophylaxis for ambulatory patients J. W. Eikelboom et al. Rivaroxaban with or without Aspirin in stable cardiovascular disease. N Engl J Med. 2017; 377: 1319 -1330 Restart collaboration. Effects of antiplatelet therapy after stroke due to intracerebral haemorrhage (RESTART). Lancet 2019; 393: 2613 -23

General principles of managing anticoagulation in trauma patients • Early recognition of anticoagulant • Consider impact of anticoagulation (or antiplatelets) • Simple measures – hydration, local measures, activated charcoal (if appropriate < 3 hrs exposure) • Maintain Hb (>80) • Consider trauma coagulopathy • Tranexamic acid (as per CRASH 2)

Tranexamic acid • Not trying to teach you to suck eggs • It works, it’s cheap. • No thrombosis risk – not only in trauma trials • Main risk – seizures (excessive dosing required) • Major benefit – 1 st 3 hours

Anticoagulant Measurements • INR – clearly indicates level of VKA effect in warfarin patients only • INR/PT/a. PTT – no correlation with DOAC anticoagulant effect For example – Apixaban 40 -80% patients with a normal PT/a. PTT will have significant levels of circulating Apixaban NO simple coagulation screening tests available for DOACs

Bleeding? European Heart Journal, Volume 37, Issue 38, 7 October 2016, Pages 2893– 2962, https: //doi. org/10. 1093/eurheartj/ehw 210
 reversal for")
Life or limb threatening bleeding Anticoagulant Reversal • Prothrombin complex concentrate (PCC) reversal for VKA • PCC is often used to reverse DOACS • Until recently no direct antidote for DOACS • Haemodialysis for dabigatran?

Warfarin/VKAs • Do not use FFP • Always give vitamin K • Use 4 factor PCC (Beriplex or Octaplex) • Repeat INR post reversal Reverses effect rapidly, but short half life R. Sarode et al. Efficacy and safety of 4 factor Prothrombin complex concentration in patients on vitamin K antagonists presenting with major bleeding. Circulation 2013; 128: 1234 -43

DOACs • Rivaroxaban Xa = anti Xa • Edoxaban • Apixaban • Dabigatran Short half life Renal/liver clearance Peak and trough effect No Xa = DTI

PCC DOACs • • • Preclinical data suggests pro-coagulant effect Only case series or retrospective data 70% effective haemostasis noted Meta analysis - disappointing Thrombosis rate 4. 8 -7. 8% Mortality ~ 10% S. Piran et al. Management of direct factor Xa inhibitor related major bleeding with prothrombin complex concentrate – a meta analysis. Blood advances. 2019. 3(2): 158 -167
 • Monoclonal antibody fragment to dabigatran only • REVERSE AD trial -")
Idarucizumab (Pragbind) • Monoclonal antibody fragment to dabigatran only • REVERSE AD trial - 500+ patients in trial • Trial testing effectiveness of drug in reversing dabigatran in 2 scenarios a. Uncontrolled haemorrhage b. Emergency surgery Delivered as 2 X 2. 5 g infusions (15 minutes apart) • Pollack C. Idarucizumab for dabigatran reversal – full cohort analysis. N Engl J Med 2017; 377: 431 -441

Bleeding

Pragbind • Median time to cessation of bleeding 2. 5 hours • Median time to operation in surgical group 1. 6 hours (normal or mildly abnormal haemostasis in 95% patients) • Only 1 dose in 98% cases • Approximately 5% thrombotic rate in next 20 days Minimal pro-thrombotic effect
 • Recombinant derivative of Factor Xa without intrinsic catalytic activity. Higher")
Andexanet Alfa (Ondexxya) • Recombinant derivative of Factor Xa without intrinsic catalytic activity. Higher affinity to Xa inhibitors than Xa – decoy drug. • Good anti-Xa inhibition demonstrated in healthy volunteers • Reverses all Xa inhibitors

Bleeding patients • Multicentre, prospective, open label, single treatment arm • Patients admitted with bleeding and treated with bolus plus a 2 hour infusion of Andexenat alfa. • 352 patients in analysis of ANNEXA 4 Delivered as a Bolus and infusion. Several vials need to be constituted. Andexenat Dose based upon time of ingestion and dose of DOAC. • Connelly S et al. Full study Report of Andexenat Alfa for bleeding associated with factor Xa inhibitors. NEJM 2019; 380: 1326 -1335
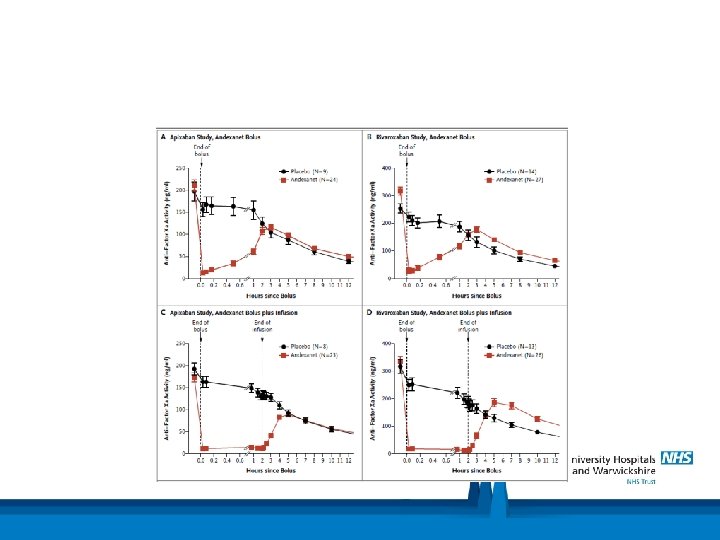

Results • Levels of anti. Xa in both R and A treated patients reduced by 90% and were sustained during infusion • Clinical haemostasis judged to be excellent or good in 82% patients 12 hours post treatment • Thrombosis rate 10% during 30 days follow up • Mortality 14%

BUT… • • No comparator Most unwell patients excluded High thrombosis rate No relationship between reducing Xa levels and haemostatic effectiveness noted in the results • 1/3 rd patients CNS haematoma increased >33% from baseline – judged to be good? • Not randomised, un-blinded Is this a clinical trial…or an advertisement? • FDA accelerated approval – (pending RCT data) for the reversal of Rivaroxaban & Apixaban. • Black box warning concerning risk of arterial and venous thrombosis
, a level")
DOAC levels • DOACs do not need monitoring • Certain situations (TRAUMA), a level may be useful • Prevent unnecessary reversal ££ Thrombotic risk • DOAC calibrated anti Xa levels (surrogate for drug level, suggest level of inhibition of Xa by the DOAC) • Hemoclot assay – Dabigatran assay • <30 ng/ml – no need for reversal • ANNEXA 4 – 28% patients included did not need reversal

28% no need to reverse! Why? • Elderly population • Adherence issues • Chronic illness • Drug interactions ‘First do no harm’

Effective pathways • Levels are only useful if they are integrated into effective pathways • Rapid TAT • Clear guidance on the shop floor • Reversal agents rapidly available • Support from haematology

DOASENSE urine test • DOASENSE POCT • DOAC dipstick – Qualitative, all in one, POCT for Xa inhibitors and thrombin inhibitors • 10 minute turnaround • Yes/No answer only – presence of DOAC at a level sufficient to result in bleeding NCT 03182829 observational study

IVC filters • Not recommended prophylactically in trauma patients • No overall benefit – only if absolute contraindication to anticoagulation + thrombosis • If one is inserted – refer for removal at insertion • Dedicated review service at UHCW K. M. Ho et al. A multicentre trial of Vena cava filters in severely-injured patients. ISTH abstract. 2019.

Do’s and Don’ts DO • Act promptly • Involve haematology • Recognise anticoagulants • Consider effectiveness of reversal agents • Reinstate anticoagulation ASAP DON’T • Insert prophylactic IVC filters • Forget TXA • Use the reversal agents unless severe bleeding • Routinely reverse anticoagulants in trauma in the absence of bleeding

Questions?
- Slides: 33