TH 4 INTERNATIONAL TOXICOLOGICAL CONFERENCE Dr P Sampath





























- Slides: 33
TH 4 INTERNATIONAL TOXICOLOGICAL CONFERENCE
Dr. P. Sampath Kumar Professor & Police Surgeon Head of Department of Forensic Medicine & Toxicology Sri Ramachandra Medical College & RI Vice Principal , Sri Ramachandra University, Chennai, India
PRINCIPLES OF MANAGEMENT IN A CASE OF MULTIDRUG OVERDOSE
INTRODUCTION: �Alcohol interacts with a number of drugs thereby resulting in adverse health effects for the drinker. �Alteration can occur either in the metabolism or effects of alcohol and/or the medication. �Alcohol and drug interaction can be of two types Pharmacokinetic interaction Pharmacodynamic interaction
�Antihypertensive drugs constitute leading form of cardiovascular drug overdose �Implicated in 48% deaths resulting from such overdose �Most common among these- Calcium channel blockers and Beta blockers �Treating patients with such overdose can be a challenge for even experienced physicians
College student- quarrels at home Consumes ethyl alcohol Comes home and takes 20 -25 antihypertensive tablets
Gets up at midnight with severe headache Takes few tablets of aspirin for relief from headache Stays awake for the next two hours after which he falls asleep again
Next day morning family leaves for a function leaving the boy at home Boy gets up , manages to reach the college Friends find him drowsy and unable to walk Narrates the incident to them
Wheel him into the casualty of a tertiary care hospital Medical officer seeing him in a wheelchair delays attending to him, thinking its not an emergency Collapses in the wheeler, on examining pulse feeble, BP not recordable
Intubated – put on ventilator, I. V line secured and fluids ionotropes started Grave prognosis explained to the relatives Other investigations were conducted Despite the fluid management and ionotropes , his urine output was nil.
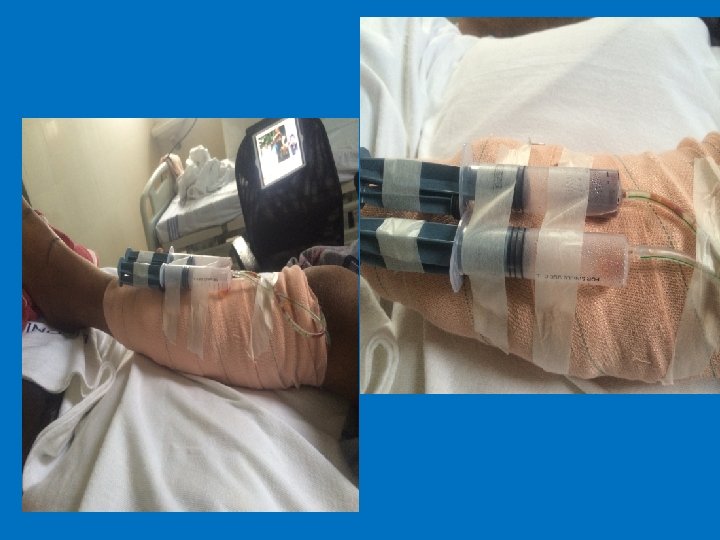
Intensivist suggested to start ECMO Shifted to MDCCU Specific antidotes were given in the MDCCU After about half an hour , 15 ml of urine is collected After 3 days of ECMO, boy regains consciousness
However he developed swelling and immobility of the leg in which catheter was placed Investigations revealed- leg ischemia, that would have necessitated amputation However appropriate management by a plastic surgeon in a rural centre saved the boy, his leg.
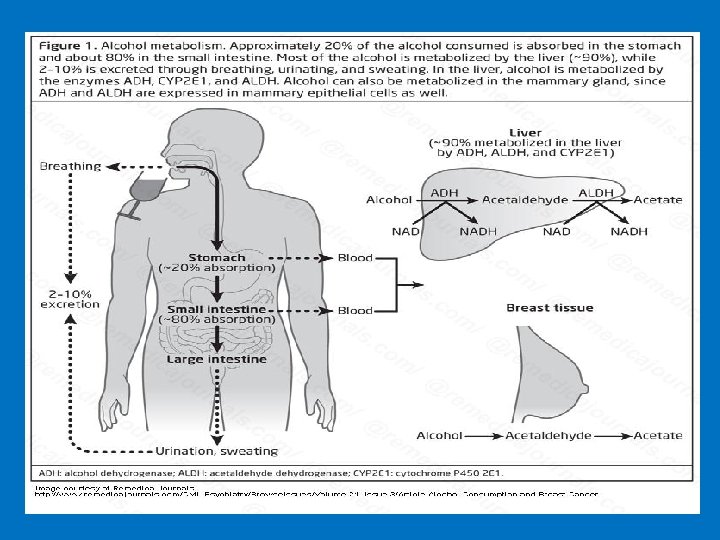
DISCUSSION �Alcohol & a number of medications interact with each other resulting in potentially serious medical consequences. �Interactions alter A)the metabolism or activity of the medication B)alcohol metabolism.
� Medications and alcohol compete in the body for absorption potency of the medication and/or alcohol is often increased/ decreased. �No set formula �Each person is different �Results of this type of potentially fatal cocktail vary based on ü type and quantity of medication and alcohol ingested ü the time frame involved ü individual's tolerance (medication/alcohol)
�Studies focus on the effects of chronic heavy drinking. �Relatively limited information available on medication interactions resulting from moderate alcohol consumption
ALCOHOL AND CARDIAC DRUGS ALCOHOL ANTIHYPERTENSIVE DRUGS üprofound hypotension ü refractory bradycardia ü cardiogenic or non cardiogenic pulmonary oedema � For these reasons it is difficult to treat even for an experienced physician
ALCOHOL and PAIN KILLERS • increase stomach irritation • impair thinking and motor skills • lead to breathing problems.
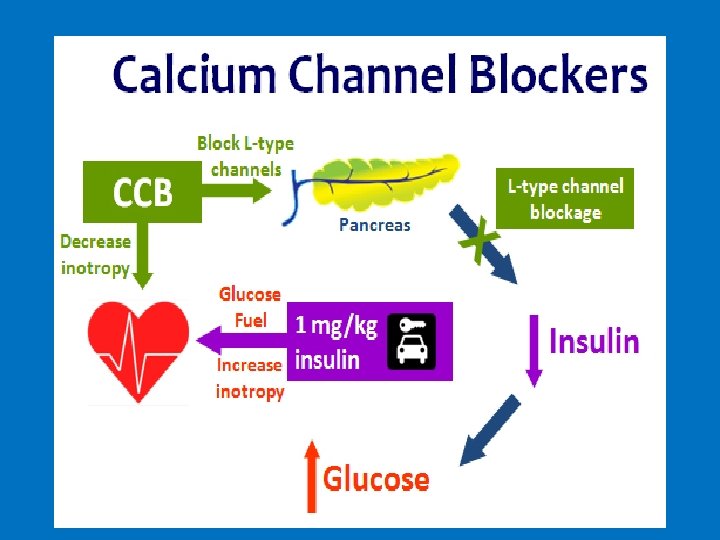
TREATMENT OF CCB TOXICITY � Calcium Therapy: as calcium gluconate or calcium chloride � Calcium gluconate , 30 m. L of 10% solution, can be administered IV over 10 -15 minutes in adults � Glucagon Therapy : promotes calcium entry into cells via stimulation of a receptor that is considered to be separate from adrenergic receptors � Administer glucagon 5 -10 mg IV bolus up to 15 mg, followed by an infusion � Insulin Therapy : Hyperglycaemia may occur in CCB toxicity, as calcium channel blockade inhibits insulin release. To counter act this Hyperinsulinemia- Euglycemia
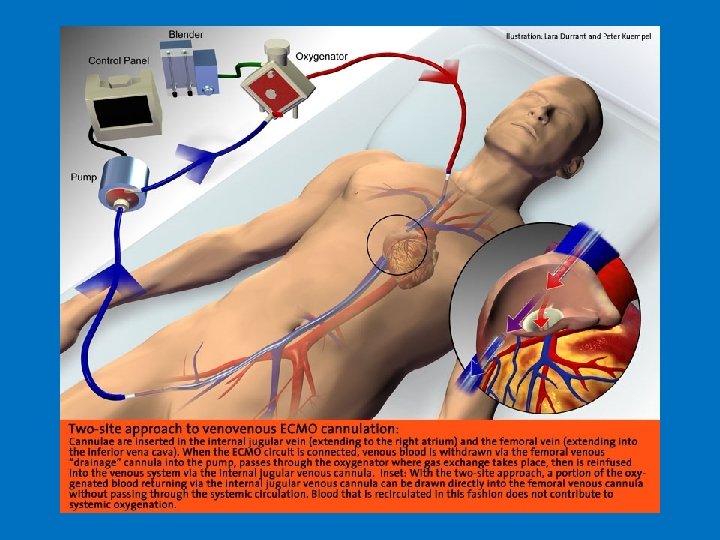
ECMO � Extracorporeal Membrane Oxygenation �Oxygen for the body when someone’s lungs and/or heart are not able to supply oxygen on their own VEIN DEOXYGENATED BLOOD ARTERY ECMO
�A known side effect of this therapy is risk of low blood flow to the distal part of the limb in which catheter is placed risk of causing clots � However this wasn’t given a keen eye to by the treating physician in the MDCCU. �Resulted in leg ischemia
NEGLIGENCE? ? ? ?
REASONS �Carelessness on part of the physician �Inadequate staffing �Lack of proper communication �Not foreseeing the known complications �Improper diagnostic techniques �Lack of immediate treatment �Insensitivity to patients needs �Incompetence of the physician – washing hands off
REFERENCES: � Buckley N, Dawson AH, Howarth D, Whyte IM. Slow- release verapamil poisoning. Use of polyethylene glycol whole-bowel lavage and high-dose calcium. Med J Aust. 1993 Feb 1. 158(3): 202 -4. [Medline]. � Hung YM, Olson KR. Acute amlodipine overdose treated by high dose intravenous calcium in a patient with severe renal insufficiency. Clin Toxicol (Phila). 2007. 45(3): 3013. [Medline]. � Haddad LM. Resuscitation after nifedipine overdose exclusively with intravenous calcium chloride. Am J Emerg Med. 1996 Oct. 14(6): 602 -3. [Medline].
� Levine M, Boyer EW, Pozner CN, Geib AJ, Thomsen T, Mick N, et al. Assessment of hyperglycemia after calcium channel blocker overdoses involving diltiazem or verapamil. Crit Care Med. 2007 Sep. 35(9): 2071 -5. [Medline]. � Mycyk MB, Bryant SM. Is simple bedside glucose assessment prognostic in calcium channel blocker overdose? . Crit Care Med. 2007 Sep. 35(9): 22167. [Medline]. � http: //emedicine. medscape. com/article/2184611 - treatment#d 17