The Affordable Care Act and Beyond Objectives of

“The Affordable Care Act, and Beyond” Objectives of the presentation: 1. Review the core features of the ACA (“Obamacare”) 2. Answer the question: Will the ACA achieve its goals of universal and affordable care? 3. Stimulate a discussion: What else is needed to make our healthcare equitable and sustainable? Chinh T Le, MD April 24, 2014

National Academy of Sciences - Institute of Medicine September 2012 Report “The past 50 years have seen an explosion in biomedical knowledge, dramatic innovation in therapies and surgical procedures, and management of conditions that previously were fatal. Yet, American healthcare is failing short on basic dimensions of quality, outcomes, costs and equity. ”

“Shorter Lives, Poorer Health” A “must-read” for all: • politicians who claim that “the US have the best health care in the world” • Health policy makers • Social scientists (http: //www. nap. edu/catalog. php? record_ id=13497)
")
(Source: The Lancet Commissions on Global Health – March 2014)

Controlling costs does not mean a decrease in quality. On the contrary… • Most US health outcomes, when measured, are below the average of other OECD countries. • A saving of $ US 500 billion/year (or 20% of US healthcare expenditures) can be achieved if the quality of the US health care is brought up to the average of other OECD countries (Source: Stefan Larsson, Nov 2013)

National Academy of Sciences Institute of Medicine – 2004 recommendations Health care coverage should be: 1. 2. 3. 4. 5. Universal Continuous Affordable to individuals and families Affordable and sustainable to society Promoting access to high-quality care that is effective, efficient, safe, timely, patientcentered, and equitable

Five interdependent principles and goals for a reformed health care system • • • Health care coverage for all Cost containment Improvement of health care quality and safety Equitable funding Simplified administration “Health care reform must be a national priority, must be system-wide, not partial nor piece meal”. (National Coalition on Health Care, 2004) www. nchc. org

Understanding healthcare dynamics and finances Funding Public and private Insuran ce structur e Payments to providers and suppliers Delivery of services

Roots of current healthcare problems in the US Insuranc e structur e Provider reimbursement Fee-for-service: No transparency, No accountability divides populati on into inequitab le “categori es” Delivery of services: Provider-centered, fragmented, uncoordinated and inefficient

Health insurance coverage – US population 2011 -12 Uninsured 15% Military, VA 1% Employerbased 48% Medicare 14% Medicaid 16% Other private 5% (Source: US Census, 2013)

The ACA and Medicare • Leave the insurance structure intact • Test new models in payment and service delivery to lower costs and improve quality: –Create Accountable Care Organizations (ACO) –Enter into a partnership with State and multiple private insurance systems to make changes possible • Create an Independent Payment Advisory Board to recommend to Congress payment to providers and suppliers, replacing the current “SGR=sustainable growth rate” • Expand drug coverage • Attempt to cut 14% subsidy to MC Advantage plans unsuccessful so far

Accountable Care Organizations • Assume responsibility for a defined population of patients across a continuum of coordinated care • Are held accountable through payments linked to value (saving) and performance measurements (quality) • But create a danger of consolidation and market monopoly Oregon CCOs (for OHP) “Medical Home” model

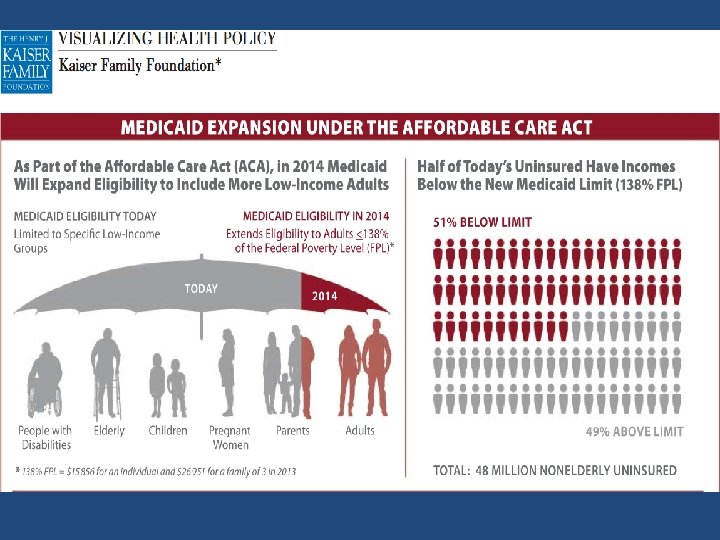
The ACA and Medicaid • Expansion: – initially funded by the federal government, with States gradually taking more financial responsibility – Subject to State co-operation
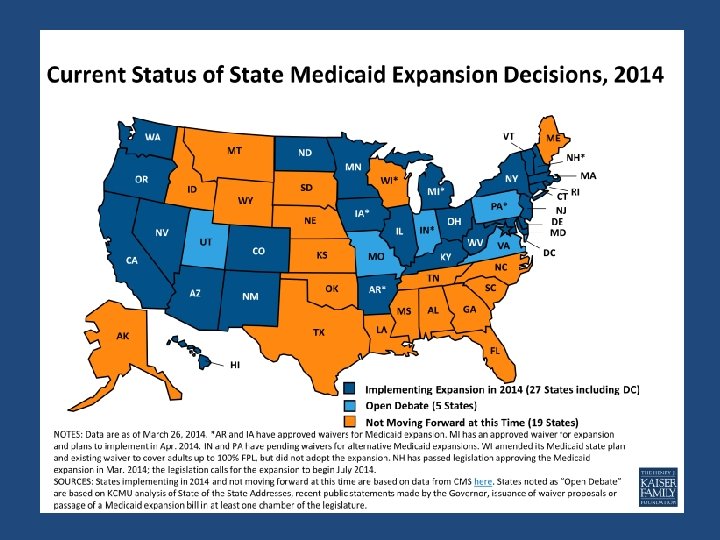

Failure to expand Medicaid

Who does the Affordable Care Act leave behind? 19 million 6. 3 million (Source: RAND Corp. March 2014) 5. 3 million in 23 states

The ACA and the private insurance market • Keep employer-based model • Create “exchange markets” to “shop, choose and buy” insurance plans • Income-based tax credits to buy insurance • “Mandate” insurance , or pay penalty

For those using private insurance plans, the ACA offers significant consumer-friendly clauses: • Bans insurance denial for pre-existing conditions • Bans cancellation after illness or injury occurs • Limits maximum deductible • Bans lifetime limit for essential benefits • Mandates dependent coverage until age 26 • Limits insurance administrative & marketing costs and corporate profits to 20% (“Minimum Medical Loss Ratio” rule) • Requires large employers to offer insurance or pay a penalty

Health Insurance Exchanges • Goal: Make it “easier” for small businesses and individuals to buy “qualified” private health insurance coverage, promote competition among health insurers • Qualifications: Plans must offer 10 “essential benefits” • Process: “on line shopping” : side-by-side comparison of various insurance plans to choose what fits you best • Affordability: Use premium tax-credit for families with incomes between 138 -400% of FPL, and for small businesses

Essential Benefits for inclusion in ACA Insurance Exchange Market 1. 2. 3. 4. 5. Ambulatory patient services Emergency services Hospitalization Maternity and newborn care Mental health and substance abuse disorder services, including behavioral health treatment 6. Prescription drugs 7. Rehabilitative and habilitative services and devices 8. Laboratory services 9. Preventive and wellness services 10. Pediatric services, including oral and vision care
")
The problem with the “exchange markets”: Easier said than done (NY Times cartons, 04/2014)
 … it’s")
“If you like your healthcare plan, you can keep it” (Obama, 2010) … it’s a bit like saying: “If you like your husband, I promise he won’t cheat on you or divorce you…” (The Economist, Jan 26, 2013)

In summary, Obamacare Funding Public and private Insuran ce structur e basically unchan ged Test new models of Payment to providers Test new models of health service delivery

Beyond dealing with insurance structure, Obamacare offers an unprecedented opportunity to: 1. reform health delivery and payment system Patient-centered; transparent and accountable, and value-driven (so far, easier said than done…) and 2. improve population health Public health interventions Disease prevention Comparative effectiveness research Health equity

Value-based health care Source: Stefan Larsson, MD in Ted Talk, Nov 2013: “What doctors can learn from each other” http: //www. ted. com/talks/stefan_larsson_what_doctors_can_learn_from_each_other. html

Return on investment Looking at “value-based” cost-benefits of health interventions Clinical management Public health measures $ $$ $$$$

New GOP proposals in health care reform • 1. Medicare: Voucher system • 2. Medicaid: change to a block-grant program; open to private insurance plans with low premium, high deductible and high out of pocket expenses • 3. Other issues: – Keep many of the popular benefits enacted under the ACA, but make them not mandatory and much weaker. – Keep employer-based private insurance and tax-credit subsidies, but at lower levels; premiums can be based on health status and gender. – Repeal individual mandate; states can “auto-enroll” eligible individuals. Source: NEJM, Feb 2014 –Sen. Hatch (UT), Coburn (OK) and Burr (NC)
 Medicare beneficiaries will have more")
Under the GOP “voucher” system (i. e. “premium support”) Medicare beneficiaries will have more out-of pocket expenses

Will Obamacare fulfill the 5 core principles advanced by the IOM and National Coalition on Healthcare ? Principles Obamacare: initial evaluation Universal coverage No - Many obstacles remain; vary by states Continuous coverage Not for everyone - Gaps lessened, but “churning” of plans likely. Choice of providers limited by health networks Cost is a moving target, varies widely. Overall cost control not yet proven Affordable to individuals, families and society High-quality and equitable Remains to be seen care Effective, efficient simplify No - susceptible to volatile private administration market

ACA limitations Obamacare Because of it is built on faulty foundations: • Is a complex, confusing and unstable system for patients and providers, and 1. • Will continue to drive high administrative costs • Probably will not solve problems of healthcare inequities and financial insecurity due to highdeductible plans Americans continue to receive health insurance depending on what “categories” they belong to, and 2. The free-market, profitdriven model is intrinsically volatile and encourage rent-seeking by suppliers and providers

Beyond Obamacare: The long and winding road 1. Identifying major obstacles: – Ideological divide: Private vs. public control Who do you trust the most? Corporations or Government ? – Power of special interest groups: • Lack of transparency • Cost-shifting and waste • Rent-seeking – the “legalized” form of corruption

Lack of transparency encourages cost-shifting and waste: In the US , this amounts to $750 billion a year, or 30 c of every medical dollar • • • Unnecessary services (overtreatment) Inefficient delivery of care Excessive administrative costs Inflated prices Prevention failures Fraud $210 B $130 B $190 B $105 B $ 55 B $ 75 B (Source: National Academy of Sciences - Institute of Medicine, September 2012 report)

“Rent-seeking” • Refers to activities that reap extra profits by re-writing the rules • Usually driven by “big money” rather than political ideologies • Examples in health care: This is the ultimate – Lobbyists help write laws that prohibit fraud, a “legalized” Medicare from getting discounts from corruption that bulk-purchasing, or from purchasing maintains a forcheaper therapeutic equivalents; IP profit healthcare laws that give rich payday to drug system, runaway manufacturers costs, and health – Industry-funded researchers write clinical guidelines that encourage over inequity -diagnosis and over-treatment

$ Billions spent since 1998 on lobbying Washington • Defense and aerospace contractors • Oil and gas companies • Health care organizations (Source: Time magazine, Feb 26, 2013) 1. 53 1. 3 5. 36

State Report Card on Healthcare Price Transparency Laws Scores: Blue= 60 -100%; …; F= 0 -30% Source: Catalyst for Payment Reform and Health Care Incentives Improvement Institute, March 2013

Beyond Obamacare: The long and winding road 2. What further steps, and/or new directions do we need to take in our healthcare reform? 3. How will we move forward? (Possible topics for afternoon discussion groups…)

Universal, publicly funded health insurance Advantages: Universal coverage Lower administrative costs Equitable benefit package Negotiate competitive purchasing of drugs and equipment ü Organized planning and sharing of major capital expenditures ü ü Social Value: Access to health care for all is a shared community responsibility and benefit. Opponents fear: “Big Government bureaucracy” Ø Anti-free market? Ø More taxes? Ø Less choices: rationing? Ø Less autonomy for providers? Ø Abuses and fraud? Social Value: Does not promote “individual responsibility and ownership” of health care decisions

We accept the role of government in providing safety and enhancing quality of life for everyone Schools Roads & Bridges Firemen Libraries Police National Parks Why not “Medicare For All”

“Mankind made a big mistake when it allowed the practice of medicine and the profit motive to intertwine. ” George Bernard Shaw (1856 -1950)

In a political discussion, it never helps to take a morally superior tone to one’s opponent Nelson Mandela (in “Long Walk to Freedom”)

Choices, social values, and “rationing” in health care “Medicine is a social science in its very bone and marrow” (1847) Solomon Newman, German physician (1819 -1908) “Most ethical dilemmas are not the result of conflicts between right and wrong, or good and evil, but result from conflicts between competing goods” Cliff Hall, Corvallis physician, January 13, 2012

“First, determine what is the right thing to do. Then, find the way to do it. ” right Abraham Lincoln (1809 -1865)


- Slides: 45