Technique and Benefits of Cutdown vs Percutaneous Access

Technique and Benefits of Cutdown vs. Percutaneous Access Rajesh Malik MD, RPVI Associate Program Director, Vascular Surgery Residency and Fellowship Med. Star Washington Hospital Center

Rajesh Malik MD, RPVI I have no relevant financial relationships

Femoral Access • Historically access to the common femoral artery has been obtained via surgical cutdown • There is growing literature that percutaneous access is safe alternative with possibly more benefit to the patients

Open Femoral Access § Incision made inferior/caudal to the inguinal ligament § Dissection carried through Scarpa’s fascia § Femoral sheath opened and vascular control obatined with vessel loops
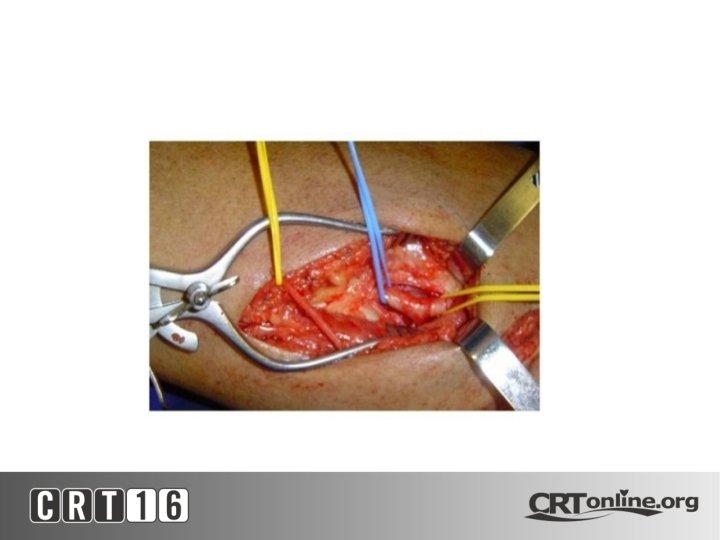

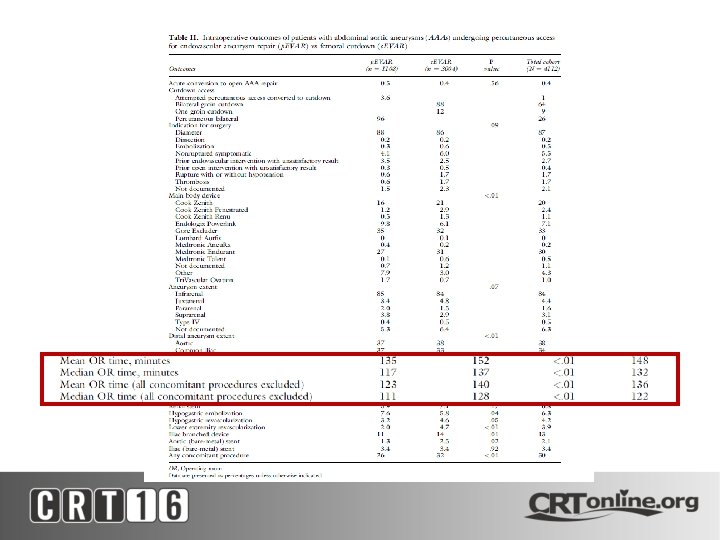
• Pros – Direct visualization of vessel for repair – Gives the option to do adjunctive procedures if needed – If vessels extremely tortuous, gives opportunity to straighten out by pulling vessel – Useful when multiple exchanges are required • Cons – – Increase OR time Increase blood loss? Wound complications Possibly increase LOS

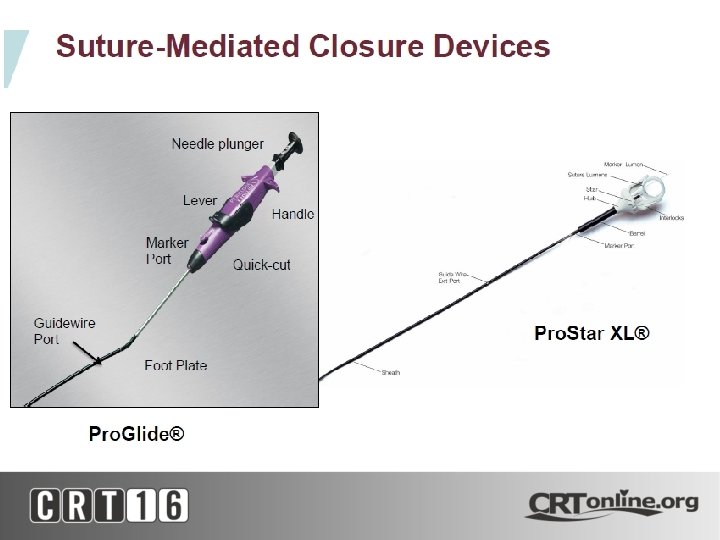
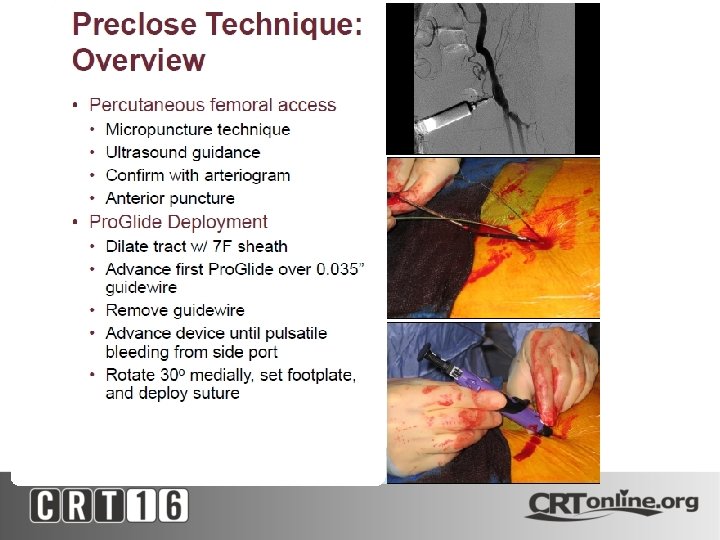
Percutaneous Access • The use of closure devices has gained wide popularity since introduction in the 1990 s • They’ve been used increasingly to close largebore arterial punctures like in EVAR, TEVAR and TAVI/TAVR • Reported success rates have been high(66100%) • FDA approved to close large sheath access

Success rate 87%access sites 93. 5% 154 femoral pts Year of 101 procedure, 96%Conversion in 168 pts larger sheaths, 90. 1% calcification, female Access diameter ratio to CFA diameter Successful deployment, genderuse of US
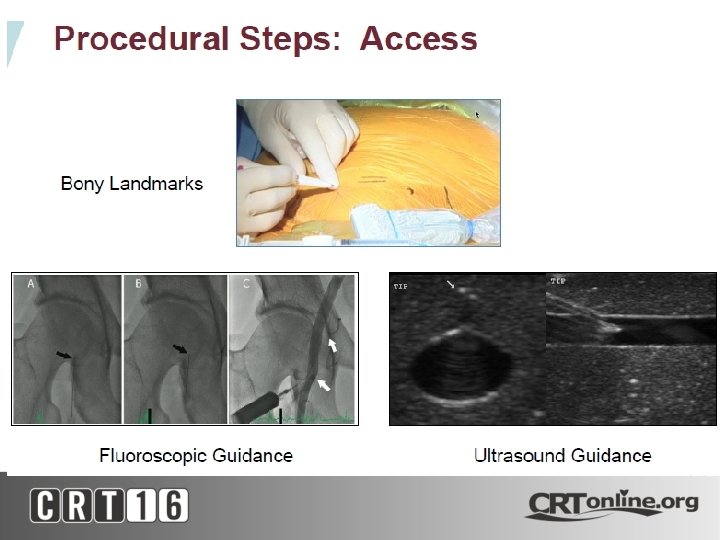



Amount of calcification
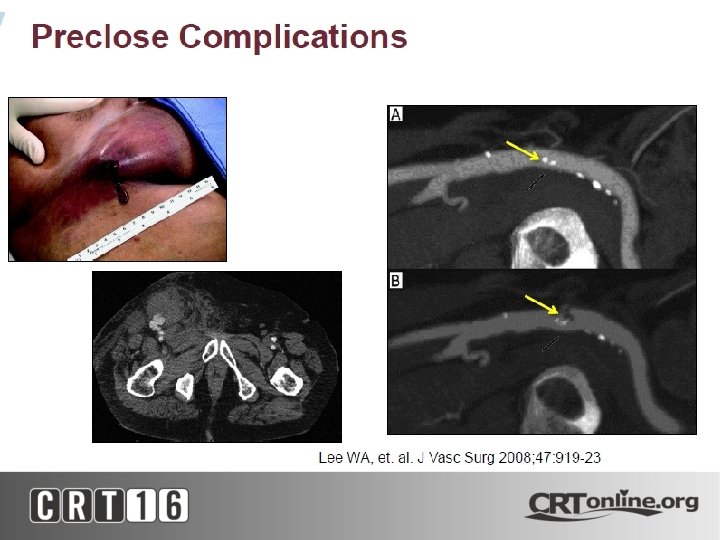

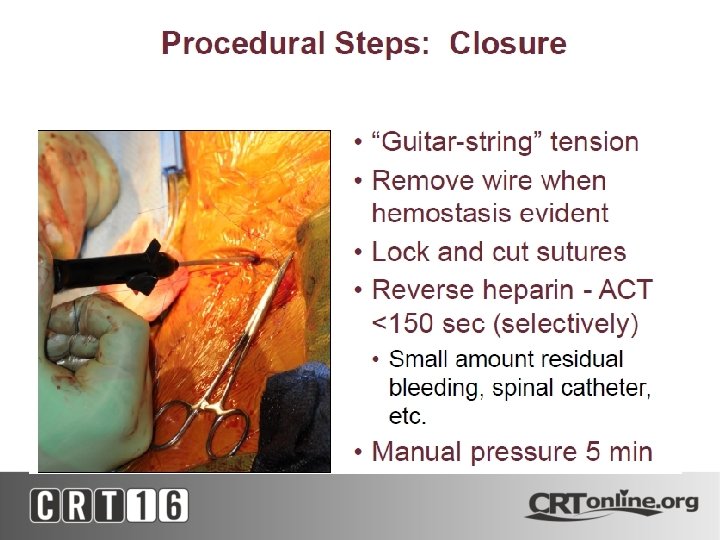
• Pros – Less OR time, EBL – Pateint comfort – Potentially decreased LOS • Cons – Failure of device with bleeding – Pseudoaneurysm/ dissections

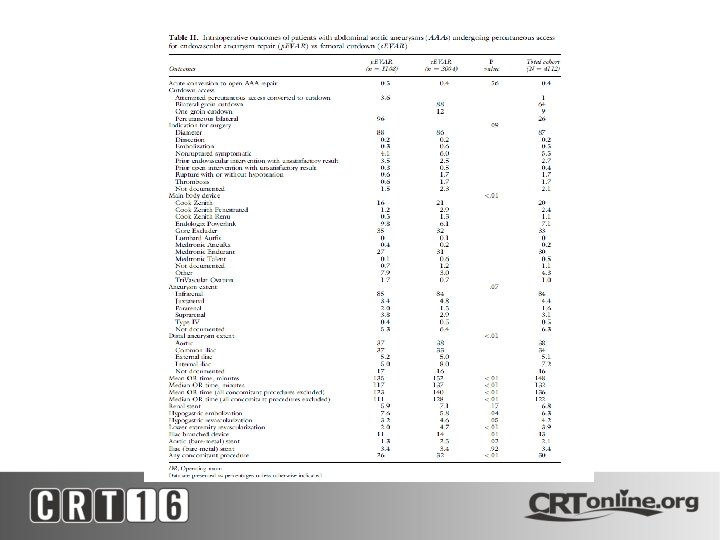
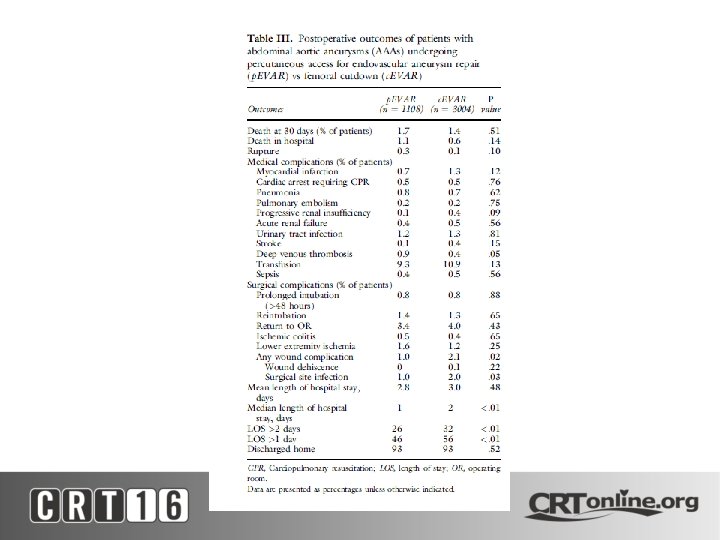
• Retrospective Review of NSQIP dataset from 2011 -2013 • 4112 patients identified • 3004 c. EVAR (cutdown) & 1108 p. EVAR (perc)
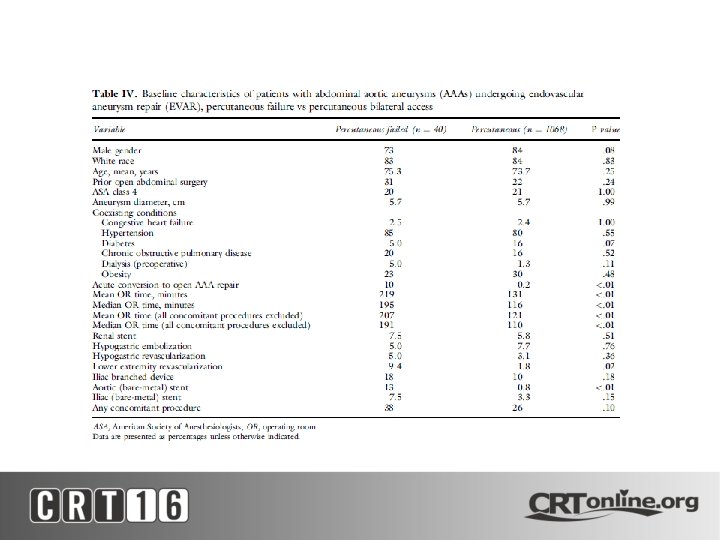

• p. EVAR failure from other studies: – Vessel diameter – Type of closure device – Femoral artery calcification – Access vessel tortuosity – Groin scars

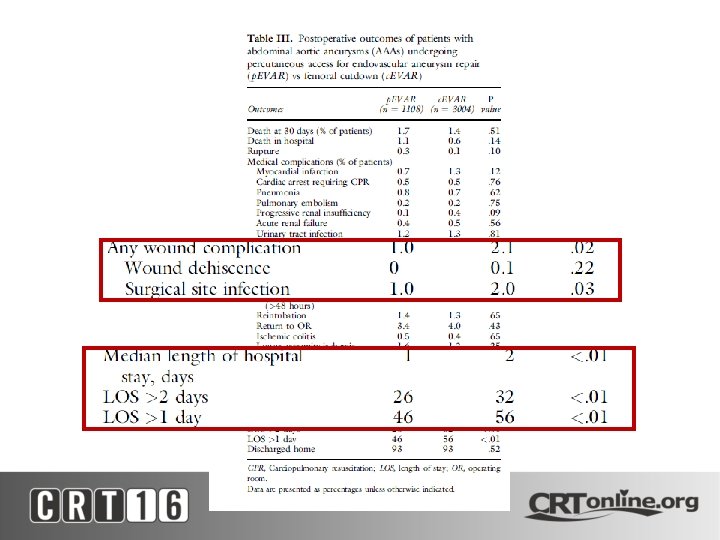
• Conclusion from Study – High technical success rates with p. EVAR – Shorter length of stay – Fewer wound complication – Predictor of percutaneous access failure was performance of any concomitant procedure

• Patient Selection Key to Good outcomes • Patient Group that is not conducive to p. EVAR – Females with small access – Calcified femoral arteries – Obesity with BMI >40 – Recent femoral access/intervention (? ) – Prior groin incision (bypass, c. EVAR etc) – Procedure requiring multiple sheath exchanges

- Slides: 32