Tetralogy of Fallot Beth Harrison Advisor Samuel Powdrill

Tetralogy of Fallot Beth Harrison Advisor: Samuel Powdrill, PA-C PAS 646

Outline • • • Review blood flow through the heart Discuss To. F anatomic abnormalities Etiology Clinical Presentation Labs and Exams Two surgical interventions

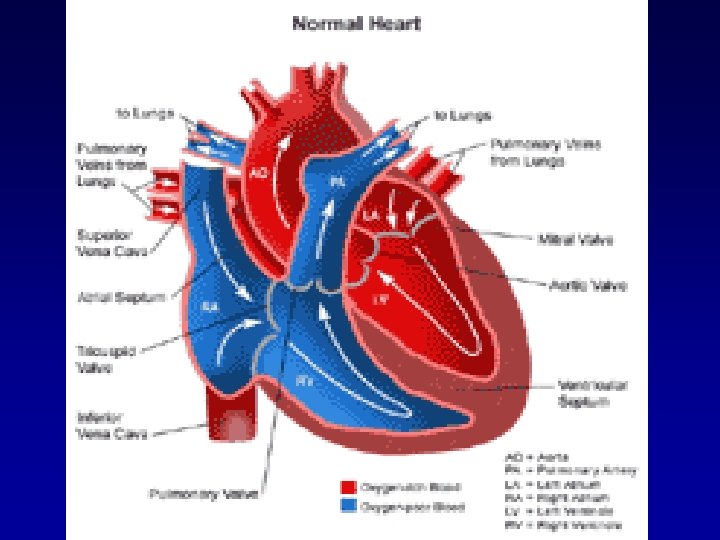
Healthy Heart Blood Flow • Deoxygenated blood from the body enters the RA • At the same time, oxygen rich blood leaves the lungs to flow into the LA • Blood in the RA enters the RV through the tricuspid valve • At the same time, blood flows from the LA to the LV through the mitral valve

Blood Flow cont. • Blood in the RV is pumped through the PA to the lungs • At the same time, LV pumps blood out the aorta to supply the body with oxygen rich blood • As seen in To. F, structural defects lead to the circulation of oxygen-poor blood

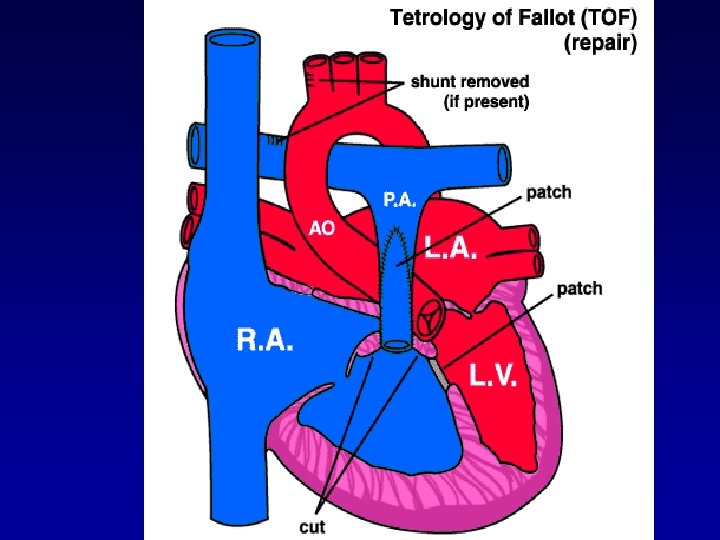
To. F • 4 anatomic malformations: -Right Ventricular Hypertrophy -Pulmonary Valve Stenosis -Transposition of the aorta -Ventricular Septal Defect

To. F • RVH -secondary to PA Stenosis -Increased P on RV leads to RVH • Transposition of Aorta -aorta is displaced • VSD -”hole in the heart” -mixing of oxygenated and unoxygenated blood -cyanosis • PVS -more severe, less blood transported to the lungs and more deoxygenated blood will pass through VSD to aorta to be circulated throughout the body

Etiology • Theory: destruction of the neuronal crest cells during embryogenesis • In the laboratory setting, destruction of these cells reproduced results displayed with certain cardiac malformations.

Clinical Presentation • Clinical presentation is directly related to the degree of pulmonary stenosis. • Severe stenosis results in immediate cyanosis following birth. Mild stenosis will not present until later. • Growth is retarded – insufficient oxygen and nutrients • SOA on exertion

“Tet Spell” • “Tet spells” at 23 yo, child becomes cyanotic, may experience syncope

Exams and Tests • CBC - hematocrit • ECG -RVH, RAD • CXR -boot shaped heart, right sided aortic arch • Echocardiogram -VSD

Surgical Intervention 1 • Complete intracardiac repair of VSD and PA stenosis. • Enter chest through the sternum. Connect the heart and lung machine. Heart is stopped. • Repair the VSD with a patch. • Determine if PA needs to be removed or if removing the excessive muscle tissue will help to function correctly.

• Pacemaker wires are placed temporarily because of the potential for postoperative ventricular arrhythmias. • Individual chamber pressures are then measured before the chest is closed. The pressure readings help to determine how effective the surgery was. • Complications: infective bacterial endocarditis, pulmonic regurgitation, arrhythmias, RBBB, or left anterior hemiblock

Surgical Intervention 2 • New method for patching the VSD • Transcatheter patches were selected specifically for VSD size. Radio-opaque loop inside of each patch allowed for attachment of double nylon thread. Made retrieval possible if necessary. • Pts were anticoagulated with heparin initially, followed with ASA 24 hr later.

• 48 hrs later the apparatus was inserted into the femoral vein were it was catherized until it reach the ascending aorta. • Echo was used to determine its location within the heart, allowing for proper placement of the patch for the VSD. • Pts were monitored in the ICU for 24 hrs. • Only 2 of the 16 pts in this study did not benefit from this study. In comparison to others, their VSD’s were much larger. • Pulmonary valvuloplastics were also performed. • Complications: there were no reported complications for VSD in this study

Why Do We Need to Know? • Not every case of To. F will be discovered by cardiologist and pediatricians. • Some symptoms will be subtle and present later in life to PCPs. • Several case studies discussed patients who chose not to have their To. F corrected. We need to know if To. F defects are causing their health problem or if the problems are from other sources.
. “Tetralogy of Fallot. ” 2005. Available")
References • • • American Heart Organization (AHO). “Tetralogy of Fallot. ” 2005. Available online: http: //www. americanheart. org/presenter. jhtml? identifier=11071 Greenberg, S. Bruce. “Tetralogy of Fallot. ” 2004 Emedicine. com, Inc. Available online: http: //www. emedicine. com/radio/topic 685. htm Inova Heart and Vascular Institute. “Tetralogy of Fallot. ” 2006. Available online: www. inova. org/inovapublic. srt/heart/pediatric_services/cardiac_surgery/tetralogy_of_fallot. html Moyano D. , I C Huggon, L D Allan. “Fetal echocardiography in trisomy 18. ” Originally published online 24 May 2005. Arch. Dis. Child. Fetal Neonatal Edition 2005; 90; pp. 520 -522. Pflieger, Kurt. “Tetralogy of Fallot. ” 2005 Emedicine. com, Inc. Available online: http: //www. emedicine. com/emerg/topic 575. htm Sideris, Eleftherios. “Transcatheter Patch Occlusion of Perimembranous Ventricular Septal Defects. ” The American Journal of Cardiology; 95(12), 15 June 2005, 1518 -1521. Warnes, Carole. “The Adult With Congenital Heart Disease. ” Journal of the American College of Cardiology; 2005; 26(1): 1 -8. Yang, X. , L J Freeman and C Ross. “Unoperated Tetralogy of Fallot: case report of a natural survivor who died in his 73 rd year; is it ever too late to operate? ” Postgraduate Medical Journal 2005; 81; 133 -134. Zeballos, Alvaro. “Tetralogy of Fallot. ” 2003 Emedicine. com, Inc. Available online: http: //www. emedicinehealth. com/fulltext/11205. htm
- Slides: 18