The ageing skin Dr Shubhada Mandar Bichu Specialist

“The ageing skin” Dr Shubhada Mandar Bichu Specialist dermatologist Al Qassimi Hospital Sharjah

Objectives • The aging skin – How is it different? • Care of the skin in the elderly • Common skin problems in the aged

Introduction • You do not heal old age. You protect it; You promote it ; You extend it” – Sir Sterling Ross • The World Health Organization predicts that the global population of people aged over 60 years will reach two billion in 2050. • The skin is a window to ageing changes, a biological reality • Better healthcare increase in life span aging skin • “Prevention, accurate diagnoses & proper management decreased morbidity & improved Quality of Life

Why do we age? • Extrinsic ageing – Effect of sun exposure, pollutants in environment, smoking, drinking, stress. • Intrinsic ageing – Thinning of skin with loss of collagen, elastin, skin lipids leading to increased transepidermal water loss & decreased skin hydration

Skin in Elderly • Ageing is associated with structural and functional changes in the skin. Ø Ø Ø thinning of the epidermis and dermis, fragmentation of collagen and elastic fibres decreased cell healing and DNA repair. decrease in melanocytes reduced function of sebaceous glands decrease in skin lipids, vascularity and supporting structure

Hallmarks of aged skin • • • Dryness/ xerosis Laxity/ sagging Pigmented blemishes Senile purpura Sparse grey hair

• The impact of skin disease on an older patient can be both physical and psychological. • The physical impact includes pain, itching and sleep disturbance. • Psychological impact includes loss of confidence, depression and anxiety, problems with interpersonal relationships and restriction of leisure activities. • The impact on other family members, especially carers should not be underestimated.

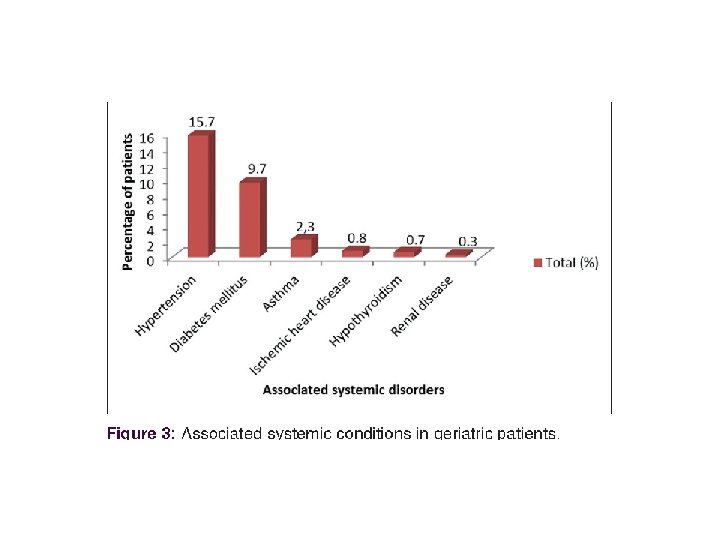
Common Skin Problems in the Elderly Pruritus is defined as an unpleasant sensation of the skin that provokes the urge to scratch Chronic pruritus represents one of the most significant challenges and is compounded by problems faced by many older people. This includes insomnia (as this increases time available for scratching), boredom and loneliness, bereavement, financial difficulties, chronic health issues and polypharmacy. Types - localised itch with or without rash and generalized itch with or without rash. Causes - Xerosis : means dry skin and by the age of 70 years nearly all adults are affected. Xerosis is the most common cause of generalised pruritus without rash in the elderly population. medication induced: A host of drugs can cause pruritus including antihypertensives, antibiotics, diuretics and psychotropic agents. Some medications induce itch by multiple mechanisms, either by provoking a primary inflammatory eruption or directly activating nerves. The mechanisms by which many drugs cause itch are unknown. In generalised pruritus without rash, underlying systemic disease accounts for up to 50% of cases. This can range from diabetes and thyroid disease to renal failure and lymphoma. Appropriate investigations to elucidate the underlying cause include full blood count, ferritin, renal and liver function, thyroid function, glucose and chest x-ray.

Dermatitis Eczematous dermatoses in the elderly include: • • Asteatotic eczema Seborrhoeic dermatitis—up to 31% of elderly patients. occurs in disproportionate numbers • • Allergic contact dermatitis—up to 11% of elderly patients (decades of potential sensitisation) Incontinence associated dermatitis-excessive moisture from urine and/or stools • Often multifactorial causes eg. venous eczema and allergic contact dermatitis to topical • • in Parkinson’s disease and central nervous system disorders. leads to overhydration and chemical irritation of the epidermis. Physical irritation (eg. cleansing) contributes to the destruction of epidermis and dermis. In addition, secondary bacterial infection is common medications and dressings. Investigations for dermatitis include swabs for microbiology and skin scrape for mycology (especially unilateral distribution). An HIV test in extensive or refractory seborrhoeic dermatitis should be considered.

• • • Patients should be referred for patch testing if allergic contact dermatitis is suspected. Referral should also be made when acute or chronic eczema is not responding or aggravated by treatment or there is an unusual distribution/pattern. Venous eczema and eyelid eczema should be seen by a specialist. A skin biopsy should be conducted for suspected eczematous drug eruptions. Emollients combined with humectants (eg. urea) are the best strategy for treating xerosis in older patients. For preventing skin injuries the use of soap substitutes and non-detergent cleansers can reduce the incidence of skin tears and incontinence associated dermatitis. Skin protecting effects might be enhanced when barrier products are additionally applied. In a study, the occlusive agent dimethicone was most often reported for incontinence associated dermatitis and skin-tear prevention. 2 Recommended management for both pruritus and eczematous dermatoses is therefore emollients (preferably ointment containing urea) and soap substitutes. Bathing in tepid water for 10 minutes enables the stratum corneum to absorb water and the patient should moisturise immediately after. For active eczematous areas, a mild/moderate potency topical steroid should be used on the face once daily for two weeks then 1 -2 times weekly as maintenance. Whereas a moderate potency topical steroid can be used on the body once daily for two weeks then 1 -2 times weekly as maintenance. Secondary bacterial infections should be treated with appropriate antibiotics. Patients should be referred for patch testing and compression for venous eczema if appropriate. Second and third line treatments include phototherapy and systemic treatments such as methotrexate, mycophenolate and ciclosporin. Management of seborrhoeic dermatitis includes 2% ketoconazole shampoo to the scalp (and skin) twice weekly for four weeks, then once weekly as maintenance. A de-scaling shampoo, containing coconut oil or salicylic acid and a topical steroid can also be applied to the scalp (preferably mousse, lotion or shampoo) once daily for two weeks then twice weekly as maintenance. In addition, a mild topical steroid that contains an antifungal agent can be used. Itraconazole 200 mg od for 14 days can also be considered for refractory cases.

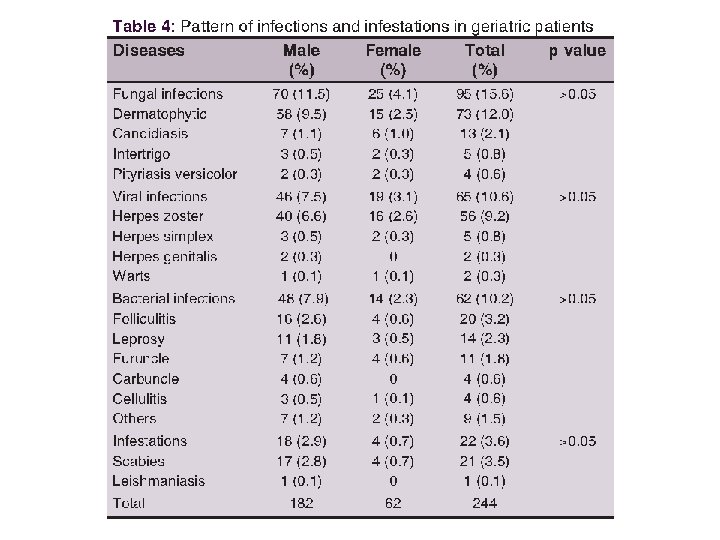
Skin infections • Can be bacterial, viral or fungal • Diabetics are more prone • Fungal infections are the commonest. Candidal and dermatophyte infections flourish in moist areas like the flexures, interdigital and diaper areas. Prevalence of fungal nail infections also increases with age. Keeping the involved parts dry, use of zinc oxide creams in diaper areas help in prevention. Use of appropriate antifungal creams and powders help in control. • Bacterial infections may appear atypical in the elderly. Most common are cellulitis and infected ulcers. Prompt treatment and drainage of abcesses/debridement of ulcers is essential • Viral infections such as herpes zoster with post herpectic neuralgia occurs more commonly in the elderly due to decreased cell mediated immunity

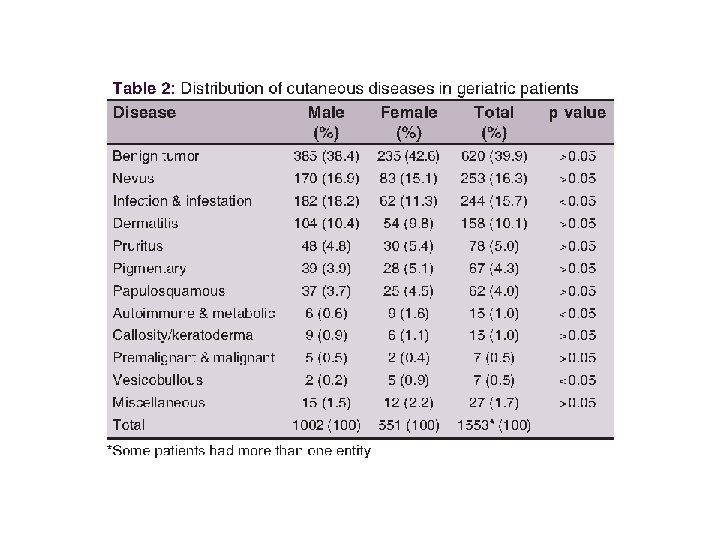
Benign Skin Tumors • Elevations and Discolorations of the Skin Ø Age spots (liver spots, lentigos) appear most often on areas of skin likely to get UV exposure such as the face, shoulders, forearms, and back of the hands Ø Moles (nevi) and atypical moles (dysplastic nevi): Ø Seborrheic keratoses: Ø Acrochordons (skin tags): Ø Cherry angiomas:

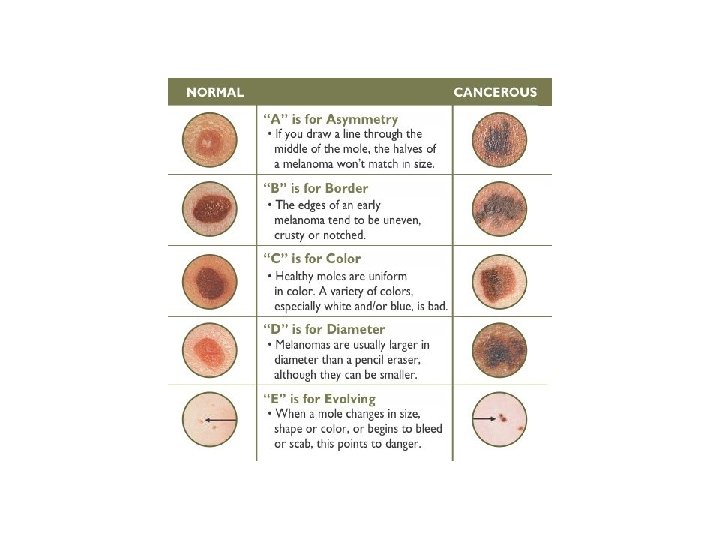
Malignant Skin Tumors • • • Surgical excision is the only curative treatment for melanoma. Risk factors are fair skin, freckles, blue or green eyes, red or blonde hair, increased number of moles (>100), immunosuppression, family history, sunbeds and UVR exposure with a history of severe sunburn in early life. Other red flags in patients are the sudden appearance of new moles— 80% of melanomas occur de novo rather than within pre-existing moles and changes in an existing mole eg. growing rapidly, changing shape or colour, itching or bleeding. The ABCDE and the “ugly duckling” methods can be used to differentiate a suspect lesion from an ordinary mole. ABCDE stands for Asymmetry, Border, Colour and Diameter and Evolution. An ugly duckling is when a lesion appears different to the rest on a person’s skin. Acral melanoma is melanoma arising on the soles or palms and within the nail unit. It can be difficult to recognise so delays occur in diagnosis. A history of trauma should not exclude the possibility of a melanoma as evidence suggests many cases of melanoma are brought to the attention of the patient by co-incidental trauma and injury. They can occur in all ethnic groups and skin types. Squamous cell carcinoma can present as a thickened red scaly spot that may bleed, or a nonhealing lesion, and it is often painful. It develops on chronically sun-exposed sites such as the face, hands, forearms. High risk squamous cell carcinomas occur on ears and lips and anything over 2 cm has a higher risk of metastasising. Basal cell carcinoma is the most common and least dangerous form of skin cancer. It is a red or pale pearly lump or scaly dry area and is usually a non-healing lesion.

To Conclude • • In summary, ageing is associated with structural and functional changes in the skin that render it more susceptible to skin disease. Xerosis is the most common disorder in aged skin. Elderly patients are also more prone to skin infections and skin malignancy incidence is increasing. There should be a full dermatological examination in admitted elderly patients looking for undiagnosed dermatoses, infections, skin cancers and manifestations of underlying systemic diseases. In affected patients, emollients and soap substitutes should be prescribed as standard and as basic treatment for pruritus, prevention of xerosis and skin injury. An appropriate topical formulation will aid compliance. A maintenance regime in inflammatory dermatoses following an initial course of topical steroid also helps to break the itch/scratch cycle and reduce frequency of flares. Key recommendations are to consider allergic contact dermatitis in refractory disease and dermatitis with an unusual distribution or patients with atopic dermatitis; to consider secondary bacterial infection in refractory disease; to look out for skin malignancies and refer promptly to a dermatologist and consider malignancy as a cause of non-healing lesions.
- Slides: 18