TBS Trabecular Bone Score as a New DXADerived
 as a New DXA-Derived Measurement")
TBS (Trabecular Bone Score) as a New DXA-Derived Measurement

outlines • • • DXA & FRAX problems TBS method Case presentation Fracture risks (TBS/TBS-FRAX) TBS on treatment TBS and conditions(DM/HPT) related to increased fracture risk • conclusion

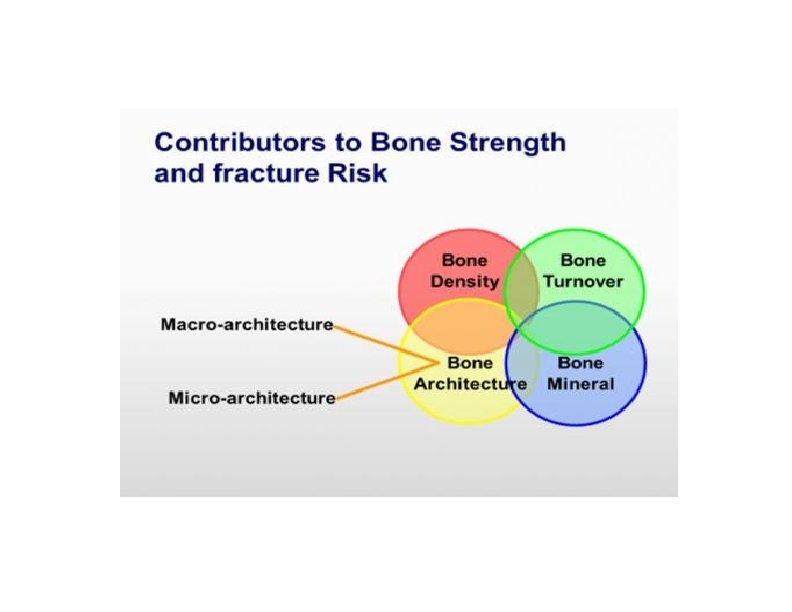
ü Osteoporosis is characterized by compromised bone strength, predisposing to an increased risk of fracture. ü An accepted operational definition for osteoporosis in postmenopausal women or in men age 50 years and older is when BMD by DXA is 2. 5 or more SDs below the average young reference value (ie, a T score 2. 5). ü Low BMD by DXA is a strong predictor of fracture risk: for each SD decrease in BMD, there is a 1. 4 -fold to 2. 6 -fold increase in the risk of fracture. ü Most individuals with fragility fractures have BMD values that do not fall within the osteoporotic range. Therefore, the identification of other skeletal and extraskeletal risk factors that contribute to overall fracture risk can be used to better select patients for treatment. BC Silva. Trabecular Bone Score A New DXA–Derived Measurement for Fracture Risk Assessment. Endocrinol Metab Clin North Am. 2017

DXA errors Ø Ø Ø incorrect patient positioning Analysis failure to consider confounding artifacts that affect BMD values inappropriate reference database use for T-score derivation failure to recognize densitometer drift or shift that could lead to reporting an inappropriate BMD change, thus leading to alteration of therapy, failure to change therapy, and/or unnecessary diagnostic studies Ø failure to perform precision assessment, resulting in inability to distinguish between an apparent BMD difference that is simply within the range of error of the test vs one that is statistically significant. Lewiecki EM Best Practices for Dual-Energy X-ray Absorptiometry Measurement and Reporting: International Society for Clinical Densitometry Guidance. J Clin Densitom. 2016

• DXA does not always translate into an accurate estimate of future fracture risk. Walker-Bone K. Recognizing and treating secondary osteoporosis. Nat Rev Rheumatol. 2012
")
FRAX calculator contʹd q FRAX calculator requires dichotomous (i. e. , yes or no) answers for risk factors, which are actually associated with a range of risks depending on modifying factors such as dose, length of exposure, or severity. Additionally, as the number of prior osteoporosis-related fractures increases or the dose of glucocorticoids rises, the risk of future fractures increases, yet these considerations are not included in the FRAX algorithm. q In children, the correlation between BMD and fracture risk is not well established; a FRAX algorithm for the pediatric population does not yet exist.
 • This novel method, which is entirely noninvasive and, in")
trabecular bone score (TBS) • This novel method, which is entirely noninvasive and, in fact, requires no further patient testing, has been repeatedly shown to be a BMD-independent predictor of skeletal strength and fracture risk. • It consists of gray-scale textural analysis of anteroposterior LSDXA images previously obtained for BMD assessments. It also, by assessing the micro-architectural texture of trabecular bone, contributes to the evaluation of bone strength, thereby aiding in the diagnosis of osteoporosis and the prediction of future osteoporotic fractures Silva BC, et al. Trabecular bone score: a noninvasive analytical method based upon the DXA image. J Bone Miner Res. 2014

TBS: 1. 512 TBS: 1. 196 TBS greater than or equal to 1. 350 is considered normal

§ TBS i. Nsight is a software program to evaluate bone microarchitecture in clinical practice and enhance fracture risk prediction. § TBS is an independent risk of fracture and therefore an additional clinical risk factor. As such, it should be interpreted in accordance with appropriate guidelines and according to the good practice as defined in the Position Development Statements of the International Society for Clinical Densitometry (ISCD). Compendium of TBS Clinical Case Studies first edition: March 2016

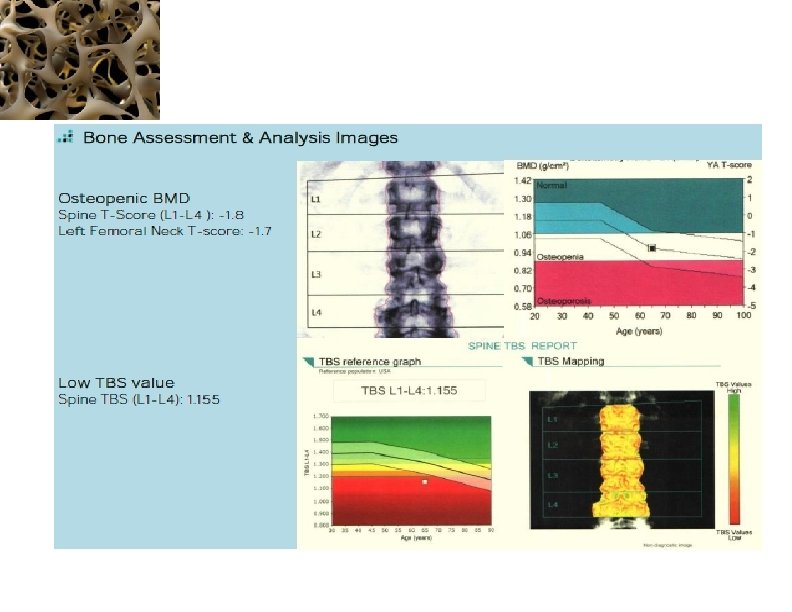
65 -year Old Woman Osteopenic BMD Low TBS Jane Doe is a 65 -year old white female who is concerned about fracture risk, as her mother recently fell and sustained a hip fracture. Her mother had previously sustained three vertebral fractures, the first of which occurred at age 68. Ms. Doe is generally healthy, taking only a statin for hyperlipidemia. Her diet provides ~1, 000 mg of calcium and she takes 1, 000 IU of supplemental vitamin D 3 daily. She does not smoke, drinks one glass of wine daily and walks for ~30 minutes three to five times a week. Her menopause was at age 48, and she never received estrogen therapy. She has no personal history of fragility fracture, rheumatoid arthritis or glucocorticoid use. Laboratory evaluation included serum calcium, creatinine, phosphorous, PTH, and 25 (OH)D, all of which were normal. Dr Neil Binkley, Geriatrics University of Wisconsin Hospital and Clinics, Madison, WI, USA

18% 1. 2 Adjust for TBS Treatment: MOF≥ 20% Or HF≥ 3%

Conclusion & Patient Management Decision In this individual, the estimated 10 -year probability of major osteoporosis related fracture is 18%. Based on this, she does not meet current NOF guidelines for therapy. However, her TBS is 1. 155. The 10 -year probability of major osteoporotic related fracture adjusted for TBS is 21%. Based upon this, she does meet treatment guidelines.

Is TBS Affected by Degenerative Vertebral Osteoarthritis? 2013 § subgroup of 390 women aged 50 to 88. 5 years § cross‐sectional study § designed to evaluate age‐related changes in TBS in a cohort of white French women Subjects were allocated to two groups according to the presence or absence of OA exclusively at the L 4 vertebral level, in accordance with the International Society for Clinical Densitometry (ISCD) definition. § There was no significant difference between cases and controls for BMD and TBS at L 1 to L 3. The severity of OA was defined by the differences between L 3 and L 4. At L 4 vertebral level, BMD was significantly greater in cases than in controls (þ 19%), whereas no significant difference in TBS was found between the groups (– 3. 2%)

P= 0. 426 TBS -3. 2% 19% BMD p<0. 001
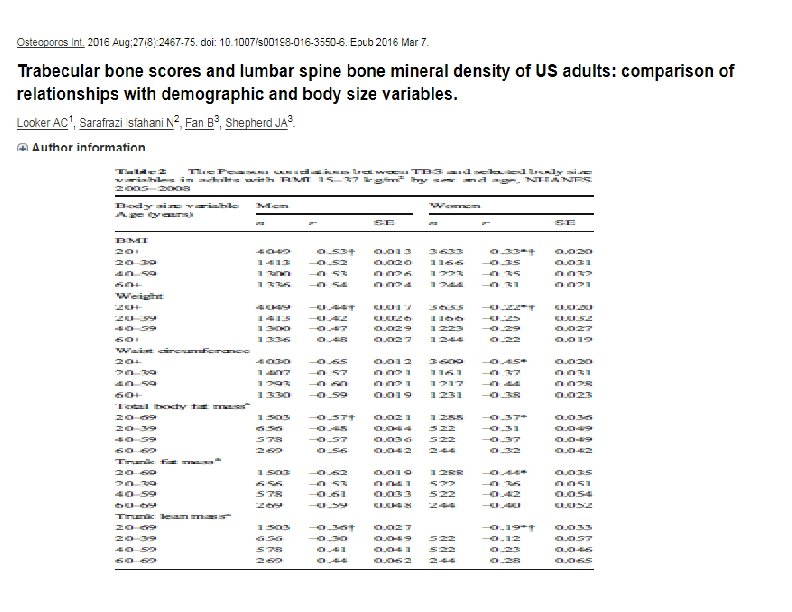

• This study examines demographic patterns and body size relationships in trabecular bone score and lumbar spine BMD of US adults from NHANES 2005– 2008 . • The analytic sample used in the present study consisted of 7682 adults aged 20 years and older. • TBS was negatively correlated with BMI, weight, waist circumference, total body fat mass, trunk fat mass, and trunk lean mass in all sex and age groups. • Results of the sensitivity analyses designed to assess the impact of BMI exclusions for TBS revealed that mean TBS values among those with BMI >37 kg/m 2 were approximately 26% lower in men and 15% lower in women than mean TBS in those with BMI between 15 and 37 kg/m 2 (p< 0. 001 for both sexes) TBS software have not recommended the use of TBS in individuals with BMI lower than 15 kg/m 2 or greater than 37 kg/m 2.

Endocrinol Metab Clin North Am. 2017

14 cross sectional OR All FX: 1. 95 V. Fx: 2. 66 VFx: 1. 9 VFx: 3. 8 HF: 1. 66 Any: 2. 36 VF: 2. 44 Any: 1. 3 VF: 1. 7 MOF: 1. 6 Any: 1. 28

OR Any: 1. 27 Any: 1. 83 Vfx: 1. 23 Non Vfx: 1. 42 Any: 1. 55

11 prospectove HR/ OR MOf: 1. 17 Vfx: 1. 14 Hf: 1. 47 Any: 1. 34 Vfx: 1. 52 Vfx: 1. 62 (clinical) 1. 54 (radiogr aphy)

HR/ OR MOF: 1. 17 Any: 1. 87 At least 1 MOF: 1. 18 HF: 1. 23 Death: 1. 20 MOF: 1. 08 VF: 1. 02 HF: 1. 44 MOF: 1. 76 MOF: 1. 27 HF: 1. 20 MOF: 1. 32 HF: 1. 28

• pool of 441 Caucasian, postmenopausal women between the ages of 50 and 80 years, we identified 42 women with osteoporosis-related vertebral fractures, and compared them with 126 age-matched women without any fractures (1 case: 3 controls)
 in")
Subgroup analyses for women with osteopenia Fifty-one of the 168 women (30. 4%) in the study, 11 of the 42 (26. 2%) in the fracture group, and 40 of the 126 (31. 7%) in the control group were found to have a T-value between − 1. 0 and − 2. 50, so that they were considered to have osteopenia, according to DXA data. The two groups did not differ but did differ in TBS (0. 932 vs. 1. 065, p=0. 0296)

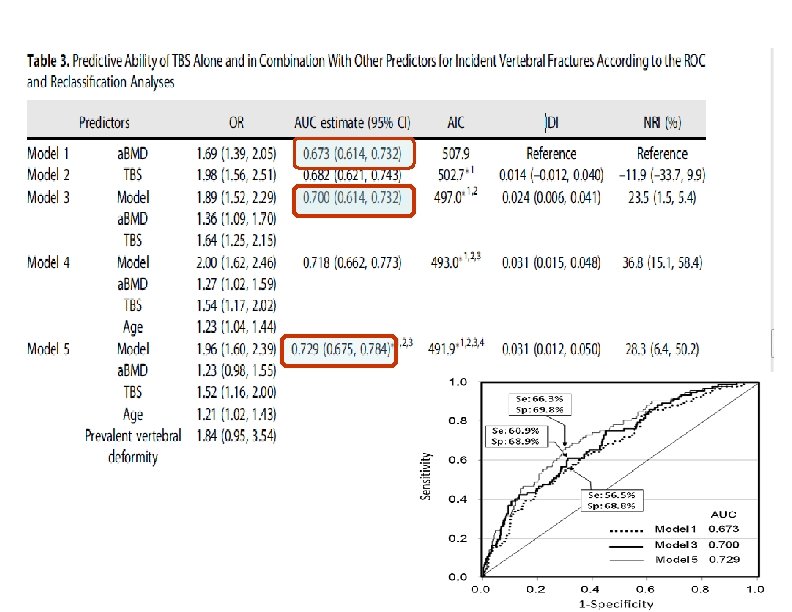
Subgroup analyses for women with osteoporosis Also among the 168 subjects, there were 117 (69. 6%) who met the T-score criteria for osteoporosis, with a T-score less than − 2. 5: 31 of the 42 (73. 8%) in the fracture group and 86 of the 126 (68. 3%) in the control group. The groups did differ in both BMDa (0. 799 vs. 0. 882, p=0. 0008) and TBS (0. 903 vs. 1. 047, pb 0. 0001). The odds ratio for fracture was 2. 43 (1. 49– 3. 95) for each incremental decrease in BMDa, 3. 36 (1. 90– 5. 92) for each incremental decrease in TBS, and 4. 04 (2. 35– 6. 92) for each incremental decrease in (TBS + BMDa). The AUC again was statistically higher for (TBS + BMDa) (0. 835, 0. 755– 0. 897, vs. 0. 718, 0. 627– 0. 797; p=0. 013).
")
A comparison of TBS versus BMDa versus TBS plus BMDa TBS BMD TBS+BMD (a) Area under the receiver operating curves for bone mineral density (BMDa, the grey curve) and trabecular bone score (TBS, the dark curve). (b) Area under the receiver operating curves for bone mineral density (BMDa, the grey curve) and the combinedand trabecular bone score plus BMDa (TBS + BMDa, the dark curve).

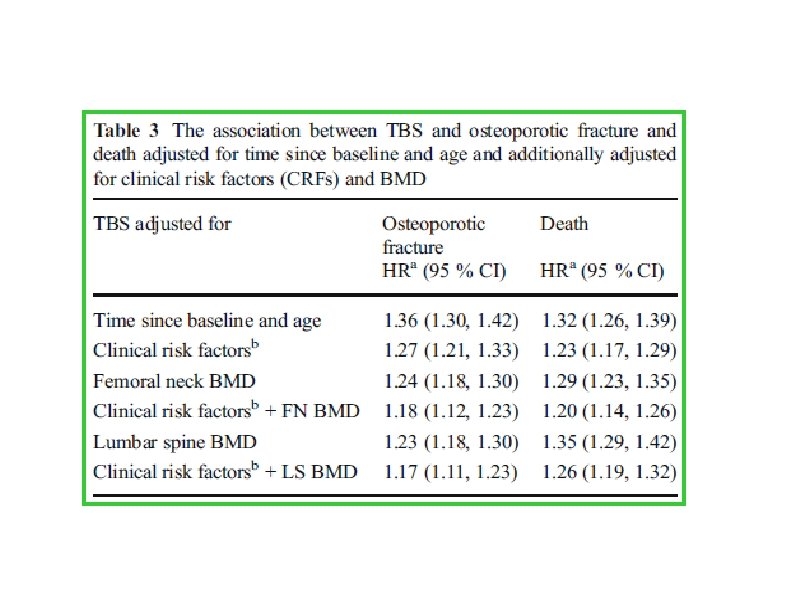
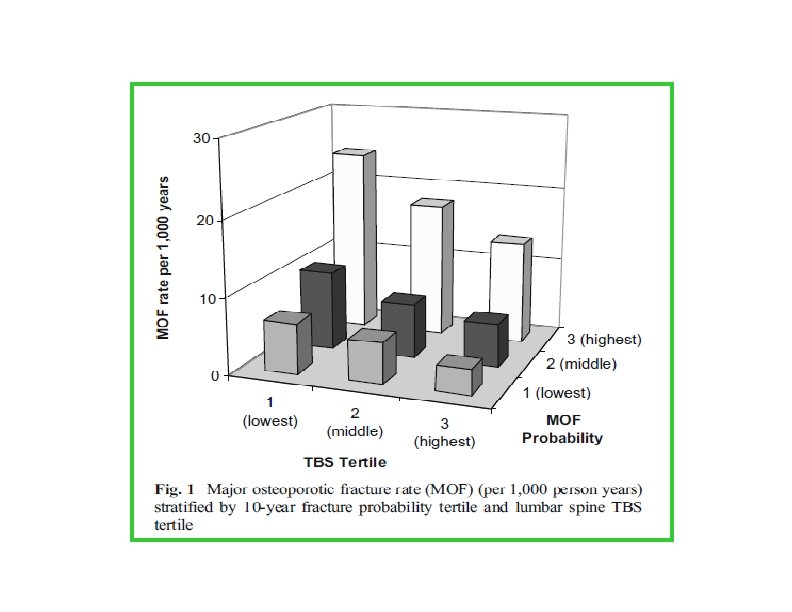
International Osteoporosis Foundation and National Osteoporosis. Foundation 2014 • retrospective cohort study from a large clinical registry for the province of Manitoba, Canada • We included 33, 352 women aged 40– 100 years (mean 63 years) with baseline DXA measurements of lumbar spine TBS and femoral neck BMD. The association between TBS, the FRAX variables, and the risk of MOF or death was examined • The mean observation period was 4. 7 years

Study population baseline characteristics

The association between each potential risk factor and osteoporotic fracture and death adjusted for time since baseline and age a: HR per SD decrease
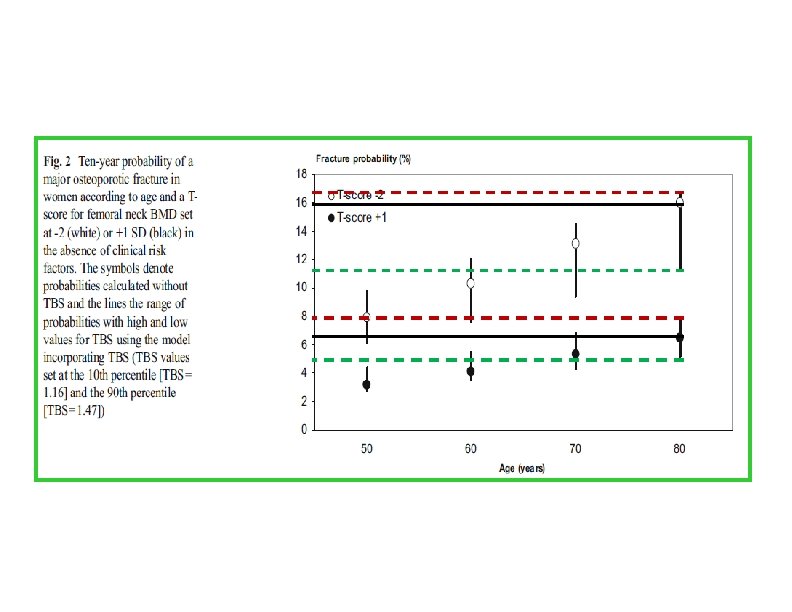

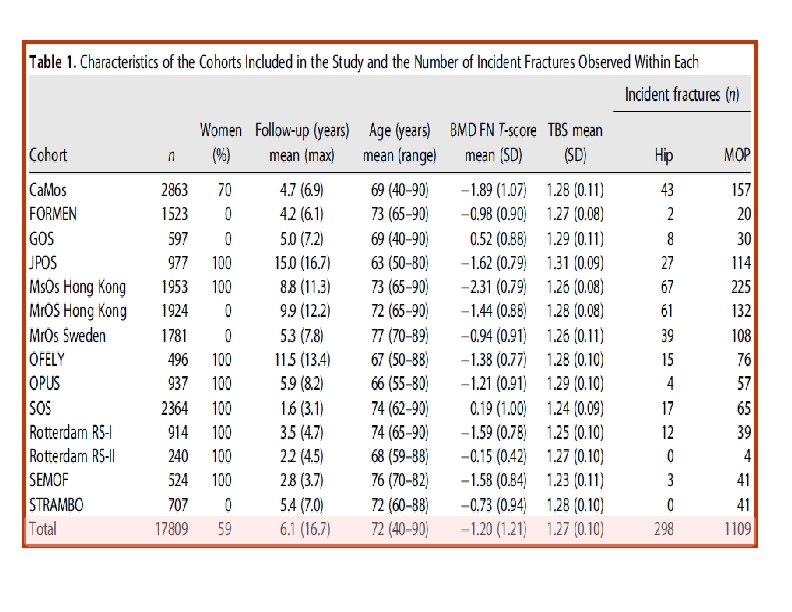
et al. Journal of Bone and Mineral Research, 2016 • • Cohorts studied used baseline and follow-up data from 14 prospective population-based cohorts
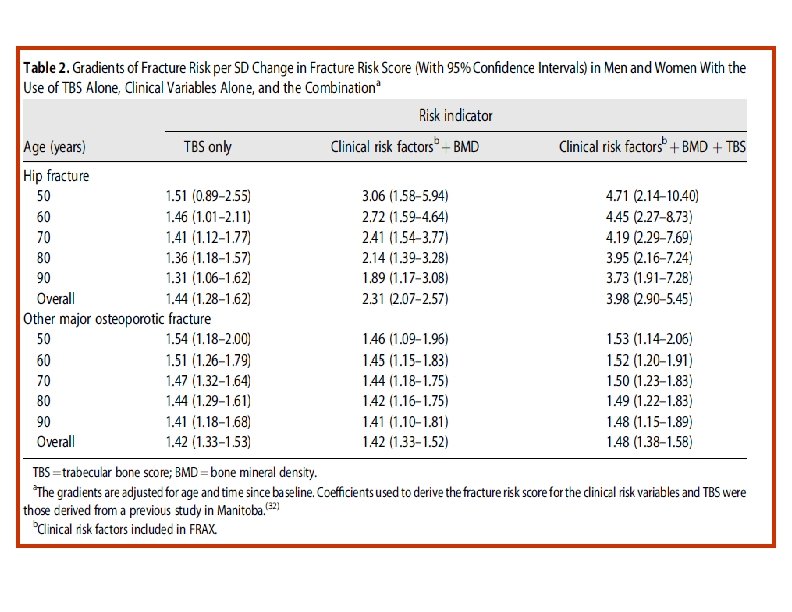
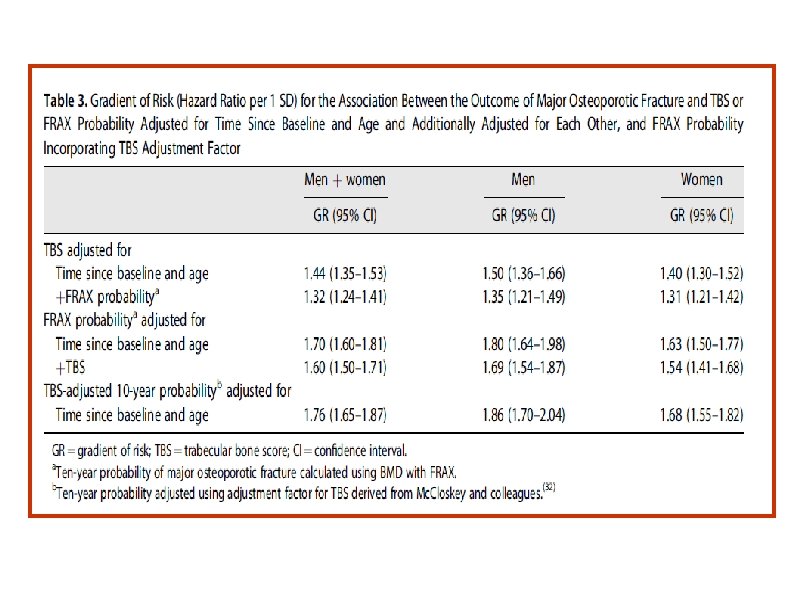
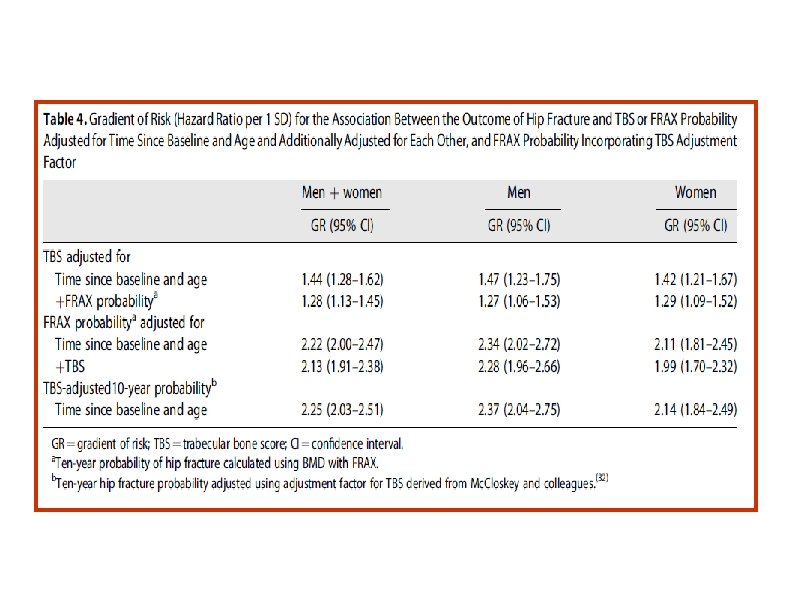

• The findings of the study support the use of TBS, not only as a standalone assessment of fracture risk but also, more importantly, as an independent contributor to a more global risk assessment that could permit its use along side established risk assessment tools such as FRAX. • This was reflected in the higher GRs and AUCs when TBS was combined with the FRAX clinical risk factors and BMD, particularly for hip fracture outcomes

2014 American Society for Bone and Mineral Research

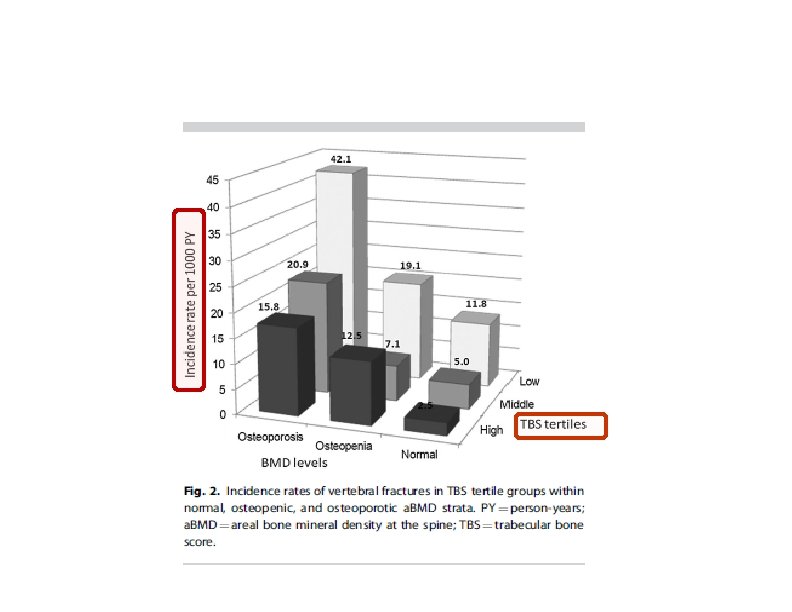
Flowchart of subject recruitment and follow‐up

Baseline Characteristics of Participants With and Without Vertebral Fractures During the 10‐Year Follow‐up

Comparison of TBS at Baseline Between Participants With and Without Incident Vertebral Fractures During the 10‐Year Follow‐up
 ≥ 40 y &")
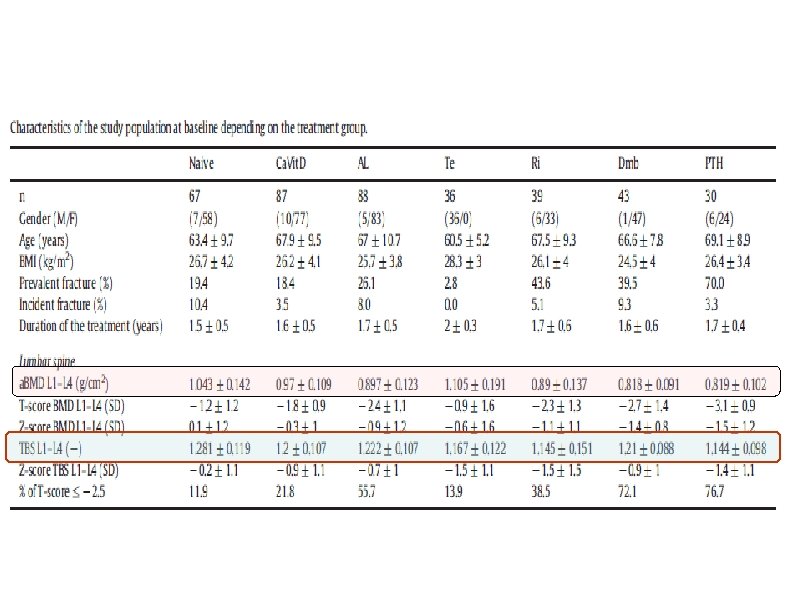
• • • 390 subjects(318 women and 72 men) ≥ 40 y & BMI between 15 and 37 kg/m 2 25. 1% sustained at least an osteoporotic fracture Subjects were stratified using their fracture status (with fracture, without fracture) and using the treatment status (with and without treatment) as well as treatment group: Calcium and Vitamin D (Ca. Vit. D), Testosterone (Te), Alendronate (Al), Risedronate (Ri), Denosumab (Dmab) and Teriparatide (PTH) mean follow-up of 20 months. Drug Doses: • • • Ca. Vit. D : Calcium(2500 mg) and Vitamin D 3 (880 IU) daily Teriparatide: 20 μg Dmab received 60 mg one per six months ALN : 70 mg /w or Risedronate 5 mg/d 36 men (had Testosterone deficiency) treated with, 50 mg of Testosterone gel daily, applied in the morning.
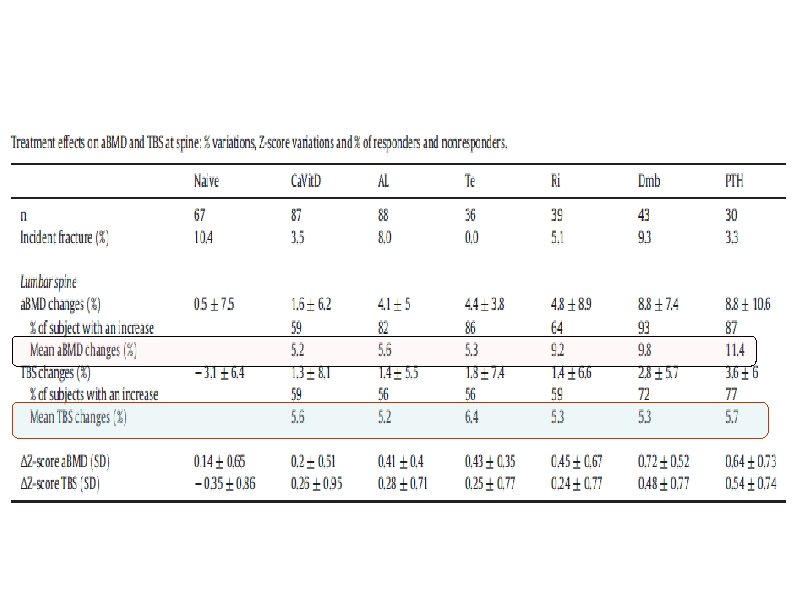

a. BMD and TBS variations after 24 months of follow-up *, **and *** were p ≤ 0. 05, p ≤ 0. 01 and p ≤ 0. 001 respectively.
 Objective: This study evaluated the ability")
(J Clin Endocrinol Metab 98: 602– 609, 2013) Objective: This study evaluated the ability of lumbar spine TBS to account for increased fracture risk in diabetes. Design and Setting: We performed a retrospective cohort study using BMD results from a large clinical registry for the province of Manitoba, Canada. Patients: We included 29, 407 women 50 years old and older with baseline DXA examinations, among whom 2356 had diagnosed diabetes.
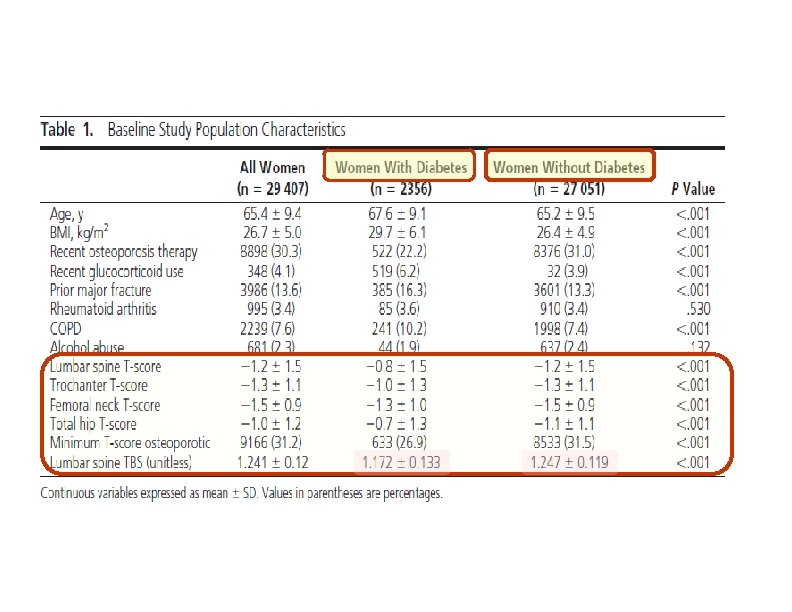
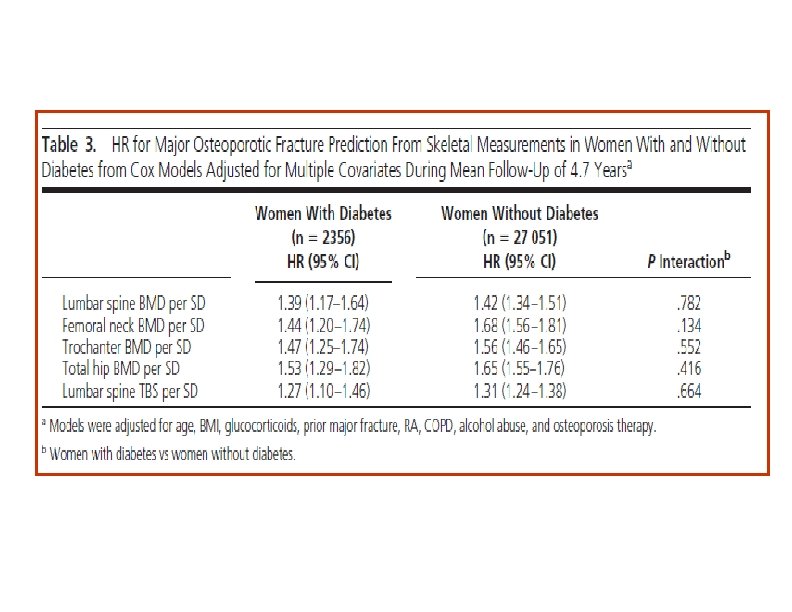
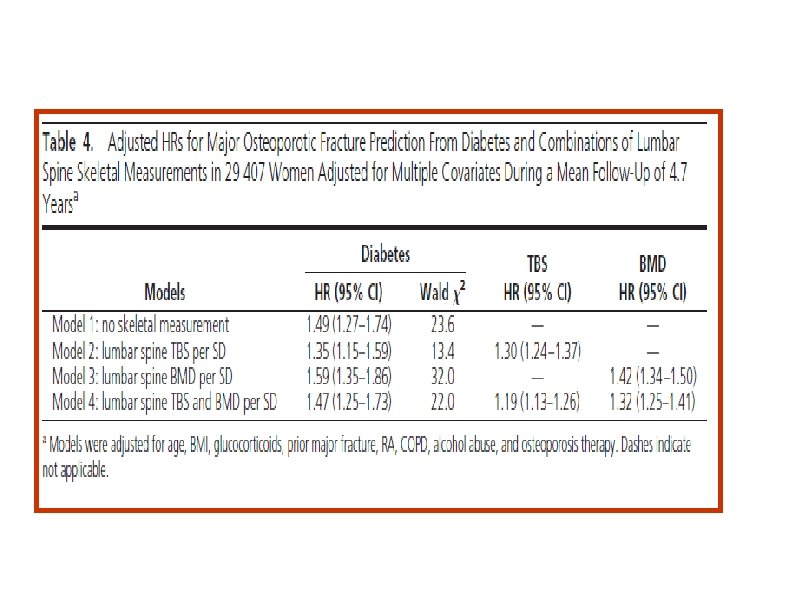

• In this large clinical cohort of women, we found that diabetes was associated with higher BMD measurements, whereas lumbar spine TBS was associated with lower measurements. • Lumbar spine TBS captures some of the fracture risk associated with diabetes. In contrast, because BMD measurements are paradoxically higher in the women with diabetes despite higher fracture risk, BMD measurements actually confound this relationship. • The mechanisms for increased fracture risk : High glucose levels in diabetes lead to accumulation of advanced glycosylation endproducts in the organic bone matrix and advanced glycosylation end-products cross-links lead to biomechanically more brittle bone

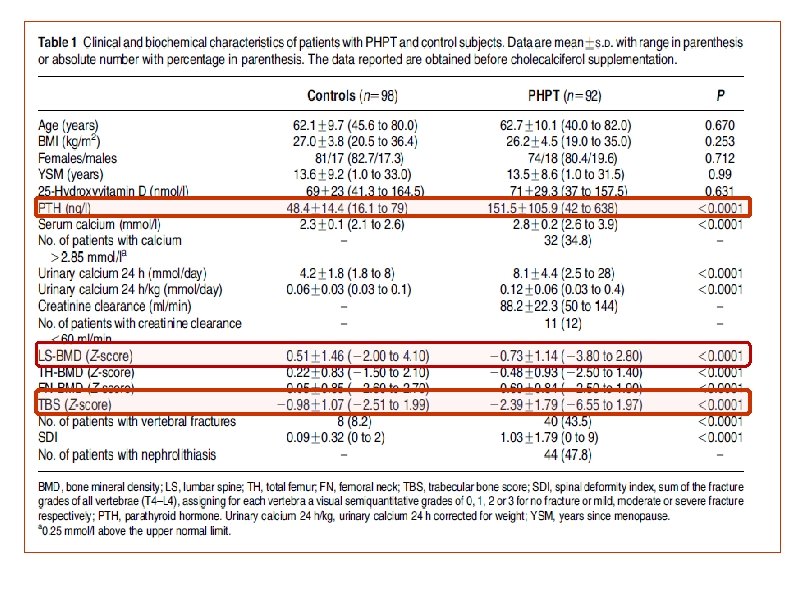
• Design: • 92 PHPT patients (74 females, age 62. 1± 9. 7 years) and 98 control. • In all patients at baseline, in 20 surgically treated patients and in 10 conservatively treated patients after 24 months, TBS, spinal (lumbar spine (LS)) and femoral (total hip (TH) and femoral neck (FN)) BMD were assessed by DXA and VFx by spinal radiograph.

3 experiencing a. VFx duringthe follow-up

• The aim of this study was to evaluate the usefulness of TBS alone or in combination with BMD for predicting VFx in asymptomatic PHPT patients before and after surgery or a conservative follow-up.

How Can TBS Be Used in Clinical Practice? . Use of Trabecular Bone Score (TBS) as a Complementary Approach to Dual-energy X-ray Absorptiometry (DXA) for Fracture Risk Assessment in Clinical Practice. Enisa Shevroja et al. ISCD 2017

ISCD Official Position Ø TBS is associated with vertebral, hip, and major osteoporotic fracture risk in postmenopausal women Ø TBS should not be used alone to determine treatment recommendations in clinical practice. Ø TBS can be used in association with FRAX and BMD to adjust FRAX-probability of fracture in postmenopausal women and older men. Ø TBS is not useful for monitoring bisphonate treatment in postmenopausal women with osteoporosis. Ø TBS is associated with major osteoporotic fracture risk in postmenopausal women with type 2 diabetes.

conclusions ü TBS is very useful during the whole patient management process, helping in decision making for diagnosis, treatment and patients' follow-up care ü Enables to complete the diagnosis by adding an estimation of bone microarchitecture to the tools we are already using the estimation of density (BMD) and estimation of future fracture (FRAX®) ü When the diagnosis of a patient's bone status is clear, TBS is reassuring. When you have cases where the decision to treat or not is equivocal, which we often do, TBS clearly brings added valuable information to identify patients at risk. ü The TBS is useful in following the patient's progress over time, and it is a tool that allows to verify the impact of the selected treatment on a patient's bone structure.
- Slides: 62