The Baker Act Demystified August 5 2015 Beth

The Baker Act Demystified August 5, 2015 Beth Oberlander, LCSW

Learning Objectives Participants will gain an understanding of the following: – The scope of the Baker Act – Involuntary examination initiation and criteria – Determining if an individual meets the criteria – Parental consent, voluntary admissions, and duty to warn – What happens after an involuntary examination is initiated

What does Baker Act actually mean? • Baker Act is another name for the Florida Mental Health Act, Chapter 394, Part I, F. S. It is intended to protect the rights of all individuals examined or treated for mental illness in Florida. • It provides legal procedures for mental health examination and treatment, including voluntary admission, involuntary examination, involuntary inpatient placement, and involuntary outpatient placement. • The Baker Act also regulates crisis stabilization units (CSU’s) and short‐term residential facilities.

Involuntary Examination Initiation and Criteria

Initiation of Involuntary Examinations When a person is “Baker Acted, ” an involuntary examination is initiated and the person is taken to a receiving facility (hospital/CSU). There are three ways to initiate an involuntary examination: 1. A circuit court may enter an ex parte order stating that a person appears to meet criteria based on sworn testimony. (2% of all IE per DCF 2013) 2. A law enforcement officer (LEO) shall take a person who appears to meet criteria into custody and deliver the person or have him or her delivered to the nearest receiving facility. (49%)

Initiation of involuntary examinations 3. A licensed psychiatrist, physician, clinical psychologist, psychiatric nurse, clinical social worker, mental health counselor, or marriage and family therapist, as defined in FS 394. 455, may execute a Certificate of Professional Initiating Involuntary Examination. (49%) Licensed mental health professionals do not have a statutory duty to initiate involuntary examinations, but they may have responsibility under their code of ethics.

Involuntary examination criteria A person may be taken to a receiving facility for involuntary examination if they meet ALL of the following criteria: 1. There is reason to believe that the person has a mental illness as defined in Section 394. 455(18), F. S. (excludes retardation or developmental disabilities, intoxication, or conditions manifested only by antisocial behavior or substance abuse impairment).

Involuntary examination criteria 2. Because of his or her mental illness, the person has refused voluntary examination after conscientious explanation and disclosure of the purpose of the examination; or The person is unable to determine for himself or herself whether examination is necessary. *See definitions of expressed and informed consent vs. incompetent to consent. **

Involuntary examination criteria 3. Without care or treatment, the person is likely to suffer from neglect or refuse to care for himself or herself; such neglect or refusal poses a real and present threat of substantial harm to his or her well‐being; and it is not apparent that such harm may be avoided through the help of willing family members or friends or the provision of other services; or
 There is a substantial likelihood that without care or")
Involuntary examination criteria 3. (continued) There is a substantial likelihood that without care or treatment the person will cause serious bodily harm to himself or herself or others in the near future, as evidenced by recent behavior.
 \"Express and informed consent\" means consent voluntarily given")
Definitions of consent (re: criteria #2) "Express and informed consent" means consent voluntarily given in writing, by a competent person, after sufficient explanation and disclosure of the subject matter involved to enable the person to make a knowing and willful decision without any element of force, fraud, deceit, duress, or other form of constraint or coercion. "Incompetent to consent to treatment" means that a person's judgment is so affected by his or her mental illness that the person lacks the capacity to make a well‐ reasoned, willful, and knowing decision concerning his or her medical or mental health treatment. All minors are considered "incompetent to consent" by virtue of their age.
 Over ten years (2002‐ 11), there were increases of • 50%")
Key Statistics (DCF) Over ten years (2002‐ 11), there were increases of • 50% in involuntary exams (100, 000 to 150, 000) • 46% in individuals examined • 49% in adults examined • 35% in children examined In 2011, there were • 150, 000 involuntary exams • 111, 000 individuals examined • 93, 000 adults examined • 18, 000 children examined

But how do you know? ? Determining if an individual meets involuntary examination criteria

Neglect and self‐care issues Factors to consider: • Refusal to take prescribed medications • Refusal to eat or drink over a period of time • Large amount of expired and unused food in the home • Inability to sleep • Placing oneself in imminently dangerous situations • High risk behaviors • Neglects household, property or personal hygiene–to the point of putting self at risk

Lethality Assessment Model: WHAT • • Who does the person want to hurt? How does the person intend to cause harm? Access to method of harm? Time frame to carry out threat?

Lethality Assessment Model Who does the person intend to hurt? • If he/she is suicidal, is he/she discussing future events, i. e. next weekend? • Are threats directed at a vague group of people, i. e. “everyone”? • If the threats are directed at a specific individual/group of people, does the person have regular contact with them? If no, can the person travel easily to their location? Do they live far away?

Lethality Assessment Model How does the person intend to cause harm? • Has he/she thought of a specific plan, or is he/she making vague statements? • Is the intended method potentially lethal? Is it unrealistic, i. e. “I’m going to hold my breath”? Access • Can the person easily gain access to the means to carry out their plan? Do they have money, transportation, etc. ? • For minors, are weapons readily available in their home or neighborhood? How attentive is the primary caregiver?

Lethality Assessment Model Time Frame • Does the plan include a time frame? • Is it specific, i. e. tomorrow afternoon, or vague, i. e. “one of these days”? • Are there qualifiers in the threat regarding when it will occur, i. e. “the next time he makes me mad”?

Additional elements to assess • ELDERLY ISSUES: wanders at night, leaves things on stove unattended, unrealistic fears, uncontrollable anxiety, confusion • MOOD: feels hopeless or helpless, flat affect • A person who expresses suicidal ideation but is too depressed to put together a plan should be strongly considered for involuntary examination. • SUBSTANCE ABUSE: abuse of prescribed medications, use of alcohol or illegal substances while taking medications

Additional elements to assess • PSYCHOSIS: auditory and visual hallucinations, delusions, etc. ; reports seeing people who aren’t there, observed responding to an unseen person, hears voices telling them to harm self or others • HARM: severe cutting that warrants medical attention, recent suicidal gestures, head banging to the point of bleeding and unresponsive to prompts, previous suicide attempts, physical aggression toward others, previous CSU admissions due to HI/SI

Additional elements to assess • MEDICATION ISSUES: noncompliant or recent change in regimen, particularly for antidepressants, antipsychotic meds, and mood stabilizers • BEHAVIORS: rapid speech, flight of ideas, no eye contact, disconnected speech patterns, constantly moves or paces, can’t concentrate, mood changes quickly and frequently, disorganized thoughts, disoriented to time or place, inappropriate dress or nudity

Reasons to think twice • Does the person seem to be making up the plan while speaking to you? • Is the person romantically involved with someone currently at the CSU? • Is the person manipulative in general? • Does he/she have a pattern of making threats when angry over minor issues and calming down quickly? • Please note that while people with personality disorders can be very manipulative, they often carry out their threats; do NOT dismiss them.

The bottom line If the person is not sent to a Crisis Stabilization Unit for an involuntary examination, are you confident that the person and others will be safe?

So Now What? Initiation of an Involuntary Examination by a Licensed Mental Health Professional

The authorized professional may conduct a phone examination if the professional is sure of the person’s true identity and there is no conflict with the clinician’s professional standards.

MINORS
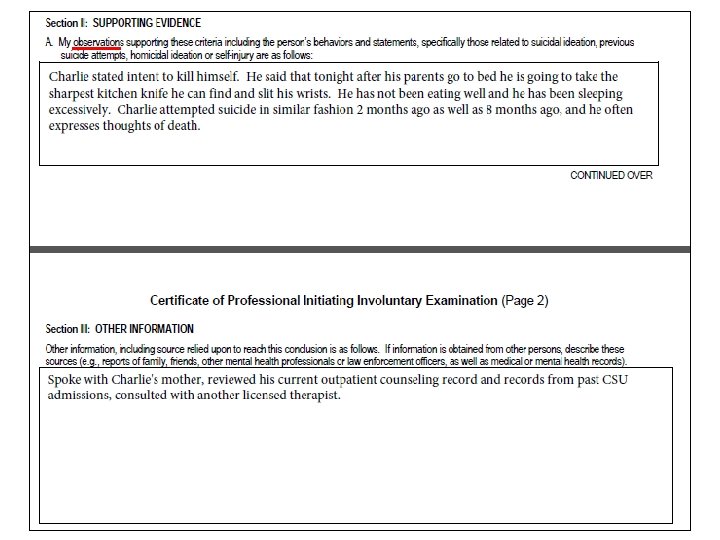

KEEP A COPY OF THIS FORM FOR THE CLIENT RECORD.

Transportation by law enforcement • Once the certificate has been completed, contact law enforcement to transport the person to the nearest receiving facility; they are required to do so by law. • If a person is arrested for a felony and the person meets involuntary examination criteria, the person will first be processed in the same manner as any other criminal suspect.

Transportation alternatives • When a member of a mental health overlay program or a mobile crisis response service, who is also a professional authorized to initiate an involuntary examination, evaluates a person and determines that transportation to a receiving facility is needed, the service may transport the person to the facility. • It is unwise to allow parents to transport minors, because the child may jump out of the car, the child may attack the parent, or the parent may opt not to take the child to the receiving facility.

Parental consent, voluntary admissions, and duty to warn

Parental consent and notification • You do not need parent permission to initiate an involuntary examination for a child or adolescent. • Chapter 394. 463 FS does not differentiate between adults and minors, nor does it mention parental consent. • Senate Bill 954, approved by Governor Scott 5/15, requires school principals/designees to immediately notify the parent of a public/charter school student who is transported to a receiving facility for involuntary examination.

Voluntary Admission of Minors • Minors cannot be legally admitted on voluntary status unless the minor’s legal guardian has applied for the admission, the minor is in agreement, and a hearing has been conducted prior to the admission. • DCF has proposed legislative changes to eliminate the requirement for a hearing, but the changes have not been approved yet. • Receiving facilities sometimes admit minors on an involuntary status and then transfer the minor to voluntary status, avoiding a voluntary “admission” (If the minor and the legal guardian agree to the admission).

Voluntary Admission of Adults • If an adult requesting admission is believed by the admission staff to be capable of providing well‐ reasoned, willful and knowing decisions about their health care, he/she may be admitted on voluntary status. Within 24 hours, a physician must confirm this capacity and certify it in the clinical record. • However, regardless of the person’s willingness to be admitted, they must be handled on an involuntary basis if they appear to be unable to make well‐reasoned decisions.

Duty to warn • Florida is a permissive state; we are not legally mandated to warn intended victims, but we are permitted to do so. • Duty to warn is an ethical mandate. • If the person continues to make threats after the initial warning, the professional should continue to warn the intended victim.

Duty to warn • A professional licensed or certified under chapter 491 may disclose confidential client information when he or she determines that there is a clear and immediate probability of physical harm to the client, to other individuals, or to society. • The professional may communicate information to the potential victim, appropriate family member, or law enforcement or other appropriate authorities. The professional is immune from liability for disclosure under this section. (491. 0147 FS)

What happens next?

Notification of involuntary examination The receiving facility must give prompt notice of the whereabouts of a patient who is being involuntarily held for examination, by telephone or in person within 24 hours after the patient’s arrival at the facility, unless the patient requests that no notification be made.

Involuntary Examination The patient shall be examined by a physician, psychiatric nurse, or clinical psychologist at the receiving facility without unnecessary delay and may, upon the order of a physician, be given emergency treatment if it is determined that such treatment is necessary for the safety of the patient or others.

After the examination Within the 72 hour time period (or by the next working day due to a weekend or holiday), one of the following must occur: • The patient shall be returned to the custody of a LEO if he or she is charged with a crime; • The patient shall be released for voluntary outpatient treatment; • The patient shall be asked to give express and informed consent to voluntary placement; or • A petition for involuntary outpatient or inpatient placement shall be filed by the facility administrator. Average length of stay is 4. 5 days per DCF 2013.

Requirements for release The patient may not be released by the receiving facility or its contractor without the documented approval of a psychiatrist or a clinical psychologist or, if the receiving facility is owned or operated by a hospital or health system, the release may also be approved by a psychiatric nurse performing within the framework of an established protocol with a psychiatrist or an attending emergency department physician with experience in the diagnosis and treatment of mental and nervous disorders and after completion of an involuntary examination.

Involuntary Placement: Criteria If a petition for involuntary placement is filed by the receiving facility with the circuit court, there must be clear and convincing evidence that the person is mentally ill and because of his or her mental illness: • He/she has refused voluntary placement or is unable to determine whether placement is necessary; and • He/she is incapable of surviving alone or with the help of others and without treatment is likely to suffer from neglect which poses a real and present threat of substantial harm to his or her well‐being; or

Involuntary Placement: Criteria • There is substantial likelihood that in the near future he/she will inflict serious bodily harm on self or other person, as evidenced by recent behavior causing, attempting, or threatening such harm; and • All available less restrictive treatment alternatives which would offer an opportunity for improvement of his or her condition have been judged to be inappropriate.

For additional information http: //myflfamilies. com/service‐ programs/mental‐health/baker‐act Forms, FAQ’s, free online training Questions? boberlander@childguidancecenter. org
- Slides: 44