THE BASIC SURGICAL SKILLS Inflammation and wound healing

THE BASIC SURGICAL SKILLS

Inflammation and wound healing • • • Vascular response Initial vasoconstriction as a direct response to trauma Exposed subendothelial tissue activates coagulation and complement cascades Platelet adhesion and aggregation causes clot formation Degranulation of platelets releases growth factors and chemotactic factors Inflammatory response due to histamine and 5 HT release produces: – Vasodilatation – Increased capillary permeability – Margination of neutrophils • • Cellular response Migration of neutrophils, macrophages and lymphocytes Macrophages produce growth factors leading to migration of fibroblast and epithelial cells. This causes cellular proliferation with three components: – Epithelialisation – Contraction – Fibroplasia

• Epithelial barrier important to prevent infection and maintain fluid balance • Achieved by both migration and proliferation of epithelial cells • Migration require presence of granulation tissue • When epithelial cover complete contact inhibition prevents further epithelial growth • Contraction can account for up to 80% reduction in wound size • Contraction due to myofibroblasts in granulation tissue • Fibroplasia due to procollagen production by fibroblasts • Intra and intermolecular bonds form the Collagen fibres with triple helical quaternary structure • Extracellular matrix contains Fibronectin and Glycosaminoaglycans • Regulates collagen synthesis and cellular differentiation • Accompanied by simultaneous angiogenesis • Proliferation is followed by remodeling • Maximum collagen production occurs at 20 days • Maximum wound strength at 3 to 6 months • Initial collagen production disorganised • Remodelling lines it up with stresses in skin • Reduced vascularity and cellularity
 Insulin Like Growth Factor")
Important growth factors • • Platelet Derived Growth Factors (PDGF) Insulin Like Growth Factor (IGF-1) Epidermal Growth Factor (EGF) Transforming Growth Factor (TGF�) Factors influencing wound healing • Systemic factors – Age and Sex – Nutrition – Vitamin and trace element deficiencies - vitamin C, vitamin A, zinc – Drugs – steroids, chemotherapy, immunosuppression – Systemic disease – diabetes, jaundice, malignancy – Hypoxia • Local Factors – – Blood Supply Infection Foreign Bodies Surgical Technique

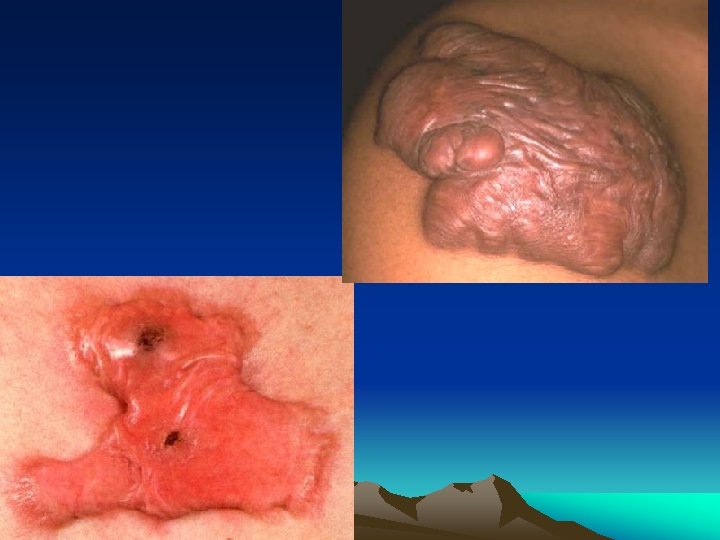
Scars and contractures • Scar formation • Factors influencing scar formation – – – – Individual genetic make up Race Anatomical site Wound tension Age Placement of incision Surgical technique • To minimise the degree of postoperative scarring: – – – Incisions should run along Langer's lines The finest suture possible should be used Tension should be avoided Sutures should be removed as soon as possible Traumatic wounds should be clean and edges excised Exposure to sunlight should be avoided in the early postoperative period

Problematic scars Contractures • • Result if scars shorten Particularly seen in badly aligned scars not corresponding to Langer's lines Can reduce joint mobility May require a z-plasty or skin graft Depressed scars • • • Result if skin becomes attached to deep tissue Can be treated by release of normal skin from margins of scar Scar is then de-epithelialised and skin edges closed over the top Keloid and hypertrophic scars • • All scars become red and thickened during the normal healing process After several months maturation results in flattening of the wound In some scars collagen formation is excessive Results in elevated and red scar If confined to wound = hypertrophic scar If extends beyond wound into normal tissue = keloid scar Seen particularly in patients of Afro-Caribbean origin Particularly affects scars on the presternal and deltoid areas

Surgical technique • Incisions and wound closure • Diathermy, laser – Diathermy – Laser • Sutures and ligature materials • Fundamental skill • Surgical drains

Wound closure 1. Simple interrupted • Insert needle through the skin at right angles including enough subcutaneous tissue to aid in everting the skin edges • Exit through skin of the opposite edge at the same angle including a comparable volume of subcutaneous tissue.
![2. Simple continuous • Insert needle as in [1] • Continue suturing without tying](http://slidetodoc.com/presentation_image_h/28bef528e7eef60627f7a26b83ffea1f/image-10.jpg "2. Simple continuous • Insert needle as in [1] • Continue suturing without tying")
2. Simple continuous • Insert needle as in [1] • Continue suturing without tying , over and over at fixed intervals and tie at the end. 3. Vertical Mattress

3. Subcuticular continuous • Starting from one end of the incision, insert needle through the dermis taking small bites alternately on one side and then the other • Maintain sutures at same depth from the edge on both sides. • At the end the sutures can be taped to the skin or tied over a dressing.

Diathermy • Diathermy is the use of high frequency electric current to produce heat • Used to either cut or destroy tissue or to produce coagulation • Mains electricity is 50 Hz and produces intense muscle and nerve activation • Electrical frequency used by diathermy is in the range of 300 k. Hz to 3 MHz • Patients body forms part of the electrical circuit • Current has no effect on muscles

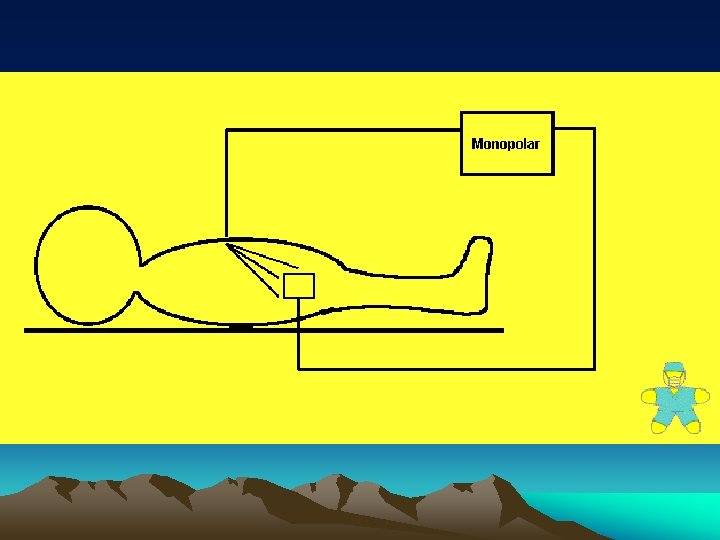
Monopolar diathermy • Electrical plate is placed on patient and acts as indifferent electrode • Current passes between instrument and indifferent electrode • As surface area of instrument is an order of magnitude less than that of the plate • Localised heating is produced at tip of instrument • Minimal heating effect produced at indifferent electrode
")
Bipolar diathermy • • Two electrodes are combined in the instrument (e. g. forceps) Current passes between tips and not through patient

Effects of diathermy • The effects of diathermy depends on the current intensity and wave-form used • Coagulation – Produced by interrupted pulses of current (50 -100 per second) – Square wave-form • Cutting – Produced by continuous current – Sinus wave-form Risk and complications • • Can interfere with pacemaker function Arcing can occur with metal instruments and implants Superficial burns if use spirit based skin preparation Diathermy burns under indifferent electrode if plate improperly applied • Channeling effects if used on viscus with narrow pedicle (e. g. penis or testis)

Lasers • Laser = Light Amplification by the Stimulated Emission of Radiation • Laser emissions are: – Collimated - parallel output beam results in little energy loss – Coherent - waves are all in phase resulting in little loss of energy – Monochromic - all of the same wave length • Effects of laser depends on photochemical, photomechanical and photothermal effects • Tissue penetration increases with wavelength • Pulsing of output can reduce thermal damage
 Pulse length Uses Carbon dioxide 10, 600 continuous")
Uses of lasers Laser Wavelength (nm) Pulse length Uses Carbon dioxide 10, 600 continuous tissue cutting Neodymium-YAG 1064 continuous coagulation Neodymium-YAG 1064 10 ns posterior capsulotomy Ruby 694 100 mss Tattoo removal Argon 488 -514 continuous coagulation Excimer 308 10 ns photorefractive keratotomy

Laser safety • Lasers are classified according to the amount of damage they can cause – Class 1 - generally safe – Class 2 - safe within the time of the blink reflex – Class 3 - cause blindness after short exposure from mirrored surfaces – Class 4 - unsafe even with reflection from nonmirrored surfaces • All medical lasers belong to class 4 • Both patients and operators require to wear goggles

Risks associated with lasers • To patient – Excessive burning – Scar formation – Visceral perforation • To the operator – Accidental skin exposure • Corneal or retinal burns

Choosing the right suture material • • Absorbable and Non-absorbable Monofilament and Multifilament Natural and synthetic Suture diameter and strength

Choice of a suture Choice of suture depends on: – Properties of suture material – Absorption rate – Handling characteristics and knotting properties – Size of suture – Type of needle
 Polyglycolic acid Catgut -----")
Synthetic monofilament Synthetic polyfilament Natural monofilament Natural polyfilament Polydioxanone (PDS) Polyglycolic acid Catgut ----- Polyglactin (Vicryl) Collagen ----- Braided Polyamide Hair Silk Polypropelene (Prolene) Polyester (Dacron) ----- Linen Stainless steel ----- Cotton Polyvinylidene ----- ----- Polybutylester --- ----- (Dexon) Polyglyconate (Maxon) Polyamide (Nylon)

Suture characteristics • Suture materials vary in their physical characteristics • Monofilament sutures (e. g. polypropylene) are smooth • The slide well in tissues but if handles inappropriately they can fracture • Multifilament sutures (e. g. polyglactin) are braided • They have a greater surface area • They are easier to handle and knot well • Some suture materials have a 'memory' (e. g. polypropylene) • Return to former shape when tension is removed

1. Catgut • Made from the submucosa of sheep gastrointestinal tract • Broken down within about a week • Chromic acid delays hydrolysis • Even so it is destroyed before many wounds have healed 2. Silk • Strong and handles well but induces strong tissue reaction • Capillarity encourages infection causing suture sinuses and abscesses 3. Vicryl • Tensile strength – 65% @ 14 days – 40% @ 21 days – 10% @ 35 days • Absorption complete by 70 days 4. Polydioxone (PDS) • Tensile strength – 70% @ 14 days – 50% @ 28 days – 14% @ 56 days • Absorption complete by 180 days
 • Hydrolysis")
Absorbable suture are broken down by either: • Proteolysis (e. g. Catgut) • Hydrolysis (e. g. Vicryl, Dexon)
 scale •")
Suture sizes • Sutures are sized by the USP (United States Pharmacopoeia) scale • The available sizes and diameters are: – – – – 6 -0 = 0. 07 mm 5 -0 = 0. 10 mm 4 -0 = 0. 15 mm 3 -0 = 0. 20 mm 2 -0 = 0. 30 mm 0 = 0. 35 mm 1 = 0. 40 mm 2 = 0. 5 mm

Surgical drains • Drains are inserted to: – Evacuate establish collections of pus, blood or other fluids (e. g. lymph) – Drain potential collections • Their use is contentious • Arguments for their use include: – Drainage of fluid removes potential sources of infection – Drains guard against further fluid collections – May allow the early detection of anastomotic leaks or haemorrhage – Leave a tract for potential collections to drain following removal • Arguments against their use include: – – Presence of a drain increases the risk of infection Damage may be caused by mechanical pressure or suction Drains may induce an anastomotic leak Most drains abdominal drains infective within 24 hours

Types of drains • Drains can be: – Open or closed – Active or passive • Drains are often made from inert silastic material • They induce minimal tissue reaction • Red rubber drains induce an intense tissue reaction allowing a tract to form • In some situations this may be useful (e. g. biliary t-tube)

Fundamental Skills Handling of Instruments, Knots by hand instruments Skin Suture Tissue Debridement Tendon Suture

Handling of Instruments

TISSUE DEBRIDEMENT • This is the most essential step in the management of the contaminated or dirty wound. • Thoroughly wash the wound with copious amounts of normal saline under pressure using either a large syringe , rubber bulb or a pulsatile lavage system. • Remove large particles of dirt with a toothed forceps. • Sharply excise [ using a No. 10 blade scalpel or sharp scissors] all slough, devitalised tissues and grossly contaminated tissues. • Wash again.

TENDON SUTURING Instruments • • • Hypodermic needles Small curved hemostat Fine non-toothed forceps Needle holder 3 -0 and 5 -0 prolene sutures Suture cutting scissors

Preparation • Match correct tendon ends using the position of the tendons & the corresponding shapes of the cut ends. • Fix tendon with a needle and steady one end with a needle. • Do not grasp tendons with any instrument as this will promote adhesions. Core Suture • Insert the 3 -0 prolene suture through the cut end of the tendon and exit through' the side at least 1 cm away from the end • Continue transversely through' the tendon and reinsert suture from the opposite side , this time to exit through' the cut end adjacent to the entry point • Repeat the above for the distal end of the tendon • Tie the ends [1 double throw and at least 4 single throws] such that the knot is buried in between the cut ends Epitendinous suture • Using 5 -0 prolene, run a simple running suture through the epitenons of the cut edges circumferentially taking care not to injure the core suture • Tie the knot at the end

Technique of tendon suture - Connell's suture

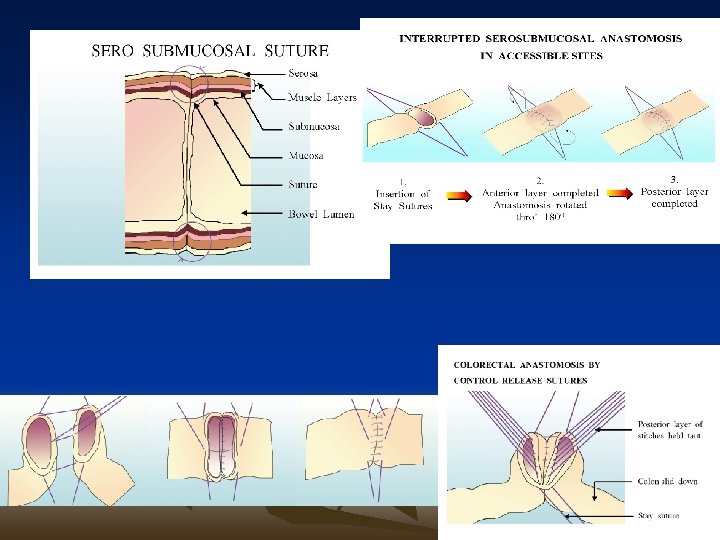
HAND SUTURED BOWEL ANASTOMOSIS BY SEROSUBMUCOSAL TECHNIQUE 1. Types • Interrupted serosubmucosal suture ( the "gold standard" for intestinal anastomosis). • Continuous serosubmucosal suture. 2. The Basis • Faster and sounder healing when compared to the traditional two layer anastomosis. 3. Advantages • Accurate tissue apposition. • Incorporates submucosa - the strongest layer. • Minimises damage to submucosal vascular plexus. • Lesser tissue strangulation. • Lesser reduction in lumen size. • Interrupted suture accommodates luminal discrepancies up to 50% without resorting to an antimesenteric slit. No 'purse string' effect even with continuous suture. • Minimises risk of implantation of neoplastic cells. • Appropriate for both upper and lower GI tract anastomosis. Continuous suture more useful in upper GI anastomoses (biliary, pancreatic). • Appropriate for both accessible and inaccessible sites. • Continuous suture is faster than interrupted suture.

Factors influencing anastomotic healing • Anastomotic technique is required to maintain apposition until collagen is laid down • Anastomoses show serosal healing and require: – Maintenance of apposition – Good blood supply – Tension free • Anastomotic leak or failure may occur if: – – – – Distal obstruction Peri-anastomotic sepsis Per-anastomotic haematoma Hypotension Hypoxia Jaundice Corticosteroids – Uraemia
- Slides: 38