THE ABORIGINAL AND TORRES STRAIT ISLANDER HEALTH NARRATIVE

THE ABORIGINAL AND TORRES STRAIT ISLANDER HEALTH NARRATIVE – EPIGENETICS AND EARLY CHILDHOOD TODAYS CHILDREN – TOMORROWS FUTURE EARLY CHILDHOOD CONFERENCE 2015 DR MARK WENITONG SENIOR MEDICAL ADVISOR APUNIPIMA CAPE YORK HEALTH COUNCIL ASSOCIATE PROF (ADJUNCT) JCU

NACCHO DEFINITION OF HEALTH AND WELLBEING – CONTEXT OF EARLY YEARS …not just the physical well-being of an individual but refers to the social, emotional and cultural well-being of the whole Community in which each individual is able to achieve their full potential as a human being, thereby bringing about the total well-being of their Community…. . …While we work with individuals for Aboriginal and Torres Strait Islander’s, its always about family and community…

Indigenous life expectancy for 2013 AIHW Future - While the Australian health system is gearing up for the aging population we are looking at a much younger population with increased middle age = CD Life Expectancy - National • 69. 1 years for males (10. 6 years lower) • 73. 7 years for females (9. 5 years lower ) 75% Aboriginal and Torres Strait Islander die before 65 yrs, 25% non Aboriginal and Torres Strait Islander before 65 yrs Cape York median Age at Death 52 males, 56 females (Qld non Indigenous 76 males, 82 females – Health Indicators Cape York 2009, QH) SMR CY 2010 : 1. 9 (all cause mortality)

QUEENSLAND Age Structure: Ref - The burden of disease and injury in Qld Aboriginal and Torres Strait Islander people 2014 QH

POPULATION RICHARD CINCCOTTA DEMOGRAPHICS

INFLUENCES INDIGENOUS In utero environment / genetics / epigenetics / FASD Early life experiences and adult behaviour Environment, safety, community/family functioning Early relationships, adaptive/maladaptive responses Access to quality early childhood programs, education, health Poverty, nutrition, access, neuro-cognitive development Cultural influences, program acceptability

HOUSEHOLD COMPOSITION REF - AIHW 2015 • In 2011, Indigenous households comprised an average of 3. 3 people compared with 2. 6 people in other households. • 21% Indigenous households were a one-parent family with dependent children in 2011 compared with 6% of other households.

CARERS VALUES

STATS AIHW 2015 Aboriginal and Torres Strait Islander children aged 0– 14 years died at more than twice the rate of non-Indigenous children. • Indigenous aged 5– 14 years, external causes was leading cause of death at 3 times the rate for non‑Indigenous children. • The hospitalisation rate for assault on Indigenous children was more than 5 times the rate for non-Indigenous children. • Indigenous children were hospitalised for burns and scalds at twice the rate of other children. • The pneumonia hospitalisation rate for Indigenous aged 0– 4 years was more than 3 times the rate. • Nearly 12% of Indigenous children who received a Child Health Check had chronic otitis media—more than 3 times the rate the World Health Organization classes as epidemic. Hence, easy to see why it’s a deficit approach to an Aboriginal and Torres Strait Islander early childhood narrative. •

UNPACKING CAUSATION- AND PERSONAL AGENCY – BOTH IMP ( BAKER IDI BROWN, ADAPTED WENITONG 2014) Policy perspective - adult Social and developmental health perspective – early childhood Bad health behaviours Allostatic Load Adverse childhood events Developmental neurobiology Bad choices Social determinants, ACE, Poverty trap Lazy ACE, lack of infrastructure/employment Trauma, loss of control, depression, poverty trap Fat Poor access to good nutrition, epigenetics, poverty trap, depression, ACE Abbot: Get some Nikes and go for a run Me: Get some decent board-shorts mate. 2 -3% of the population make up 10% of the elite sportspeople – there is personal agency

BIOLOGICAL – ANC EPIGENETICS IMPLICATIONS • Eg poor maternal nutrition/stress pulls switches re histone modification, RNA methylation to influence physical expression so that baby is physiologically set up for famine conditions when born and central fat storage as adult. (is heritable across next generation) • Rethink patient narrative re adult risk behavior without losing sense of agency • Policy implications of political ideology are where resources are invested

MICROBIOME Involved in regulation of obesity, metabolic syndrome, inflammation………fecal transplants…. 11 yr olds T 2 D
")
PHYSIOLOGICAL - ALLOSTATIC LOAD (REF- MCEWAN)

ACE - ADVERSE CHILDHOOD EXPERIENCES – REF- FELLETTI - CENTERS FOR DISEASE CONTROL WEBSITE This study compared people who had experienced four or more categories of childhood exposure including physiological, physical, and sexual abuse, or household dysfunction with those who had experienced none. • It found a 4 -12 x increased health risk for alcoholism, drug abuse, depression, and suicide attempt; • A 2 -4 x increase in smoking, poor self- rated health, and increased chance of 50 or more sexual intercourse partners and sexually transmitted disease. In addition, they had a 1. 4 to 1. 6 -fold increase in physical inactivity and severe obesity. (Felitti 1998) WANGETTI school screen • 60% children between 13 -18 had significant adverse experiences – none had an intervention – though interventions can modify later outcomes •

WA ABORIGINAL CHILD HEALTH SURVEY Primary carers of Aboriginal children reported extraordinary levels of stress. • Over one in five (22%) Aboriginal children aged 0– 17 years were living in families where 7– 14 major life stress events had occurred over the preceding 12 months. • Primary carers of Aboriginal children experienced over three times the average number of life stress events reported by carers of non. Aboriginal children in the 1993 WA CHS.

FOOT PRINTS IN TIME Longitudinal study of Aboriginal and Torres Strait Islander children Wave 4 results – key stressor scores: - household member in trouble with police - cared for by someone other than usual carer - scared by some-ones behaviour Less high scores - housing events, money worries, drug/alcohol problems in family, harassed Consider in context of current policy and assumed stressors Ref- https: //www. dss. gov. au/about-the-department/national-centre-for-longitudinalstudies/overview-of-footprints-in-time-the-longitudinal-study-of-indigenous-children-lsic
 found that children in the Western Australian Aboriginal Child")
WAACHS Zubrick and colleagues (2005) found that children in the Western Australian Aboriginal Child Health Survey (WAACHS) who had experienced up to two major life events during the previous twelve months had a 15 per cent chance of developing clinically significant social and emotional difficulties. This rose to 25 per cent for children who had experienced three to six major life events and: 42 per cent for children who had experienced seven or more.

FIGURE 11: EXPERIENCE OF THREE OR MORE EVENTS BY NUMBER OF WAVES, PER CENT

WAVE 4 https: //www. dss. gov. au/about-the-department/national-centre-forlongitudinal-studies/overview-of-footprints-in-time-the-longitudinal-study-of -indigenous-children-lsic

POVERTY THINKING I started out with nuthin…and still got plenty left… • NATSIS ABS – income significantly less urban/remote (inc mining areas) • Duflo (economist) – interaction between Hope, poverty, mental health. • David Campbell - Economic Rationality in Choosing between Short-Term Bad-Health Choices and Longer-Term Good-Health Choices • The difference between having only enough to survive, versus having enough to apply to your capabilities…….
 bad choices, poor nutrition, tobacco, alcohol misuse (SNAP)")
Issue Etiology Adult CD mortality (SNAP) bad choices, poor nutrition, tobacco, alcohol misuse (SNAP) Developmental etiology - ACE, epigenetics, microbiome, family functioning, neglect, normalized behavior, allostatic load Economic - poverty choices, Infrastructural support, health access, non healthy environment. Bad choices, risk factors Poor family functioning, neglect, Relative poverty (trap), lack of employment, stressors, Indigenous specific – systematic (as above) at “Peoples” level, intercultural space, lack of infrastructure, lack of investment Community dysfunction/poverty Indigenous specific – Systematically socially marginalized, economically marginalized, young demography, poorly conceived policy, political drivers. Lack of control. Fast modernisation Aim at rebuilding social fabric, self determining, community structures, not quick fix programs, Capability, DRIP, re- Marginalization historical/contemporary

MASLOW HIERARCHY OF NEEDS - BACK TO BASICS

MY CHILDREN’S HIERARCHY OF NEED

FATHERS? Who has the largest influence on safe Aboriginal and Torres Strait Islander communities? • • • Engaging dads Family protector role Conscript re smoking/alcohol reductions Paternal role Teaching young men/culture/law/ID ( Ref – Apunipima Cape York Health Council program)
 • Spend more time")
DRIVERS FOR DADS Yarrabah Men’s Group (NHMRC PAR, TSEY, K) • Spend more time with the kids • Don’t argue in front of kids • Teach your kids to read • …… Cape York MJ Survey (Clough JCU) Main reason for stopping gunja – • Family role model • Employment • Cost

SATISFIED CARERS?

TABLE - WENITONG 2015 Sen Capability Framework – sociopolitical structures Definition – relevant Present/not present in Declaration of the Rights remote indigenous of Indigenous Peoples communities Political Freedoms Freedom of political expression, voting… DRIP 23/24/18/20 √ but called “Activist” Voting post ‘ 67 Economic facilities Opportunities to utilise economic resources. . DRIP 26/32 × Mostly Lacking long term investment/ serious reform Social Opportunities Education, healthcare… DRIP 14/24/34 × limited opportunities Transparency guarantees Openness in dealings with × often not included in others…. policy that effects them DRIP 27/19 Protective security Safety net to prevent abject poverty…. DRIP 7 × welfare threshold for basic living – but poverty trap

EMPOWERMENT APPROACHES FROM A CLINICIANS POINT OF VIEW o Critical consciousness – not passive acceptance o From political consciousness to taking better selfcare/individual health – FWB CY o ANFPP, self mx, Bo. P, all examples o Community control o Ability to envisage a positive future

SOCIAL DETERMINANTS Control Environment wellness Employment Income discrepancy

INDIGENOUS DETERMINANTS? Body Spirit wellness Land Relationships
")
CULTURAL CONTINUITY FACTORS ( CHANDLER, LALONDE)

CULTURAL CONTINUITY

APUNIPIMA MATERNAL AND CHILD HEALTH 2014 -15 DATA - INC B 0 P “BABY ONE PROGRAM” • 100% of pregnant women received 5 or more AN consultations/ visits (av 13. 8) during pregnancy as per national recommended best practice ( was 83% 2011 QH) • 50% of women accessed AN care before 13/40 • 31% of the pregnant women also received a comprehensive adult health check ( in addition to routine AN care) • 53% of pregnant women identified as smokers( down from 72% in previous year) • 80% of babies born were within normal weight range • 90% of Cape York babies were born after 36/40 • 78% of babies were recorded as still breast feeding at 6 months • 95% of children under 5, were recorded as fully immunised ( national average: 88%) • Over 1685 home visits conducted

BABY ONE HV Parenting education sessions include health worker led: • • • DV Nutrition Home safety Alcohol and gunja Speech and language Normal development

US NURSE LED HV - NY STUDY: CHILD OUTCOME Notified Abuse / Neglect 0 – 2 yrs Control Group = 19% Intervention Group = 4% p = 0. 07

NY STUDY: CHILD OUTCOME AT 2 -4 YRS No Treatment Effect - Child abuse and neglect (but, ↓ seriousness of abuse) - Children intellectual functioning Positive Treatment Effect - Home hazards - Injuries and ingestions (40% ↓) - Behavioural and parental coping problems (45% ↓) - Emergency Department visits (35% ↓) - Maternal involvement with child - Punishment (increase)

NY STUDY: MATERNAL OUTCOMES AT 15 YRS • • Verified child abuse/neglect Unmarried, low SE status - Subsequent births - Interval to 2 nd child - Receiving Welfare - Behavioural impairment due to alcohol and drugs - Arrests Intervention 0. 29 Control 0. 54 p<. 001 1. 3 65 m 60 m 1. 6 37 m 90 m p = 0. 02 p =0. 001 p =. 005 0. 41 0. 16 0. 73 0. 90 p =0. 03 p<0. 001

NY STUDY: CHILD OUTCOMES, 15 YRS Intervention • • Running away Arrest Convictions Lifetime sex partners Cigarette / day Alcohol days in 6 m Drug related behaviour problems Control 0. 24 0. 20 0. 09 0. 92 1. 50 1. 09 0. 60 0. 45 0. 47 2. 48 2. 50 2. 49 p = 0. 003 p = 0. 03 p < 0. 001 p = 0. 003 0. 15 0. 34 p = 0. 08 p = 0. 03
 •")
PHC INTERVENTIONS • Epigenetics – EB Maternal care programs ( NHVP, Bo. P) • EB programs - Family functioning and early childhood environment, learning, nutrition – MCH, parenting, early intervention, ANFPP, ABCedenarian, Bo. P, HIPPY, • Articulating programs – eg FASD (> 20 orgs) • • Addressing the stressors in carers – police, bereavement. Paternal programs – engaging dads Cultural Continuity – community empowerment…EC • More research – RCT – what does actually work? •

BUILDING RESILIENCE TELETHON CHILD HEALTH

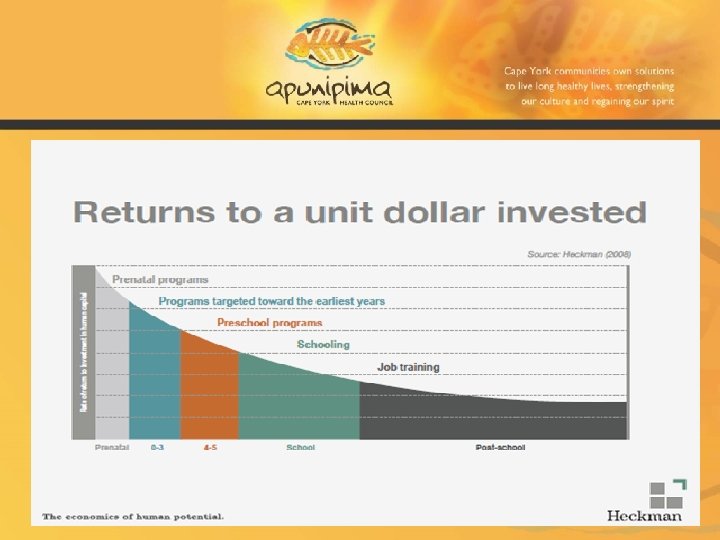
CUNHA & HECKMAN

WHY THE “EARLY CHILDHOOD NARRATIVE” IS IMPORTANT • • The narrative describes the EB for intervention and change- if we neglect it, its ground hog day for Aboriginal and Torres Strait Islander people If we have an understanding of the key drivers of poor adult health/health behaviour we can intervene appropriately/early. • Both individual and community level interventions are needed, but we have enough evidence to “just do it”. • National policy can invest wisely in EB early childhood programs • There are multiple positive Aboriginal and Torres Strait Islander family influences we can build on. • We need to better articulate how we all work together across portfolios etc. Health and welfare, public health, social scientists, educationalists, Aboriginal and Torres Strait Islander people and researchers provide a consistent backbone to drive this agenda as politicians/policy changes
- Slides: 43