Tecnica chirurgica selezione e posizionamento della protesi Paolo


 • Underlay (intraperitoneale) 4. 5 •")










 UO di Chirurgia")
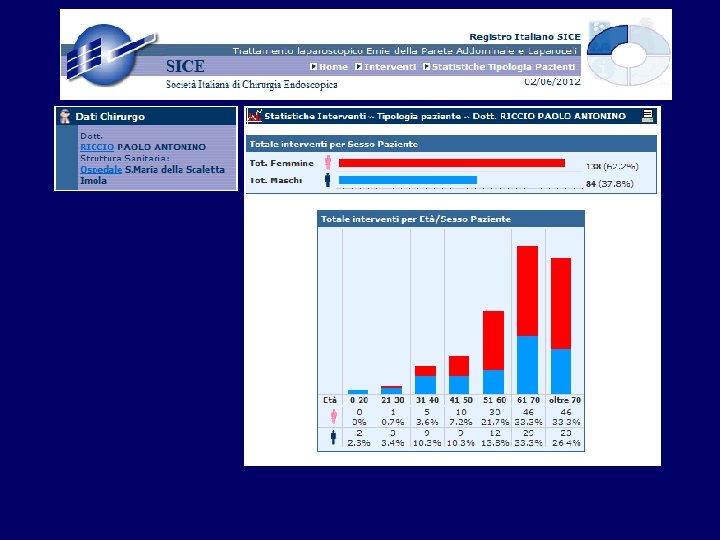
 Male/Female Age (y) Body mass index 84/138 61. 7 (15 -88)")
 Laparoscopic Incisional Hernia Repair - LIHR (172) Median laparotomies 145")
 ABDOMINAL BORDER (42) Subxiphoidal 8 Suprapubic 24 Subcostal 10 Type")
 20 (9. 0%) DYNA-MESH 12 (5.")
 ABSORBABLE TACK NON ABSORBABLE TACK 52 (23. 5%) 170 (76.")
 Use of Tissucol")
 Recurrence 12 (5. 4%) Conversion to open technique 8")
 Prolonged seroma (> 8 wk) 12 (5. 6%) Prolonged ileus 10 (4.")
 Time to recurrence (days): 537 (31 -1517) Treatment of recurrence:")
 Severity of adhesions 5 (2. 2%) Severity")
- Slides: 30
Tecnica chirurgica: selezione e posizionamento della protesi Paolo A. Riccio Chirurgia Imola
Rationale for laparoscopic approach • Avoiding dissection through previous operative sites within the abdominal wall and avoiding disruption of preexisting meshes • Not uncommon discovery of multiple small fascia defects Uranues 2008
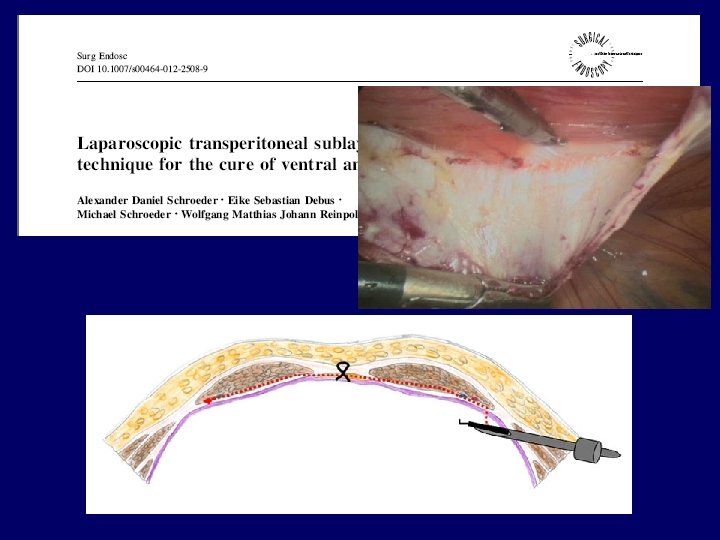
Posizionamento della rete e incidenza di recidive (%) • Underlay (intraperitoneale) 4. 5 • Sublay (preperitoneale) • Onlay • Inlay 8 14 48 Rudmik, Hernia 2006
The current recommendations to ensure the success of this hernioplasty can be summarized as follows. 1 Complete dissection of the entire anterior abdominal wall to expose all hernia defects. 2 Careful measurement of the fascial defects 3 Selection of a clinically proven prosthetic biomaterial 4 A minimum of a 3 cm overlap of all fascial borders with a larger area for obese patients or large recurrent hernias 5 Fixation of transfascial sutures and a metal fixation device Le. Blanc, World J Surg 2005
• 1, 5 milioni di reti vengono impiantate ogni anno nel mondo per il trattamento chirurgico del laparocele Weyhe, World J Surg 2007
Scelta della rete: evidenze dalla letteratura? …nessuna evidenza!!
rete ideale Ø prevenire aderenze Ø buona integrazione nella parete addominale Ø basso rischio di infezioni Ø resistenza alla tensione Ø sufficiente elasticità Ø biocompatibilità ( bassa reazione infiammatoria e shrinkage) Ø manegevolezza
Stabilità della rete v. Adeguato overlap v. Integrazione parietale v. Tecniche di fissaggio
Trends v. Reti leggere, coated mesh v. Macro + microporosità per una migliore integrazione tissutale e prevenzione dello shrinkage v. Maggiore elasticità v. Barriera antiadesiva
The current recommendations to ensure the success of this hernioplasty can be summarized as follows. 1 Complete dissection of the entire anterior abdominal wall to expose all hernia defects. 2 Careful measurement of the fascial defects 3 Selection of a clinically proven prosthetic biomaterial 4 A minimum of a 3 cm overlap of all fascial borders with a larger area for obese patients or large recurrent hernias 5 Fixation of transfascial sutures and a metal fixation device Le. Blanc, World J Surg 2005
Misurazione interna
v. Le dimensioni dell’ernia sono calcolate attraverso il posizionamento di 4 aghi passati dall’esterno a delimitare i margini del difetto parietale v. Il diametro è la distanza fra gli aghi in centimetri Misurazione extracorporea
Tecnica chirurgica • La rete viene temporaneamente ancorata alla parete addominale da 4 punti cardinali (6 nei laparoceli > di 10 cm) per consentire una adeguata distensione e l’orientamento
Experience of laparoscopic incisional and ventral hernia repair (2005 – 2012) UO di Chirurgia Dir. Dott. S. Artuso
Patient Characteristics (222) Male/Female Age (y) Body mass index 84/138 61. 7 (15 -88) 28. 8 (18 -45) ASA classification Previous open hernia repair 2. 1 (1 -3) 24 (10. 8%) Max diameter size (cm) Operating time (min) Postoperative hospital stay (d) Associated procedures 8. 4 (2 -28) 97. 5 (25 -240) 4. 8 (1 -27) 15 10 cholecistectomy 5 inguinal hernia
Type of defect (1) Laparoscopic Incisional Hernia Repair - LIHR (172) Median laparotomies 145 Lateral: 24 Left side 5 Mc Burney 5 Subcostal 10 Lumbar hernia 4 Parastomal 3 Laparoscopic Ventral Hernia Repair - LVHR (50) Umbilical hernia 29 Epigastric hernia 21
Type of defect (2) ABDOMINAL BORDER (42) Subxiphoidal 8 Suprapubic 24 Subcostal 10 Type of defect (3) Chevrel classification Small (<= 5 cm) 45 (20. 2%) Medium (6 -9 cm) 69 (31. 0%) Large (=> 10 cm) 71 (32. 1%) Type of defect (4) Swess-Cheese 37 (16. 7%)
Type of Prosthesis SEPRAMESH VENTRALIGHT 40 (18. 0%) 20 (9. 0%) DYNA-MESH 12 (5. 4%) PARIETEX 5 (2. 2%) COMPOSIX 33 (14. 8%) PROCEED 110 (49. 5%) PHISIOMESH 2 (0. 9%)
Type of fixation (1) ABSORBABLE TACK NON ABSORBABLE TACK 52 (23. 5%) 170 (76. 5%)
Type of fixation (2) Use of Tissucol
OUTCOMES Complications 32 (14. 4%) Recurrence 12 (5. 4%) Conversion to open technique 8 (3. 6%)
COMPLICATIONS (32) Prolonged seroma (> 8 wk) 12 (5. 6%) Prolonged ileus 10 (4. 7%) Prolonged pain (> 6 months) 5 (2. 3%) Pulmunary Embolism 1 (0. 6%) Myocardial Infarction 1 (0. 6%) Pneumonia + wound infection 1 (0. 6%) Wound infection 2 (0. 9%) RE-OPERATION (7) Intestinal injury 4 (1. 8%) Postoperative bleeding 2 (0. 9%) Trocar site erniation 1 (0. 6%)
RECURRENCE 12 (5. 4%) Time to recurrence (days): 537 (31 -1517) Treatment of recurrence: Laparoscopic repair 2 Open repair 5 No repair 5
CONVERSION TO OPEN TECHNIQUE 8 (3. 6%) Severity of adhesions 5 (2. 2%) Severity of adhesions and obesity 1 (0. 5%) Complete prosthesis detachment 1 (0. 5%) Intestinal injury 1 (0. 5%)