TETANUS DR I SELVARAJ I R M S








.")









To provide supportive care until the tetanospasmin")








 Ig- 1500 IU/s. c after sensitivity test (or) 2. ATS(human)")



, a disease preventable by immunization, is a major problem")
 Neo natal death rate")



- Slides: 47
TETANUS DR. I. SELVARAJ I. R. M. S B. SC. , M. B. B. S. , (M. D). , D. P. H. , D. I. H. , PGCH&FW/NIHFW, New Delhi Sr. D. M. O/S. RAILWAY (On study leave) Indian Railway Medical service
Photo Courtesy of U. S. Centers for Disease Control and Prevention
Courtesy: Google image on tetanus
CEPHALIC TETANUS : A Rare Form of Localized Tetanus Courtesy : Google image on tetanus)
Courtesy: Google image on tetanus
Newborn showing risus sardonicus and generalized spasticity
Tetanus is an acute, often fatal, disease caused by an exotoxin produced by the bacterium Clostridiumtetani. But prevented by immunization with tetanus toxoid. It is characterized by generalized rigidity and convulsive spasms of skeletal muscles. The muscle stiffness usually involves the jaw (lockjaw)and neck and then becomes generalized.
Epidemiology
• Tetanus was first described in Egypt over 3000 years ago(Edwin smith papyrus). It was again described by Hippocrates • Carle and Rattone in 1884 who first noticed tetanus in animals by injecting them with pus from a fatal human tetanus case. • During the same year, Nicolaier produced tetanus in animals by injecting them with samples of soil. • In 1889, Kitasato isolated the organism from a human victim, showed that it produced disease when injected into animals, and reported that the toxin could be neutralized by specific antibodies. • Nocard demonstrated the protective effect of passively transferred antitoxin, and passive immunization in humans • Passive immunization and prophylaxis for tetanus during World War I • Tetanus Toxoid was first widely used during world war II
• Tetanus - Greek Word -- Tetanos-to Contract • Tetanus Remains a Major Public Health Problem in the Developing World and Is Still Encountered in the Developed World. • There Are Between 800 000 and 1 Million Deaths Due to Tetanus Each Year. Eighty Per Cent of These Deaths Occur in Africa and South East Asia and It Remains Endemic in 90 Countries World Wide. • 1998 - U. K, USA 7 Cases, 41 Cases Including One Neonate
Acridine orange stain of characteristic C tetani with endospores wider than the characteristic drumstick shape.
Courtesy : Google Image on tetanus
• C. tetani is a slender, gram-positive, anaerobic rod that may develop a terminal spore, giving it a drumstick appearance. • The organism is sensitive to heat and cannot survive in the presence of oxygen. The spores, in contrast, are very resistant to heat and the usual antiseptics. • They can not survive autoclaving at 249. 8 °F (121 °C)for 20 minutes. • The spores are also relatively resistant to phenol and other chemical agents. • The spores are widely distributed in soil and in the intestines and faeces of horses, sheep, cattle, dogs, cats, rats, guinea pigs, and chickens. Manure-treated soil may contain large numbers of spores. Spores may persist for months to years. • C. tetani produces two exotoxins, tetanolysin and tetanospasmin. The function of tetanolysin is not known with certainty. Tetanospasmin is a neurotoxin and causes the clinical manifestations of tetanus. • Tetanospasmin estimated Human lethal dose 2. 5 ng/kg
• Occurrence: Tetanus occurs worldwide but is most frequently encountered in densely populated regions in hot, damp climates with soil rich in organic matter. • Reservoir: Organisms are found primarily in the soil and intestinal tracts of animals and humans. • Mode of Transmission: Transmission is primarily by contaminated wounds, Tissue injury( surgery, burns, deep puncture wounds, crush wounds, Otitis media , dental infection, animal bites, abortion, and pregnancy). • Communicability Tetanus is not contagious from person to person. It is the only vaccine-preventable disease that is infectious but not contagious. Temporal pattern: Peak in winter and summer season Incubation Period: 8 DAYS ( 3 -21 DAYS)
• Age : I t is the disease of active age (5 -40 years), New born baby, female during delivery or abortion • Sex : Higher incidence in males than females • Occupation : Agricultural workers are at higher risk • Rural –Urban difference: Incidence of tetanus is much lower than in rural areas • Immunity : Herd immunity does not protect the individual • Environmental and social factors: Unhygienic custom habits, Unhygienic delivery practices
Diagnosis Of Tetanus Clinically it is confirmed by noticing the following features: 1. Risus sardonicus or fixed sneer. 2. Lock jaw. 3. Opisthotonos (extension of lower extremities, flexion of upper extremities and arching of the back. The examiners hand can be passed under the back of the patient when he lies on the bed in supine position. ) 4. Neck rigidity
Type of Tetanus • • • Traumatic tetanus Puerperal tetanus Otogenic tetanus Idiopathic tetanus Tetanus Neonatorum
• Local tetanus is an uncommon form of the disease, in which patients have persistent contraction of muscles in the same anatomic area as the injury. Local tetanus may precede the onset of generalized tetanus but is generally milder. Only about 1%of cases are fatal. • Cephalic tetanus is a rare form of the disease, occasionally occurring with otitis media (ear infections)in which C. tetani is present in the flora of the middle ear, or following injuries to the head. There is involvement of the cranial nerves, especially in the facial area. • The most common type (about 80%)of reported tetanus is generalized tetanus. The disease usually presents with a descending pattern.
Three Objectives of Management of Tetanus • (1)To provide supportive care until the tetanospasmin that is fixed in tissue has been metabolized • (2)To neutralize circulating toxin • (3)To remove the source of tetanospasmin.
The rating scale for the severity and the prognosis of tetanus is described below. • Score 1 point for each of the following: • Incubation period less than 7 days • Period of onset less than 48 hours • Acquired from burns, surgical wounds, compound fractures, or septic abortion • Narcotic addiction • Generalized tetanus • Temperature greater than 104°F (40°C) • Tachycardia greater than 120 beats per minute (>150 beats per min in neonates) • Total score indicates the severity and the prognosis as follows: • Score of 0 -1 indicates mild severity with less than a 10% mortality rate. • Score of 2 -3 indicates moderate severity with a 10 -20% mortality rate. • Score of 4 indicates severe tetanus with a 20 -40% mortality rate. • Score of 5 -6 indicates very severe tetanus with greater than a 50% mortality rate. (http: //www. emedicine. com/ped/topic 3038. htm) Phillips, Dakar, . Udwadia Score
PREVENTION
Spores are extremely stable, although immersion in boiling water for 15 minutes kills most spores. Exposure to saturated steam under 15 lbs. of pressure for 15 -20 minutes at 121°c is highly effective against spores. Sterilization by dry heat is slower than by moist heat (1 -3 hrs at 160 °C), but it is also effective against spores. Ethylene oxide sterilization is also sporocidal.
Fumigation • Sterilization of operation theatre • 500 ml of formaline, 200 gms of Pot. permanganate/30 cu. meters of space • All windows and doors are closed except one • Fissures between the panels of the doors and windows are closed with adhesive tape • After 12 hours the doors and windows are opened and theatre is aired for 24 hours before decommissioning it
• • Active Immunization Passive Immunization Active and passive Immunization Antibiotics
TETANUS TOXOID • Tetanus toxoid was developed by Descombey in 1924, • Tetanus toxoid immunizations were used extensively in the armed services during World War II. • Tetanus toxoid consists of a formaldehyde-treated toxin. • There are two types of toxoid available —adsorbed (aluminum salt precipitated)toxoid and fluid toxoid. • Although the rates of seroconversion are about equal, the adsorbed toxoid is preferred because the antitoxin response reaches higher titers and is longer lasting than that following the fluid toxoid.
Tetanus Toxoid Adsorbed USP, for intramuscular use, is a sterile suspension of alum-precipitated (aluminum potassium sulfate)toxoid in an isotonic sodium chloride solution containing sodium phosphate buffer to control p. H. The vaccine, after shaking, is a turbid liquid, whitish-gray in color. Clostridium tetani culture is grown in a peptone-based medium and detoxified with formaldehyde. The detoxified material is then purified by serial ammonium sulfate fractionation, followed by sterile filtration, and the toxoid is adsorbed to aluminum potassium sulfate (alum). The adsorbed toxoid is diluted with physiological saline solution (0. 85%)and thimerosal (a mercury derivative)is added to a final concentration of 1: 10, 000. Each 0. 5 m. L dose is formulated to contain 5 Lf (flocculation units)of tetanus toxoid and not more than 0. 25 mg of aluminum. The residual formaldehyde content, by assay, is less than 0. 02%. The tetanus toxoid induces at least 2 units of antitoxin per m. L in the guinea pig potency test.
Active Immunization • • • 1 st dose 2 nd dose 3 rd dose 1 st booster 2 nd booster 3 rd booster - 6 th week - 10 th week 14 th week 18 th month 6 th year 10 th year
Passive Immunization 1. ATS(equine) Ig- 1500 IU/s. c after sensitivity test (or) 2. ATS(human) Ig- 250 -500 IU, no anaphylactic shock, very safe and costly.
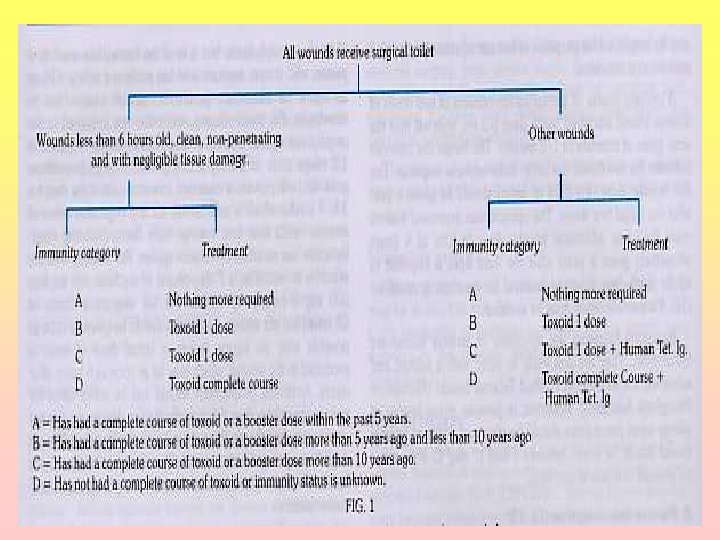
Persons Seven Years of Age or Older Who Have Not Been Immunized Immunization requires at least three doses of Td. 1 st dose should be administered on the First visit 2 nd dose 4 – 8 weeks after the first dose of Td and 3 rd dose after 6 months of the second Td. A booster dose of Td should be repeated every 10 years throughout life
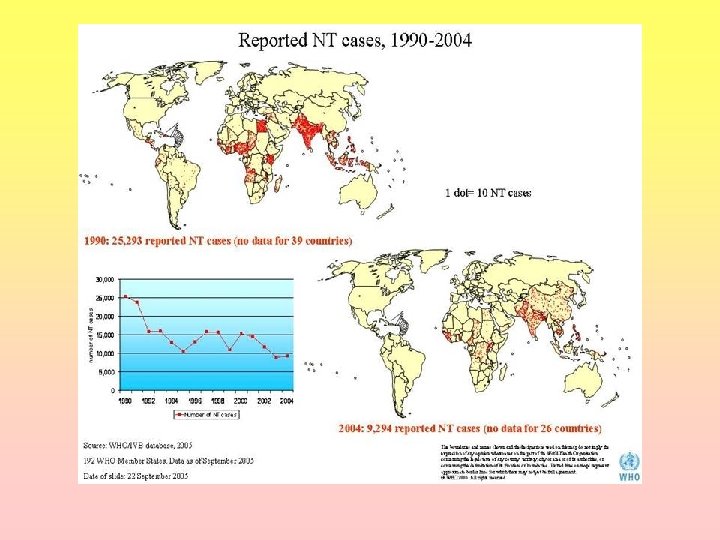
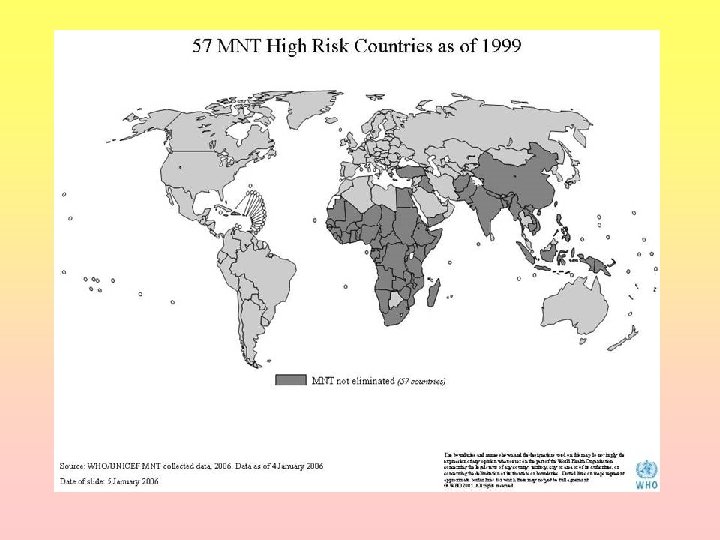
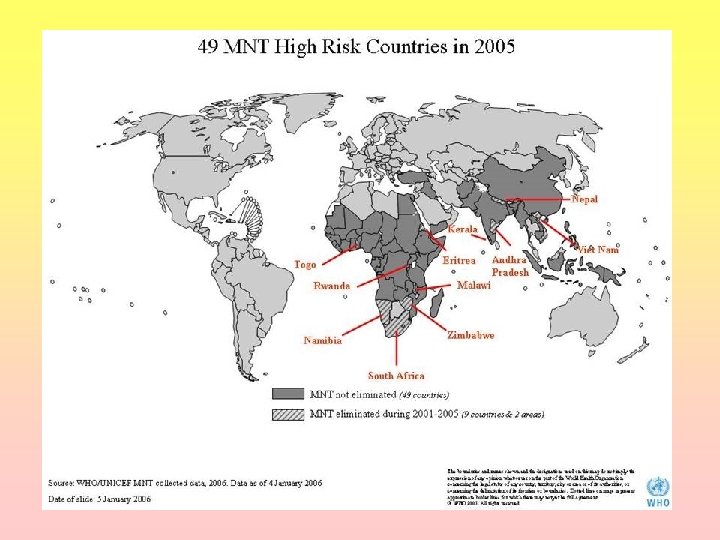
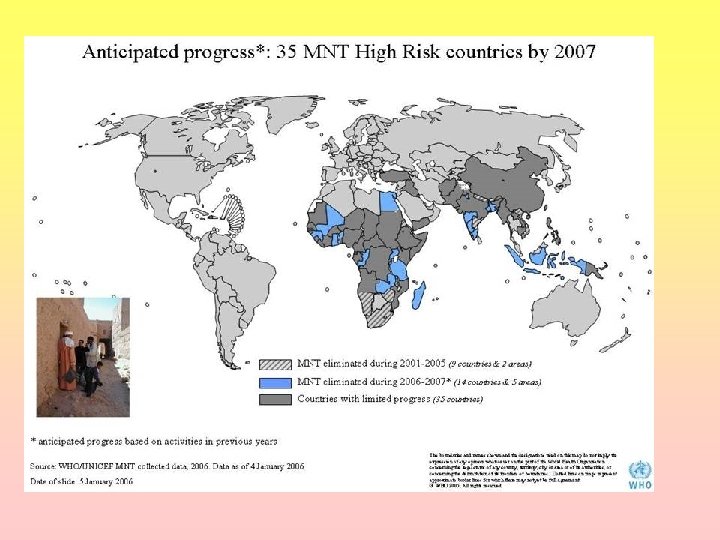
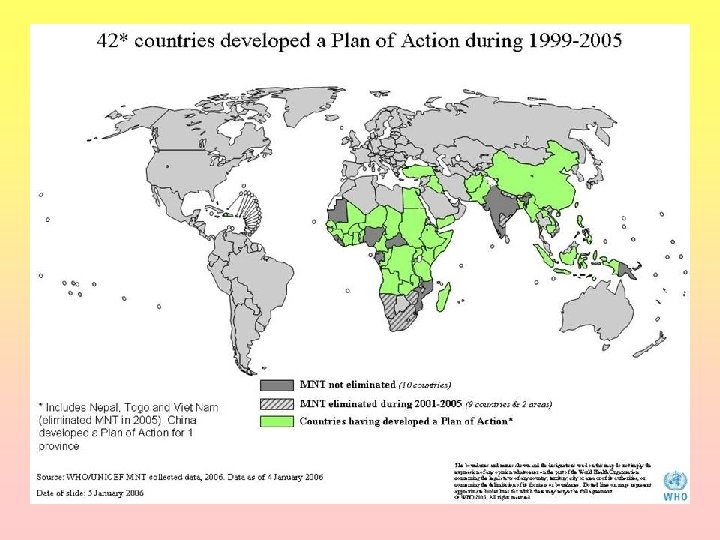
The Maternal and Neonatal Tetanus elimination initiative was launched by UNICEF, WHO and UNFPA in 1999, revitalizing the goal of MNT elimination as a public health problem - defined as less than one case of neonatal tetanus per 1000 live births in every district of every country
• Maternal tetanus, defined as tetanus occurring during pregnancy or within 6 weeks after any type of pregnancy termination, is one of the most easily preventable causes of maternal mortality. • It includes postpartum or puerperal tetanus (i) postpartum or puerperal tetanus, usually resulting from septic procedures during delivery, (ii) postabortal tetanus, following septic maneuvers during induced abortion and (iii) tetanus during pregnancy, generally resulting from inoculation through a nongenital portal of entry
• Neonatal tetanus (NNT), a disease preventable by immunization, is a major problem and a leading cause of neonatal mortality. • It is easily preventable by 2 tetanus toxoid injections and ‘ 5 cleans’ while conducting deliveries. • 2 major programs are in operation for the prevention of NNT in the country – • the immunization of pregnant women with tetanus toxoid vaccine (TT) under the expanded program on immunization (EPI) • and the training of dais under the rural health program. • NNT will be prevented if the women and the dais (who are still associated with almost 70 -75% of the deliveries in many areas with high NNT mortality rates) are convinced of the need for TT vaccination during the antenatal period and practice the basic principles of cutting cord and keeping the umbilical stump free of unclean dressings.
Elimination of Neo natal tetanus 1. High risk district: a) Neo natal death rate > 1/1000 live births b) 2 doses of tetanus toxoid coverage < 70% c) Deliveries attended by trained dais < 50% 2. Medium risk district: a) Neo natal death rate < 1 / 1000 live births b) 2 doses of tetanus toxoid coverage> 70% c) Deliveries attended by dais > 50% 3. Low risk district: a) NNT <0. 1/1000 Live Birth b) 2 Doses of T. T Coverage >90% c) Delivery attended by Trained Dais >75%
PREVENTION OF NEONATAL TETANUS • 2 doses of T. T to all pregnant women between 16 to 36 weeks of pregnancy with an interval of 1 to 2 months between the two doses. • The first dose as early as possible & the second dose a month later preferably 3 weeks before delivery. • If the pregnant woman is previously immunized, a booster dose is sufficient. • If the pregnant woman is not immunized, then the new born should be protected against tetanus by giving tetanus human immunoglobulin 750 IU with in 6 hours of birth.
REFERENCE • http: //www. medindia. net/health_statistics/diseases/tetanus. Tet anus J J Farrara b, L M Yenc, T Cookd, N Fairweathere, N Binhc, J Parrya b, C M Parrya b • http: //www. who. int/immunization_monitoring/diseases/Tetan us_map_cases. jpg • Txt book of preventive and social medicine 18 th edition by K. PARK • Text book of community medicine by T. Bhaskar Rao • Management and Prevention of Tetanus • Richard F. Edlich, MD Ph. D, ? Lisa G. . Hill, ? Chandra A. . Mahler, 툺ary Jude Cox, MD, ? Daniel G. . Becker MD, ? Jed H. . Horowitz, MD 4 Larry S. Nichter MD MS, 4 Marcus L. Martin, MD 5 &William C. Lineweaver MD 6 . www. rxlist. com/cgi/generic/tettoxpi. htm - 22 k . Manson’s Tropical diseases 21 st edition
THANK YOU