Terminal weaning or immediate extubation for withdrawing mechanical

Terminal weaning or immediate extubation for withdrawing mechanical ventilation in critically ill patients (the ARREVE observational study)

Introduction • Increasing number of deaths occur in ICU after a decision to withdraw life support • Major goal is to avoid unnecessary suffering due to prolongation of dying process • Relatives have been reported to experience psychological distress similar to PTSD, complicated grief, anxiety and or depression to degrees that vary according to treatments provided and quality of the dying of the patient

Introduction • Mechanical ventilation withdrawn either by immediate extubation or by terminal weaning (gradual decrease in ventilatory support) • Choice is controversial: whether it influences the experience of patients and relatives is unclear • Main challenge to mechanical ventilation withdrawal consists in preventing discomfort to patient and, therefore, additional distress to relatives

Introduction • Immediate extubation generally viewed as more natural dying process with less ambiguity but higher risk of patient discomfort related to airway obstruction • Previous studies suggested better satisfaction and lower rates of complicated grief among relatives of patients who died without ET tube • Other data suggest greater family satisfaction after terminal weaning and worse patient distress after immediate extubation

Introduction • No study has compared psychological variables of relatives after terminal weaning versus immediate extubation • Designed prospective observational multicentre ARREVE study to compare immediate extubation v terminal weaning regarding long term presence in relatives of PTSD-related symptoms, complicated grief, and symptoms of anxiety and depression. • Also compared comfort of patients during dying process and wellbeing of ICU staff members between the two methods

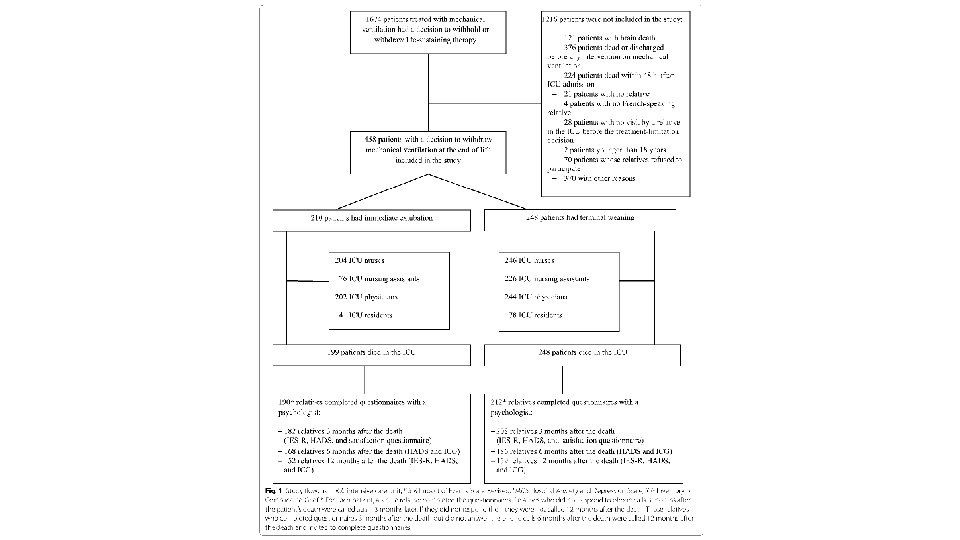
Methods • ARREVE – prospective, observational, multicentre study • 43 French ICUs • Feb 2013 -April 2014 • Critically ill adults with decision to withdraw invasive ventilation along with main adult relative of each were enrollled • Phone interview at 3, 6, 12 months

Exclusions • NIV • Brain death • Death <48 hr of ICU admission or before initiation of MV withdrawal • Relatives who didn’t speak French well enough • Those who declined to participate

Terminal Weaning v Immediate Extubation • Immediate extubation – extubation with no previous decrease in ventilatory assistance • Terminal weaning – decrease in amount of ventilatory assistance (O 2 + - TV +- PEEP +- RR +- spont with T piece) • Could include discontinuation of adjuncts (prone +- NO +- Almitrine) • Could include secondary extubation performed in event of prolonged dying causing distress to patient and/or family

Terminal Weaning v Immediate Extubation • Choice made by ICU physician and other staff members when decision to withdraw • According to local practice • Preference of relatives and staff • No specific recommendations about EOL care (including sedative use)

Study Outcomes • Patients – proportion of patients with airway obstruction +- gasping and behavioural pain scale • Relatives – Phone interview at 3, 6, 12 M: 1. Impact of Events Scale Revised (IES-R) to assess PTSD symptoms at 3 and 12. Score >32 implies PTSD related symptoms. IES-R 3 months after death was primary study outcome 2. Hospital Anxiety and Depression Scale (HADS) Relatives completed HADS at 3, 6, 12 M 3. Inventory of complicated grief (ICG) Scores >25 indicate complicated grief
 • Explored 3 domains: job")
• ICU staff completed Job Strain Score (JSS) • Explored 3 domains: job demand, control, social support • Nurse, nursing assistant, senior physician and resident completed JSS shortly after death or on day of ICU discharge

Sample Size • Planned to recruit 400 relatives • Somewhat arbitrary

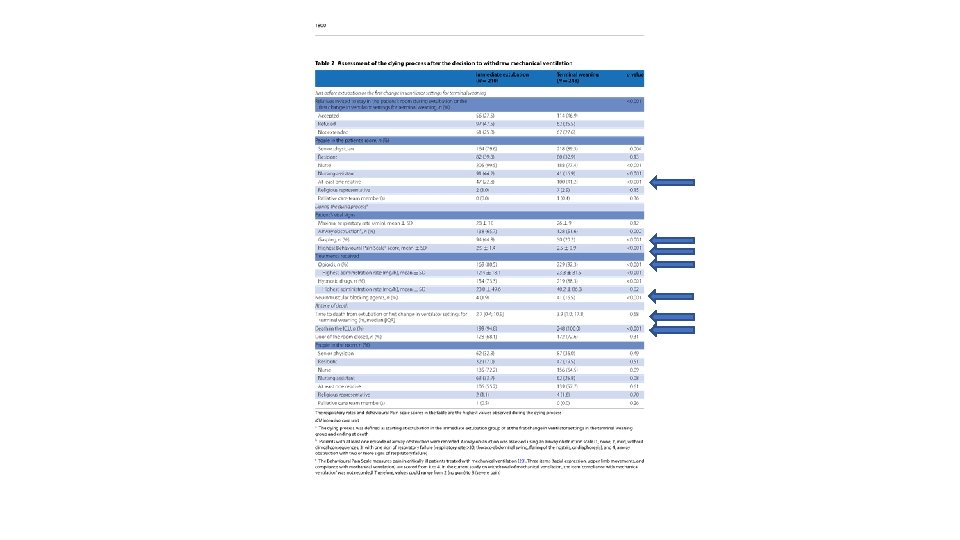
Results • Compared to relatives in terminal weaning group, those in immediate extubation more often involved in withdrawal decision and choosing between the two methods • Decisions to withdraw other life sustaining treatment more common in terminal weaning group • Other circumstances didn’t differ

Psychological Variables of Relatives - Primary • 3/12 after death, mean IES-R score was not significantly different between groups • Proportion of relatives with PTSD also similar (about 40%)

Psychological Variables of Relatives - Secondary • At 1 yr, neither mean IES-R nor frequency of PTSD differed significantly between groups • ICG scores showed no difference at 6/12 or 1 yr • Neither HADS schore nor frequency of anxiety/depression was significantly different between groups 3/12, 6/12 or 1 yr post death • Satisfaction of relatives, participation in decision making and respect of patient’s wishes were high with no difference between groups

Psychological Variables - Staff • Total JSS values in the assistant nurses were better with immediate extubation compared to terminal weaning • Satisfaction of residents with EOL care was lower in immediate extubation group, in the other 3 ICU staff categories, no significant differences found

Discussion • Large pragmatic multicentre observational study • First comparison of immediate extubation versus terminal weaning in terms of quality of death assessed by comfort of dying in patients and psychological well-being of relatives and ICU staff • Immediate extubation associated with greater airway obstruction, higher frequency of gasping and higher BPS scores

Discussion • In relatives, PTSD symptoms, complicated grief and symptoms of anxiety/depression up to 1 yr were not significantly different • In staff, job strain of nurses was lower with immediate extubation compared to terminal weaning • Under conditions of everyday practice, immediate extubation and terminal weaning were preferred by nearly identical proportions of ICU staff • In group differences suggest preference for immediate extubation in comatose patients and for terminal weaning in patients with respiratory failure

Discussion • Symptomatic airway obstruction and gasps more common and mean BPS score higher in immediate extubation group. • Directly related to removal of ET tube • ? underuse of analgesics and sedatives in patients undergoing immediate extubation • No difference in time from extubation or first change in ventilator settings between group

Discussion • ? Are physicians concerned about active shortening of dying process related to pre-emptive deep sedation after extubation • ? In terminal weaning group, greater use of opioids and sedatives and use of NMBs may reflect willingness to shorten dying process despite double effect principle • Guidelines discourage use of NMB at end of life • Use of NMBs may reflect attempt by ICU staff to avoid additional suffering in relatives • Agonal gasps • Myoclonus

• Psychological welfare of ICU staff was better with immediate extubation • Differences in perception have been noted • May be related to personal beliefs and therefore protocolising may be inappropriate

Limitations • Lack of randomisation • EOL care not standardised • Communication between ICU staff and relatives not evaluated in detail • All the units were in France

Conclusion • Immediate extubation not associated with difference in psychological welfare of relatives compared with terminal weaning • Compared with terminal weaning, immediate extubation associated with less job strain in ICU staff • Patients had more airway obstruction and gasps with immediate extubation indicating need for better palliative care
- Slides: 26