The basics of AKI and CKD Dr Jon

The basics of AKI and CKD Dr Jon Murray Consultant Nephrologist James Cook University Hospital

Acute Kidney Injury v Chronic Kidney Disease § • Creatinine 1250 mol/l • What are the priorities? 1. How is the patient? Is this single or multi-organ failure? 2. Are there life-threatening complications of kidney failure? 3. Is this acute kidney injury or chronic kidney disease? 4. (Might this be due to kidney “disease”? )

AKI a challenge for us all § • All health professionals should be well informed and proactive, recognising at risk patients, how to diagnose AKI and aid AKI recovery Ø 50% of trainees unable to define AKI Ø 30% unable to name more than two risk factors for AKI Ø 37% unable to name even one indication for renal referral Muniraju et al. 2012 • NHS campaign to improve the care of people at risk of, or with, AKI “Wherever you work and whatever your role in health or care you should be aware of AKI so that we can work together to reduce the risk of AKI and the number of patients suffering as a result of AKI. ”

Acute Kidney Injury v Chronic Kidney Disease § 1. How is the patient? Is this single or multi-organ failure? Ø Acute Kidney Injury ∞ Acute Disease Severity Marker Ø CRP elevated acute inflammation (sepsis, post-op, arthritis) Ø Cr elevated acutely often indicates patient is sick

CONTEXT Deteriorating Patient AKI alert AKI Risk AKI is… Vulnerable Patient Safety Thermometer Relevant to All Patients

AKI as a Patient Safety Thermometer Presence of AKI often indicates presence of acute illness § Acutely Unwell Patient CRP Acute Kidney Injury BP HR Temp Deteriorating Patient Creatinine Urine output Prompt recognition and good management of AKI requires and often reflects Prompt recognition and good management of acutely unwell patients

Acute Kidney Injury v Chronic Kidney Disease § 2. Are there life-threatening complications of kidney failure? Ø Is dialysis necessary? Ø Is dialysis feasible? Ø What about medical therapies?

Acute Kidney Injury v Chronic Kidney Disease § 2. Are there life-threatening complications of kidney failure? Ø Is dialysis necessary? Indications for dialysis (or CVVH) during AKI Indications dialysis therapy) ‘A HOPE’ • Refractory hyperkalaemia (K+ >for 6. 5 despite medical for survival • Refractory fluid overload (especially pulmonary) +/- anuria (despite intervention for obstruction) • • Acidosis Refractory acidosis (p. H < 7. 15 despite medical therapy) • • Hyperkalaemia Uraemic pericarditis or encephalopathy • Oedema (of lungs) • Pericarditis Discuss with renal and / or critical care team if above parameters present and registrar / consultant • reviewing Encephalopathy patient feel dialysis / CVVH referral appropriate within wider clinical context

Acute Kidney Injury v Chronic Kidney Disease § 2. Are there life-threatening complications of kidney failure? Ø Is dialysis feasible? Dialysis referral and clinical context Points to consider prior to renal / critical care referral • Dialysis can precipitate haemodynamic collapse, especially during acute illness associated with 1. Hypotension 2. Poor cardiac reserve 3. Multiple co-morbidities • Decision to dialyse patient or not should thus incorporate 1. Opinion of consultant looking after patient integrating overall clinical picture to assess if dialysis (possibly permanent) +/- critical care support +/- CPR is feasible and appropriate 2. Critical care opinion if blood pressure already low +/- other organ failure present 3. Opinion of patient / next of kin regarding dialysis (possibly lifelong) & CPR (unless emergency)

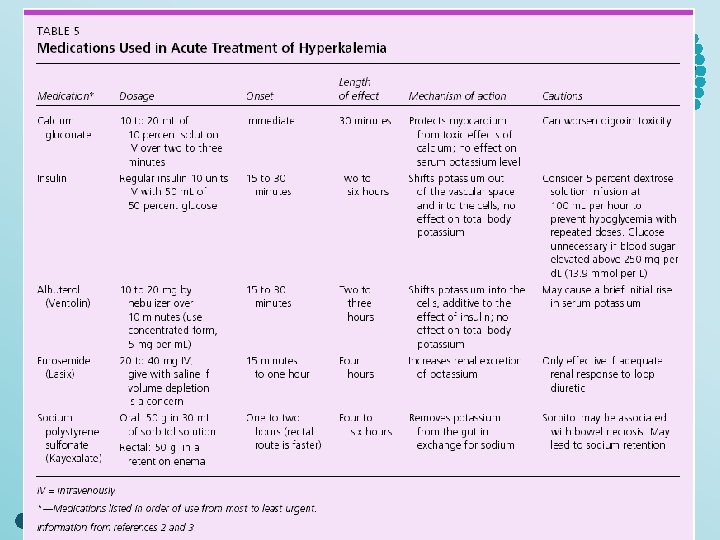
Acute Kidney Injury v Chronic Kidney Disease § 2. Are there life-threatening complications of kidney failure? Ø What about medical therapies? Treatment of Hyperkalaemia 1. If ECG changes 10 mls of 10% calcium gluconate via large vein over 10 mins & monitor ECG 2. If K+ > 6. 5 mmol/L or ECG changes 50 mls of 50% dextrose with 10 units of short-acting insulin over 15 mins & monitor BMs (15 mins post dose & then hourly for 6 hrs) to avoid hypoglycaemia 3. If K+ > 6. 5 mmol/l consider 10 mg nebulised salbutamol (avoid if angina or HR > 100 bpm) 4. Institute low potassium diet and avoid potassium-retaining medication 5. If K+ > 6. 5 mmol/l consider calcium resonium 15 g orally or 30 g per rectum (with laxatives) 6. If HCO 3 - also 15 mmol/L consider giving bicarbonate (refer to acidosis guidance)

Hyperkalaemia : ECG changes §
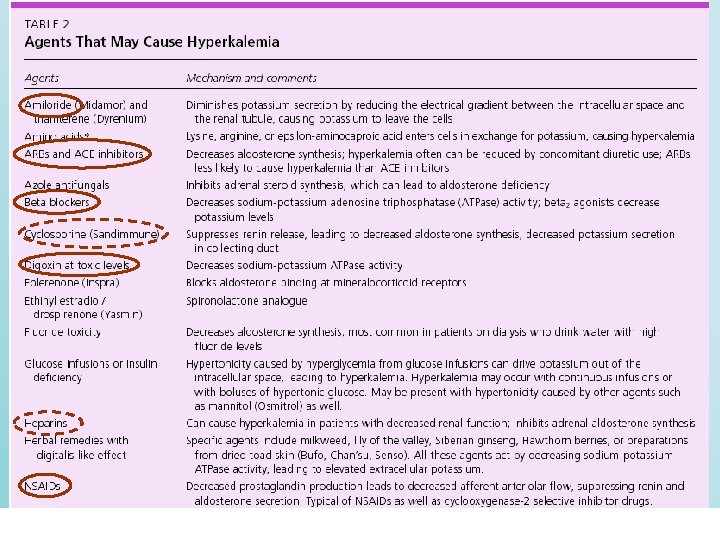

§ Agents that may cause hyperkalaemia 2

Acute Kidney Injury v Chronic Kidney Disease § 2. Are there life-threatening complications of kidney failure? Ø What about medical therapies? Treatment of Acidosis • Sodium bicarbonate therapy for acidosis in AKI often reserved for co-treatment of hyperkalaemia and acidosis, usually in clinical context of volume depletion • If venous bicarbonate 16 mmol/l consider giving sodium bicarbonate either as • 500 -1000 mg QDS orally (stop if bicarbonate rises to > 22 mmol/l or fluid overload) • 500 mls of 1. 26% sodium bicarbonate iv over 1 hour • If p. H 7. 15 • consider early critical care input and dialysis if acidosis refractory to medical interventions • ensure other causes of metabolic acidosis are identified and treated Cautions regarding sodium bicarbonate therapy in AKI • Bicarbonate therapy can worsen fluid overload and i. Ca 2+ Avoid if either parameter present • Intravenous bicarbonate and intravenous calcium should not be given via same IV cannula

Acute Kidney Injury v Chronic Kidney Disease § 2. Are there life-threatening complications of kidney failure? Ø What about medical therapies? Treatment of Pulmonary oedema • Sit the patient up and give oxygen (60 -100% unless contraindicated) • If haemodynamically stable iv furosemide 80 mg and consider GTN infusion 1 -10 mg / hour • If haemodynamically unstable early critical care input & consideration of respiratory support Notes regarding furosemide therapy in AKI • Do not use furosemide during AKI to expedite renal recovery no proven benefit • Furosemide mainly reserved for pulmonary oedema in non-oliguric AKI without hypotension

Acute Kidney Injury v Chronic Kidney Disease 3. Is this acute kidney injury or chronic kidney disease? Ø Old blood results? Ask Patient /GP? Ø What about if no old notes / results? Ø Anaemia Ø Bone Chemistry Ø Clinical tolerance Ø Size of kidneys §

Acute Kidney Injury v Chronic Kidney Disease § CKD commonly secondary to: • • • Diabetes Glomerulonephritis Hypertension / Renovascular Disease Reflux nephropathy (chronic pyelonephritis) Polycystic Kidney Disease Ø Patient often well / stable clinical context ∞ ‘steady state’ Ø e. GFR a more valid estimate of renal function

Acute Kidney Injury v Chronic Kidney Disease Ø When should e. GFR be used? Ø When should e. GFR not be used? §

AKI: conventional definitions mention GFR § Ø An abrupt and sustained decline in renal excretory function due to a reduction in glomerular filtration rate (GFR) GFR and renal excretory function

Measurement of renal function in clinical practice § Measurement of GFR and renal excretory function Ø In clinical practice assessment of GFR is usually extrapolated from 1. Serum creatinine level 2. Urine output Ø These two parameters used in conventional ARF definitions because 1. Readily available and inexpensive 2. Usually reflect changes to GFR in steady state of CKD Ø Important caveats / pitfalls during non-steady state of AKI
![AKI: Definition, detection & pitfalls GFR Creatinine (relatively in tandem in steady state [CKD])](http://slidetodoc.com/presentation_image_h/177dc50129794b7f4cade2b85518e15e/image-22.jpg "AKI: Definition, detection & pitfalls GFR Creatinine (relatively in tandem in steady state [CKD])")
AKI: Definition, detection & pitfalls GFR Creatinine (relatively in tandem in steady state [CKD]) 100 Creatinine 1 mg /dl 88 mol/l 50 Creatinine 2 mg /dl 176 mol/l 25 Creatinine 3 mg /dl 265 mol/l 12. 5 Creatinine 4 mg /dl 354 mol/l 6. 25 Creatinine 5 mg /dl 442 mol/l §

AKI definition: AKI is not a primary diagnosis § • AKI is not a primary disease nor single diagnosis • AKI is a syndrome of abrupt kidney dysfunction Usual Baseline Kidney Function Increased Risk Kidney Damage Stage 1 AKI Stage 2 AKI Stage 3 AKI

No biomarker of kidney injury no renal troponin Creatinine changes indicate kidney function changes §
 Serum Creatinine 2")
AKI: Definition AKI Definition (Kidney Disease Improving Global Outcomes, KDIGO criteria) Serum Creatinine 2 § Urine Output 4 Increase in serum creatinine by >26 mol/L ≤ 48 hrs AKI Definition Increase in serum creatinine by ≥ 1. 5 times baseline 3 which is known or presumed to have occurred within previous 7 days Urine volume <0. 5 m. L/kg/hr for ≥ 6 hrs timescale of creatinine change is central to AKI definition if no recent preceding blood test then incorporate clinical context to determine if creatinine change likely to have occurred during preceding week (ie. ‘acutely’). 2 Note 3 ‘Baseline’ creatinine value should be considered as the patient’s ‘usual’ creatinine when clinically well determine by reviewing patient’s previous blood results within clinical context. Assume normal baseline if no previous blood tests. 4 In practice urine output criteria can only be applied to hospitalised patients who are catheterised - but a reliable history of low or absent urine output should alert the clinician to the possibility of AKI.
 AKI Stage")
AKI: Staging AKI Staging (Kidney Disease Improving Global Outcomes, KDIGO criteria 1) AKI Stage 1 Serum Creatinine Urine Output Increase in serum creatinine by >26 mol/L ≤ 48 hrs OR an increase in serum creatinine by ≥ 1. 5 x baseline 2 urine output <0. 5 m. L/kg/hr for 612 hrs Increase in serum creatinine by ≥ 2 x baseline 2 urine output <0. 5 m. L/kg/h for ≥ 12 hrs Stage 2 Stage 3 2 § Increase in serum creatinine by ≥ 3 x baseline 2 OR an increase in serum creatinine by ≥ 1. 5 baseline to > 354 mol/L urine output <0. 3 m. L/kg/h for ≥ 24 hrs OR anuria for ≥ 12 h When creatinine change is known or presumed to have occurred within previous 7 days

AKI recognition: Establishing baseline creatinine is key § • Several parameters affect usual baseline serum creatinine levels in normal steady state • Balance of creatinine production (from muscle turnover) and creatinine excretion (by kidneys) Reduced kidney function (Chronic Kidney Disease) Creatinine Reduced muscle mass Age (years) Black males Other males Black females Other females Typical Normal Baseline Creatinine Values (µmol/l) Usual Baseline 20– 24 133 115 106 88 25– 29 133 106 97 88 30– 39 124 106 97 80 40– 54 115 97 88 80 55– 65 115 97 88 71 >65 106 88 80 71

AKI Recognition: Be particularly vigilant for AKI in patients at increased risk of § AKI • Most patients with acute illness are at acute risk of developing AKI • Many patients remain at persistent AKI risk due to baseline physiology / chronic disease Acute Risk Usual Baseline Increased Risk AKI Chronic Risk • Acute severe illness • Elderly Age (age > 75) • Hypovolaemia • CKD (GFR <40 ml/min) • Some drugs during acute illness • Cardiac Failure Kidney • Sepsis Damage Stage 1 AKI Stage 2 Stage 3 • Diabetes Mellitus AKI
 precedes creatinine or urine output GFR")
AKI: Kidney damage underlying kidney dysfunction ( GFR) precedes creatinine or urine output GFR Creatinine Not in tandem§during AKI Acute Illness Usual Baseline Increased Risk 100 Creatinine 88 mol/l 50 Creatinine 176 mol/l 25 Creatinine 265 mol/l 12. 5 Creatinine 354 mol/l 6. 25 Creatinine 442 mol/l No reliable biomarkers of kidney damage Changes to biomarkers of kidney function (serum creatinine / urine output) occur some time after kidney insult / damage 1 Stage 2 true GFR, Stage • Stage Poor correlation between e. GFR 3 and AKI creatinine during AKI assess. AKI serum creatinine changes when detecting / tracking AKI • • Kidney Damage Ø AKI detection requires comparing a patient’s current creatinine against their baseline creatinine Ø Review previous and current blood tests within clinical context

AKI: Definition, detection & pitfalls PITFALL 2: • GFR is not only the determinant of renal creatinine excretion • Renal excretion of creatinine glomerular filtration PLUS tubular secretion §

AKI: Definition, detection & pitfalls • Tubular secretion of creatinine most relevant to • Patients with CKD and early in course of AKI §

AKI: Definition, detection & pitfalls § • Drugs blocking tubular secretion of creatinine • Increase serum creatinine independent of GFR (especially in patients with CKD)

AKI versus ARF § How do we interpret serum creatinine and urine output? What is ‘normal’ creatinine? What represents a significant change in creatinine? Over what timescale? What is ‘normal’ urine output? Can AKI occur in the presence of ‘normal’ urine output? Variable definitions / criteria have hindered recognition, management and research into ARF. Why the change in nomenclature from ARF to AKI?

AKI: Definition, detection & pitfalls § Recognised that following an acute insult to the kidney… Even small rises in serum creatinine are independently associated with increased mortality and hence are incorporated into AKI definitions Creatinine 26 -35 44 -80 88 -168 >176 mol/l Unadjusted Age & gender adjusted Multivariable adjusted for age, gender, diagnosisrelated group, weight, CKD status, and ICD -9 -CM codes for respiratory, gastrointestinal, malignant, & infectious diseases n= 1564 885 246 105 Although causality fullyinestablished this and other studies Mortality associated withnot change serum creatinine. Chertow et al. (2005). indicate J Am Socthat patients do not just. An die of their co-morbidities AKI’ but ‘from(95% AKI’CI Nephrol 16: 3365– 3370. increase in SCr > 0. 5 mg/dl was‘with associated with die a 6. 5 -fold Thomas et & al. ~(2015) Int: 87 (1): 62 -73 5. 0 - 8. 5) increase in the odds of death, a 3. 5 -d increase in LOS, $7500 Kidney excess costs.

Pitfalls to using serum creatinine and urine output to identify § and monitor AKI 1. Changes in serum creatinine do not reliably reflect changes in GFR especially in the non-steady state setting of AKI. 2. As GFR begins to fall in AKI, tubular secretion of creatinine increases attenuating early rises in serum creatinine. 3. Conversely, potential confounding factors mean that serum creatinine levels can change in the absence of GFR change / AKI (eg. high protein intake or use of drugs that affect tubular secretion of creatinine). 4. Severe AKI can exist despite ‘normal’ urine output (‘non-oliguric renal failure’) and changes in urine output can occur before biochemical changes become apparent Thus changes in these parameters often lag behind the kidney insult – and can delay identification and management of (underlying) problem.

Pitfalls to using serum creatinine and urine output to identify § and monitor AKI 5. AKI is typically accompanied by consistent rises in serum creatinine, in the order of at least 26 to 44µmol/l (0. 3 to 0. 5 mg/d. L) per day. 6. Slower rates of serum creatinine rise, especially when inter-dispersed by periodic falls in serum creatinine are more suggestive of pre-renal disease where fluctuations in serum creatinine largely reflect fluctuations in renal perfusion. 7. During cases of established AKI, diminishing rises in serum creatinine during cases may also herald the beginning of renal recovery – especially if accompanied by a rise in urine output.

Causes of AKI – 3 basic concepts 1. AKI is most often a marker of underlying severe illness – Death most often due to cause of AKI – rather than AKI itself – AKI often a ‘severity marker’ (correlating with poorer outcomes) – Oliguria heralds ‘medical review’ in surgical patients 2. Glomerulonephritis is a rare but important cause of AKI – Often poorer patient and renal outcomes – Early recognition vital - early treatment beneficial – Urinalysis is central to early recognition 3. Recognition of obstructive nephropathy is often delayed – Low threshold for diagnosis - especially in elderly males – Early USS vital – especially if anuric §

Glomerulonephritis causing AKI RARE - but - IMPORTANT §

Glomerulonephritis: A basic concept § • A group of kidney disorders caused by inflammation of the kidneys. • Just as arthritis is a group of joint disorders caused by inflammation of the joints.

Inflammation of joints = Arthritis Reactive Osteo Crystal Arthritis Rheumatoid with Systemic Vasculitis Sero -ve Rheumatoid §

Inflammation of glomeruli = Glomerulonephritis Hypertension Urinalysis Anomalies CKD Nephritis Nephritic with Systemic Vasculitis Nephrotic Syndrome Nephritic Syndrome §

Glomerular capillary structure: 4 sites of damage in glomerulonephritis §

Glomerular capillary structure §

Histopathology illustrating glomerular damage that§ underlies active urinalysis Normal EM of GBM EM showing GBM rupture in RPGN

Histopathology illustrating glomerular damage that§ underlies active urinalysis Normal EM of GBM EM showing GBM rupture in RPGN

Glomerular injury in glomerulonephritis §

Suspecting GN as a cause of AKI § REMEMBER to dip the urine! The 3 Rs Rash Rheumo (arthralgia) Respiratory symptoms (ENT symptoms or haemoptysis)

GN and multisystem disease - ‘inflammation elsewhere’ Respiratory Wegener’s Goodpastures CSS Nephritis Rash Rheumatology HSP Lupus Wegener’s §

AKI causes: DJ’S MUSIC CLUB § • Drugs (+/- IV contrast recently? +/- overdose? ) • JVP / fluid balance status (+/- rash, respiratory or rheumo signs? ) • Septic screen (MSU, blood +/- stool & sputum) • Microscopy & urinalysis (+/- 24 hr urine collection) • USS renal • Screen autoantibodies (+/- ASOT, c. ANCA, anti-GBM, RF) • Immunoglobulins & electrophoresis • Complement levels (+/- cryoglobulins) • Creatine kinase • LFTs (+/- leptospirosis serology) & hepatitis serology • Urate level • Blood count (incl. eosinophils), film & coag screen +/- BIOPSY

Acute Kidney Injury v Chronic Kidney Disease § • Creatinine 1250 mol/l • What are the priorities? 1. How is the patient? Is this single or multi-organ failure? 2. Are there life-threatening complications of kidney failure? 3. Is this acute kidney injury or chronic kidney disease? 4. Tailoring drugs

Acute Kidney Injury v Chronic Kidney Disease § Ø Tailoring drugs Medications and AKI: General points 1. Some drugs can have direct toxic effects on kidneys and can cause AKI • Eg. NSAIDS, gentamicin, amphotericin and iodinated radio-contrast agents 2. Other drugs can exacerbate AKI - especially during acute illness or hypovolaemia • All anti-hypertensive drugs (eg. ACE inhibitors, Angiotensin receptor blockers & diuretics) 3. Other drugs accumulate during AKI and effects of drug accumulation cause further patient harm • Eg. Metformin & other diabetic drugs (eg. sulphonlyureas), opiates, gabapentin & digoxin 4. Any new drug should be considered as possible cause of AKI (secondary to interstitial nephritis) • Suspect any drug if it was started shortly before AKI occurred, especially PPI or antibiotics Further resource for medications and AKI NHS England ‘Think Kidneys’ Medicines Toolkit Link

AKI Consistent Management: Northern Region AKI Pathway § Consistent and also linked with One Page Pathway • National AKI Medicines Toolkit • NICE Guidance on management of acutely unwell patients Links to AKI Bundles • NICE guidance for IV fluids 7 bundles provide more detailed information as required • NEWS Track & Trigger Systems • Renal Association Hyperkalaemia Guidance • Intensive Care Society Guidance on patient transfer Reference guide outlining steps to consider when managing AKI

Acute Kidney Injury v Chronic Kidney Disease Ø How to distinguish AKI from CKD Ø When dialysis required Ø Medical management of AKI Ø Definition and causes of AKI and CKD Ø Use and misuse of e. GFR Ø Medications and kidney dysfunction Ø Glomerulonephritis as a cause of AKI §
- Slides: 53