TEMPORAL BONE E Khalili Pooya Temporal bone Hypotympanum

ﺑﻪ ﻧﺎﻡ ﺧﺪﺍ TEMPORAL BONE E. Khalili Pooya
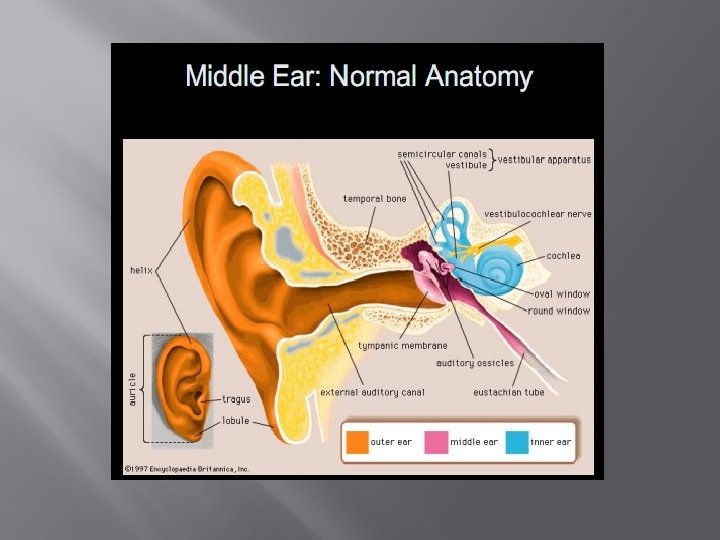

Temporal bone

Hypotympanum : Shallow space in floor of middle ear cavity
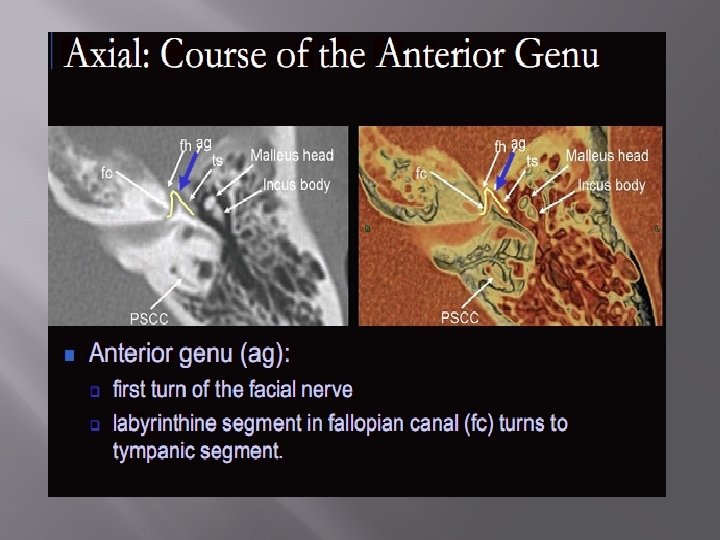
 � � Roof - tegmen tympani Floor - line between scutum and")
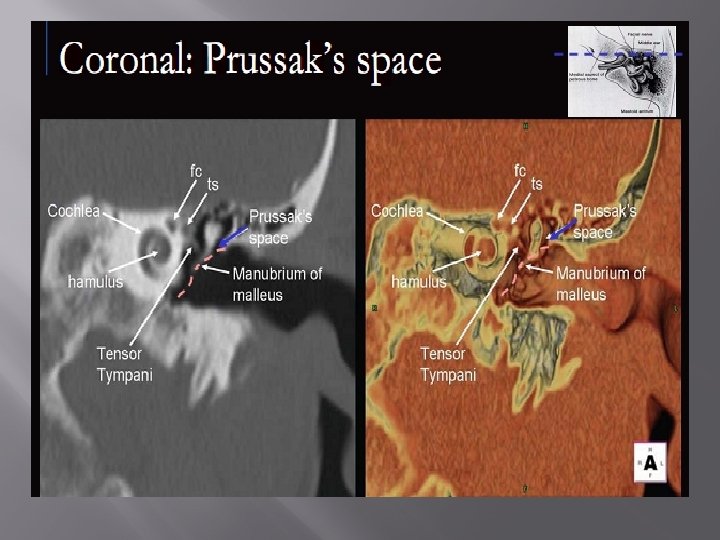
Epitympanum (attic) � � Roof - tegmen tympani Floor - line between scutum and tympanic portion of facial nerve Lateral - Prussak space Posterior - Aditus ad antrum leads to mastoid antrum

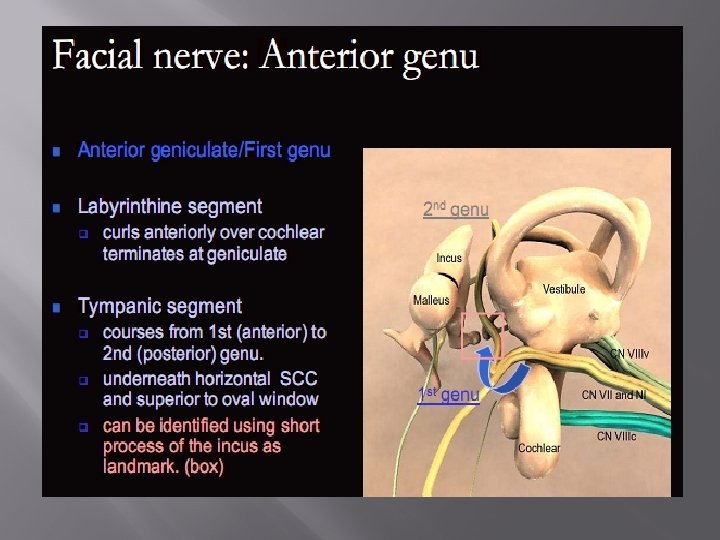
Mesotympanum * Roof - epitympanum * Floor - line between inferior edge of tympanic membrane and cochlear promontory * Anterior - Eustacian tube * Posterior - 3 key structures � • Facial nerve recess � • Pyramidal eminence � • Sinus tympani * Medial – Lateral semicircular canal – Oval and round windows – Tympanic segment CN VII

Conductive chain Tympanic membrane, ossicles, oval window � Tympanic membrane • Pars flaccida - upper 1/3 Two layers • Pars tensa - lower 2/3 Three layers: ectoderm, mesoderm, and endoderm. – More rigid than pars flaccida – Conducts vibrations to ossicles

Inner Ear: Anatomy

Perilymph: � Csf like extracellular fluid � Between membranous and bony labyrinths � Contiguous with the subarachnoid space � No appreciable “flow” Endolymph: � Fluid that fills the membranous labyrinth. � Unique in body - high K+ � “sealed” compartment maintained by ion exchange in endolymphatic sac

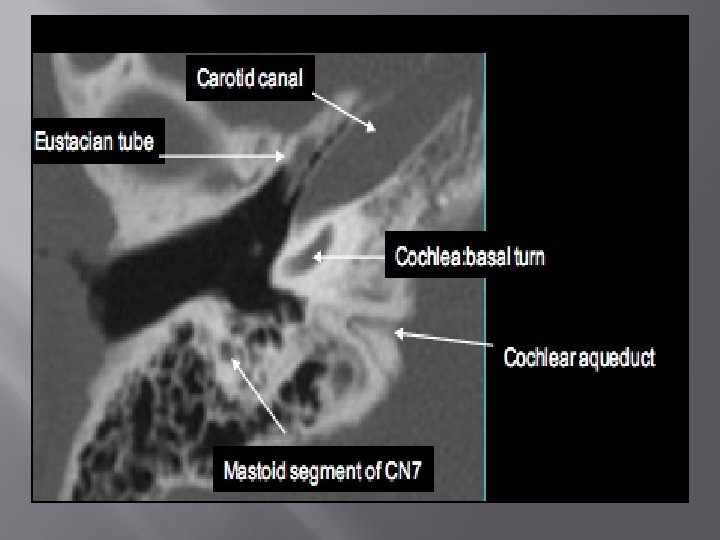
Cochlear aqueduct

Cochlear aqueduct � � The cochlear aqueduct connects the perilymph with the subarachoid space The cochlear aqueduct is a narrow canal which runs towards the cochlea in almost the same direction as the inner auditory canal, but situated more caudally It is a point where infected cerebrospinal fluid can enter the inner ear This can happen in patients with meningitis and cause labyrinthitis ossificans
")
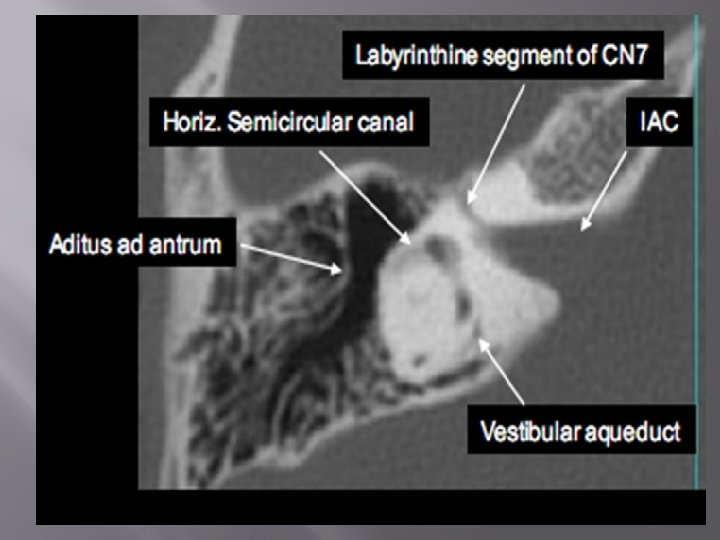
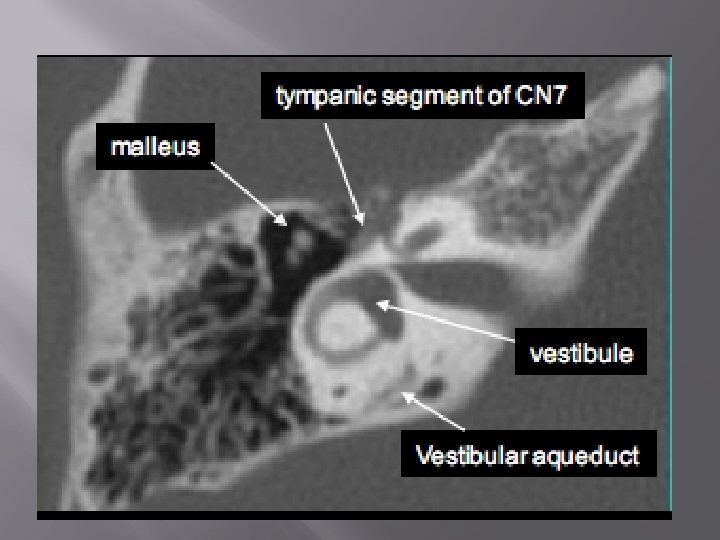
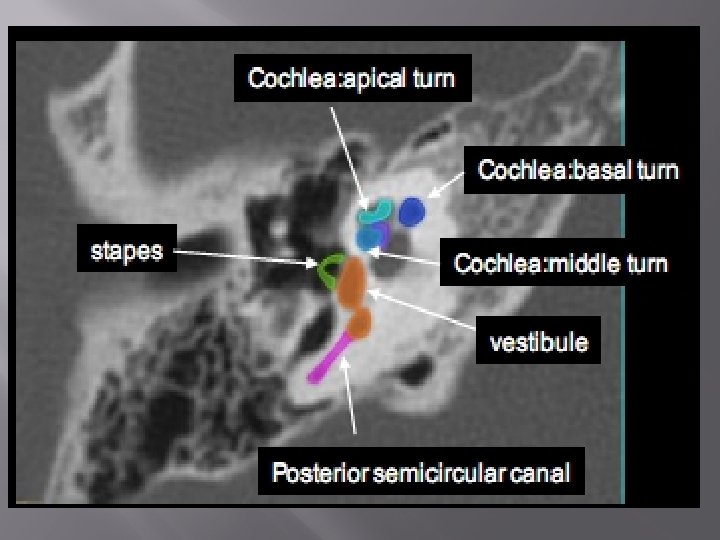
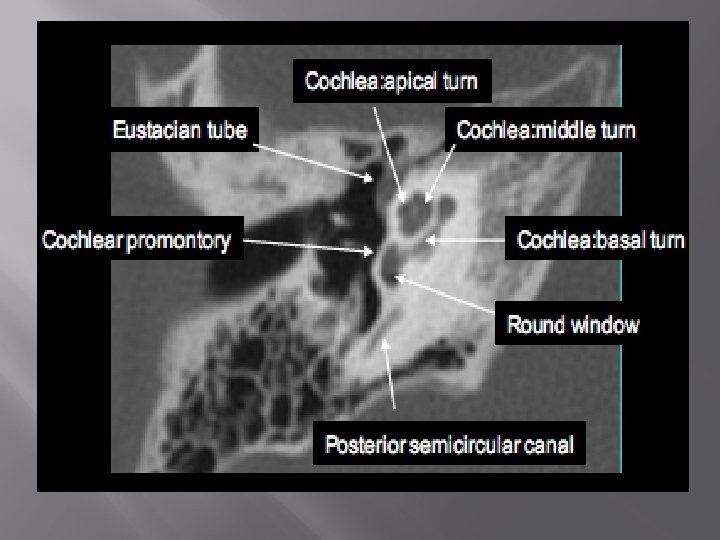
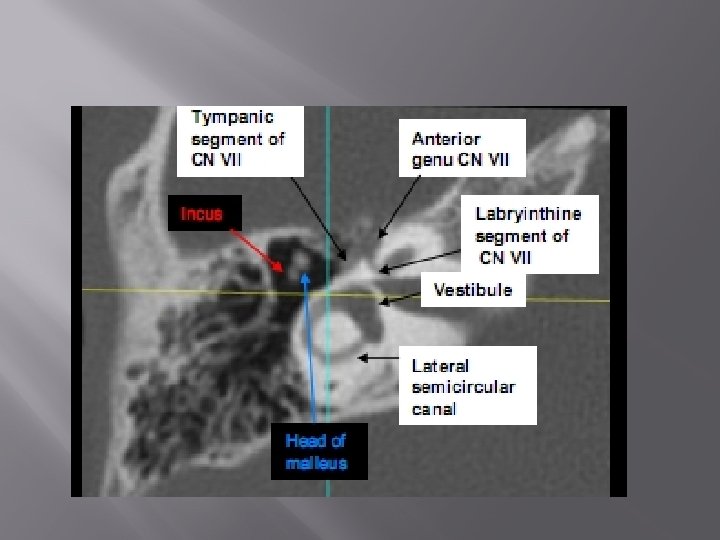
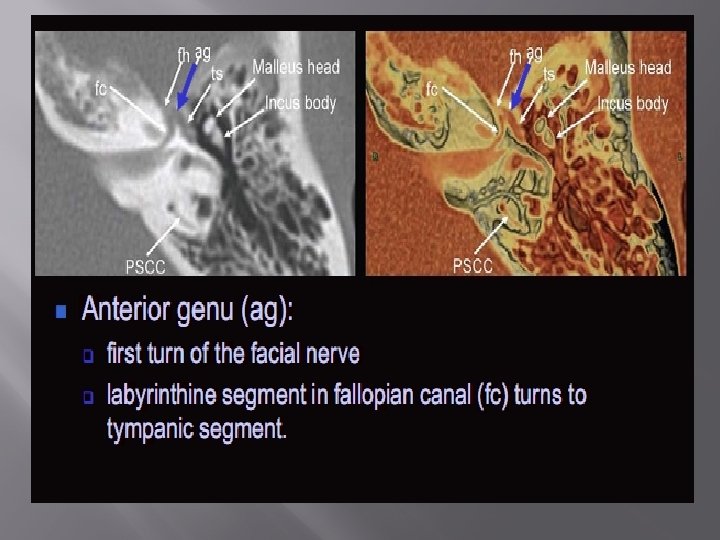
Axial anatomy in CT sections (from inferior to superior)
")
Malleus (yellow arow)
 Round window (blue arrow)")
Malleus (yellow arow) Round window (blue arrow)
 is seen connecting to the oval window")
Stapes (green arrow) is seen connecting to the oval window
 Round window (blue arrow)")
Malleus (yellow arow) Round window (blue arrow)

C=Cochlea, V=Vestibule

C=Cochlea, V=Vestibule

Semicircular canals
 Bill’s bar")
Transverse (falciform crest) Bill’s bar

Variants of Mastoid development HYPER-PNEUMATIZATION HYPO-PNEUMATIZATION

Bulging sigmoid sinus The sigmoid sinus can protrude into the posterior mastoid. It can be accidentally lacerated during a mastoidectomy

High jugular bulb � � � The jugular bulb is often asymmetric, with the right jugular bulb usually being larger than the left If it reaches above the posterior semicircular canal it is called a high jugular bulb If the bony separation between the jugular bulb and the tympanic cavity is absent, it is termed a dehiscent jugular bulb

Important variant: High jugular bulb, defect in hypotympanic floor AXIAL VIEW CORONAL VIEW

High jugular bulb

High jugular bulb

Dehiscent jugular bulb � Enlarged jugular bulb with dehiscence of sigmoid plate and protrusion of jugular vein into the posterior aspect of the middle ear.

Aberrant internal carotid artery � � Pulsative tinnitus Can look exactly like glomus tympanicum on coronal images Check for TUBULARITY on axials! DON’T BIOPSY!

Ectopic carotid artery: Posteriorly displaced canal passing into the middle ear

Carotid arteriogram, coronal projection ECTOPIC CAROTID ARTERY NORMAL

Ectopic carotid artery

Petromastoid canal

Petromastoid canal � � The petromastoid canal or subarcuate canal connects the mastoid antrum with the cranial cavity and houses the subarcuate artery and vein Its diameter is around 0. 5 mm

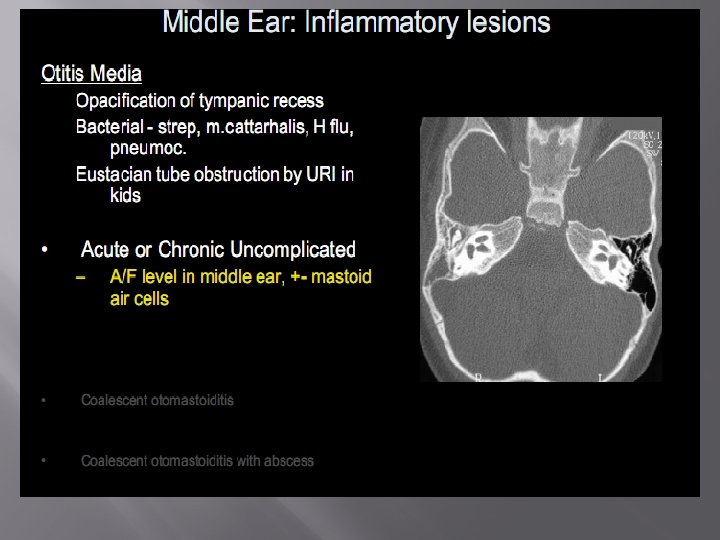
Acute otitis media and mastoiditis � � Air cell clouding Intact cell wall Fluid in middle ear No erosion in attic wall or ossicles

Tympanosclerosis: thickened tympanic membrane with plaque

Tympanosclerosis

Cholesteatoma

Cholesteatoma
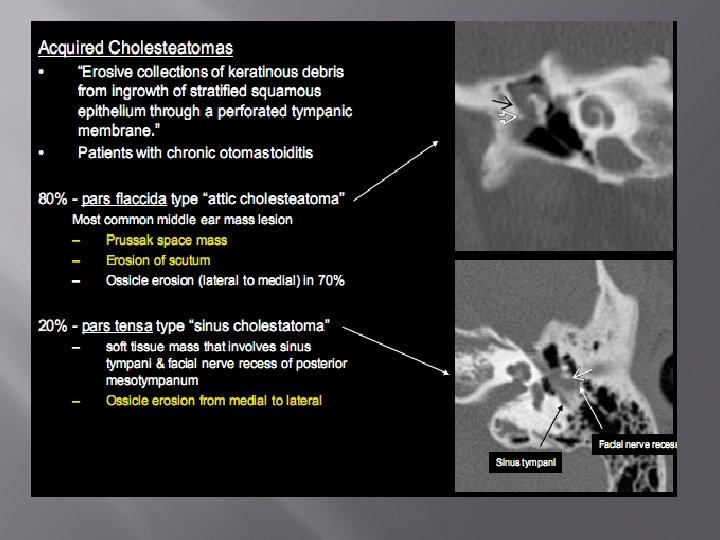

Congenital Cholesteatoma � � � =aka epidermoid Usually pediatric population Arise in variety of places in temporal bone. Middle ear involvement Bone erosion occurs late in disease Anterosuperior middle ear, adjacent to eustachian tube & anterior tympanic ring, medial to ossicles DDx : -pars tensa acquired middle ear cholesteatoma ( Ossicles commonly eroded) � -Glomus tympanicum paraganglioma ( No bony erosion , +CE on MRI) -Scwannoma of tympanic portion of CN VII

Cholesteatoma: Soft tissue mass in epitympanum, erosion of scutum & ossicles
 is visible between the scutum and the")
A small amount of soft tissue (arrow) is visible between the scutum and the ossicular chain but no erosion is present

Chronic otitis media vs cholesteatoma � � � Erosion of the lateral wall of the epitympanum and of the ossicular chain is common in cholesteatoma (around 75%) Erosion can occur in chronic otitis, but reportedly in less than 10% of patients Displacement of the ossicular chain can be seen in cholesteatoma, not in chronic otitis Cholesteatoma can present with a non-dependent mass while chronic otitis shows thickened mucosal lining However, in both diseases the middle ear cavity can be completely opacified, obscuring a cholesteatoma

Cholesteatoma: Soft tissue mass between ossicular chain and lateral tympanic wall, which is eroded

Paragangliomas: � � also known as glomus tumors or chemodectomas, are the second most common tumor to involve the temporal bone (after schwannoma)and the most common tumor of the middle ear. These tumors originate from paraganglia along the tympanic branch of the glossopharyngeal nerve (Jacobson nerve) and the auricular branch of the vagus nerve (Arnold nerve) and within the intravagal paraganglia inferior to the foramen. Paragangliomas are highly vascular. Paragangliomas may have a typical salt-andpepper appearance on T 1 -weighted and T 2 weighed images due to intermixed vascular flow voids and tumor tissue. They usually show avid enhancement on gadolinium-enhanced images.

Glomus Tympanicum paraganglioma � � Arises from glomus bodies at cochlear promontory Margin abutting cochlear promontory is flat Engulfs, not erodes ossicles DDx : * aberrant course of carotid artery * pars tensa cholesteatoma * epidermoid

Glomus Jugulare paraganglioma � Jugular foramen mass with permeative destruction of the adjacent bone and extension into hypo/mesotympanum

Glomus jugulare: Jugular fossa appears enlarged and the hypotympanic floor is eroded. Mass protrudes into the mesotympanum

Glomus jugulare tumor

Acoustic neuroma: Left IAC is enlarged by a mass extending into CPA BONE WINDOW POST-CONTRAST BRAIN WINDOW

Meningioma: Post-contrast CT scan Partially calcified mass protrudes from IAC into CPA. Hyperostotic changes narrow IAC
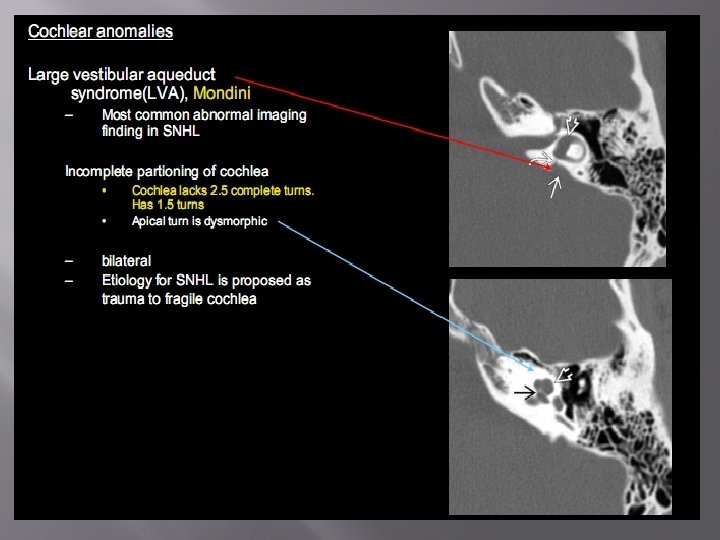

Large vestibular aqueduct
")
Large vestibular aqueduct � � The vestibular aqueduct is a narrow bony canal (aqueduct) that connects the endolymphatic sac with the inner ear (vestibule) Running through this bony canal is a tube called the endolymphatic duct A large vestibular aqueduct is associated with progressive sensorineural hearing loss The large vestibular aqueduct is associated with an absence of the bony modiolus in more than 90% of patients

Mondini deformity: Instead of the normal two-and-one-half turns, there is only a normal basal turn and a cystic apex

Labyrinthine ossificans � � � Ossifcation of membranous labyrinth as healing response to infection, trauma, surgery Classic presentation is bilateral SNHL in child after meningitis – Bone depostion in fluid spaces of vestible, semicircular canals and cochlea

Labyrinthitis ossificans

Labyrinthitis ossificans � � � Labyrinthitis ossificans is seen after meningitis It is a condition in which the inner ear is filled with fibrotic tissue, which calcifies It mostly affects the cochlea, but the vestibule and semicircular canals can also be involved

Otosclerosis � � is a genetically mediated metabolic bone disease of unknown etiology It is sometimes called otospongiosis because the disease begins with an otospongiotic phase, which is followed by an otosclerotic phase when osteoclasts are replaced by osteoblasts and dense sclerotic bone is deposited in areas of previous bone resorption When this process involves the oval window in the region of the footplate, the footplate becomes fixed, resulting in conductive hearing loss However, involvement of other portions of the otic capsule can result in mixed sensorineural hearing loss

Otosclerosis � � The process starts in the region of the oval window, classically at the fissula ante fenestram, i. e. in front of the oval window (fenestral otosclerosis) It can also occur around the cochlea (retrofenestral otosclerosis)

Cochlear Otosclerosis/otospongiosus � � Young adult with bilateral mixed hearing loss Focal lytic plaques in pericochlear bony labyrinth 85% bilateral symmetric – Unknown etiology Treated with flouride

Fenestral and cochlear otosclerosis: double ring appearance

Otosclerosis

Fenestral Otosclerosis/otospongiosus � � � Adults with conductive hearing loss More common than cochlear otosclerosis Similar process involving the oval and round window region Unknown etiology Flouride treatment slows hearing loss.
 and between the cochlea and the internal")
Lucency anterior to the oval window (arrow) and between the cochlea and the internal auditory canal. Combined fenestral & retrofenestral otosclerosis

Semicircular canal dehiscence � � thinning or absence of bony roof over superior or posterior semicircular canal Noise induced vestibular symptoms Unknown etiology Affects adults

Longitudinal fracture, bleeding in air cells

Coronal view, Incus dislocation and protrusion into canal

Transverse fracture involves vestibule and middle ear

Postoperative ear ATTICO-ANTROTOMY : MOST OF MASTOID AIR CELLS ARE PRESENT MASTOIDECTOMY: ALMOST ALL OF THE MASTOID AIR CELLS ARE REMOVED

� Thank you
- Slides: 94