Tatum Bone Expansion Illustrations Indication for Bone Expansion

Tatum Bone Expansion Illustrations

Indication for Bone Expansion n Bone expansion techniques for dental implant placement were developed by Dr. Hilt Tatum in 1970 and are proven to be an efficient alternative to block and particulate grafting for patients who have adequate bone height but insufficient width to allow implant placement.

Bone Expansion Advantages Cost effective n Reduces treatment time n Conserves precious bone cells n Eliminates difficult soft tissue closures n Restores labial contours n


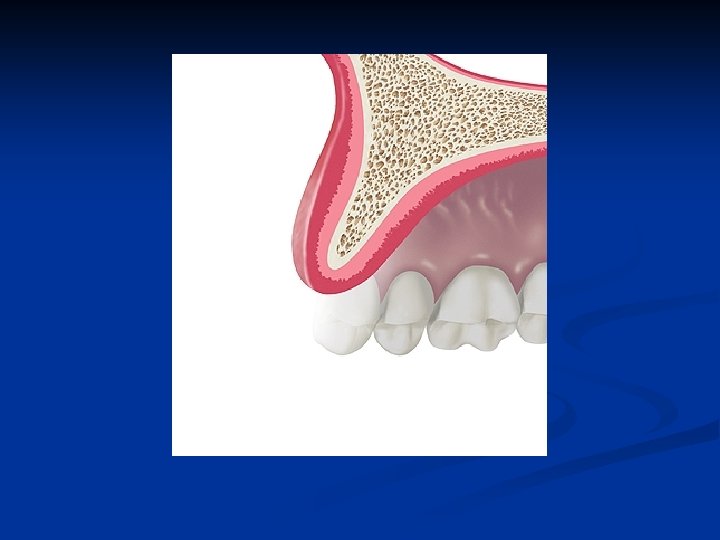
The frontal view of the edentulous segment of the maxillae demonstrates bone of adequate height and unknown width
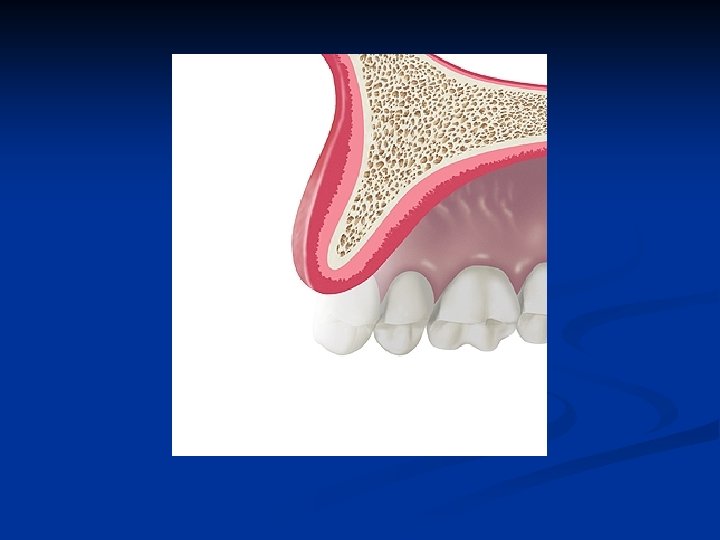

The sagittal view of the edentulous segment of the maxillae demonstrates bone of inadequate thickness to allow conventional rotary cutting instruments to be used
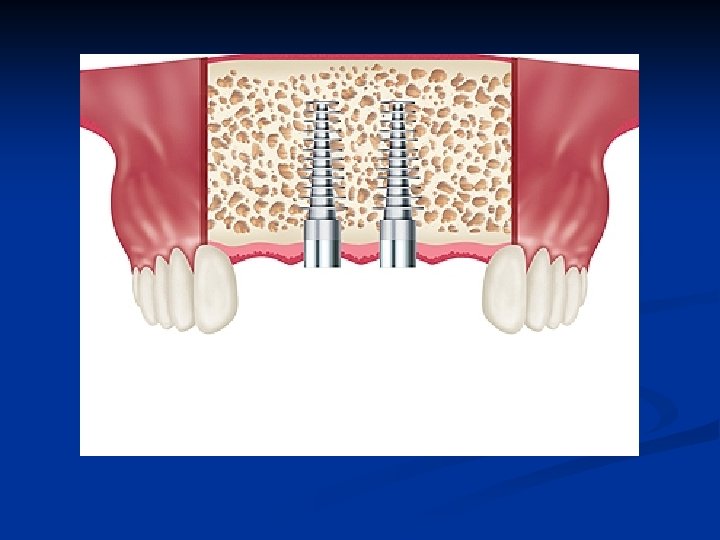

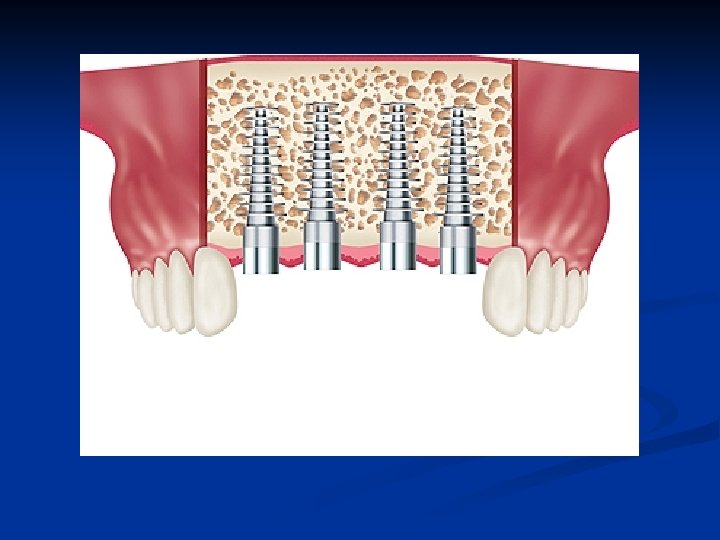
Bone Expansion for the Maxillary Anterior Segment n The median palatine suture is a factor n Implants may be placed in the central incisor positions only at the initial surgery n Implants may be added to the lateral incisor positions 6 wks following the initial placements

Aggressive bone expansion in an attempt to place adjacent implants in thin ridges will likely result in failure due to labial plate fracture

Implants are generally allowed to heal for 6 months in the maxillae and 4 months in the mandible prior to loading when utilizing bone expansion techniques

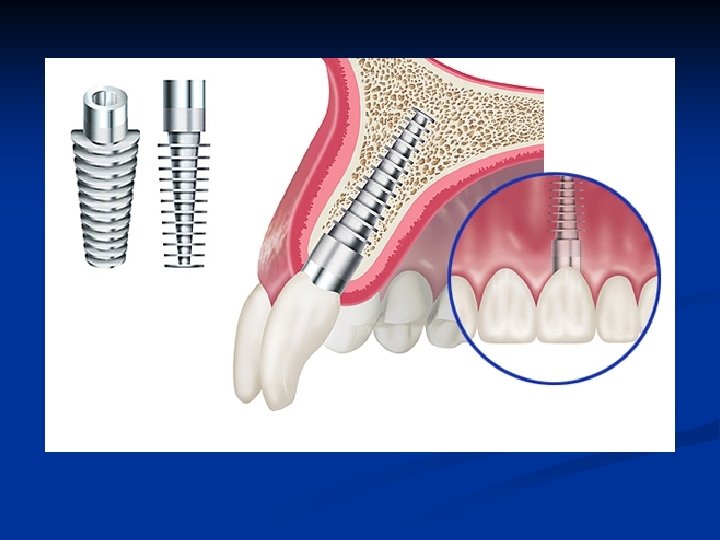
Sagittal View n n Single stage surgery Plateau or fins in bone Grit-blasted surface may be in bone or soft tissue Polished collar surface transmucosal

Illustrated Prosthetic Results Conventional crown and bridge methods n Normal gingival contours n Normal occlusal relationships n
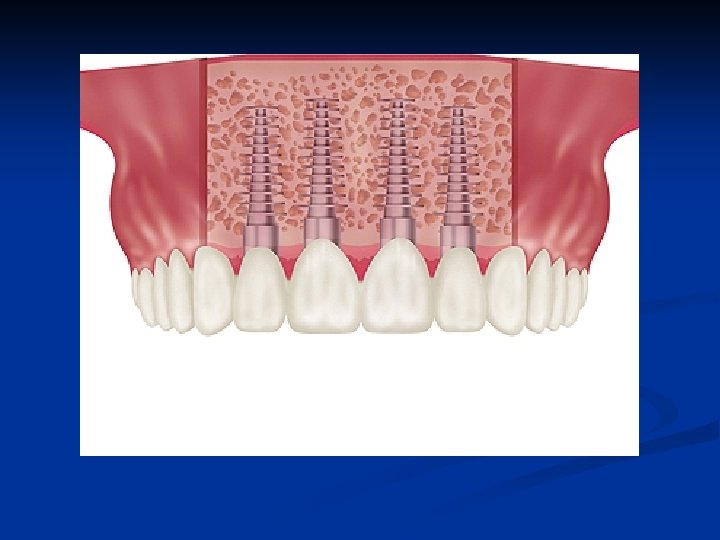

Restored “D” elliptical implant Normal gingival contour n Normal tooth anatomy n Maximum boneimplant surface area n

The following diagrams and text describe basic bone expansion technique. Contact Tatum Surgical @1 -888 -360 -5550 for educational workshops with hands on training

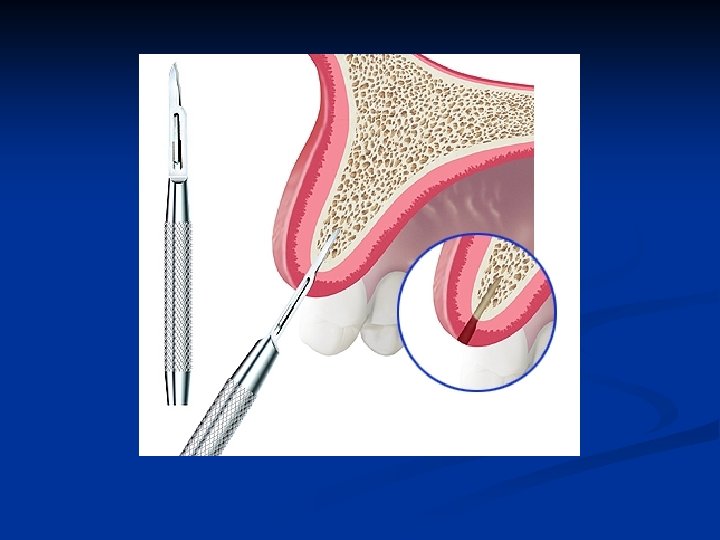
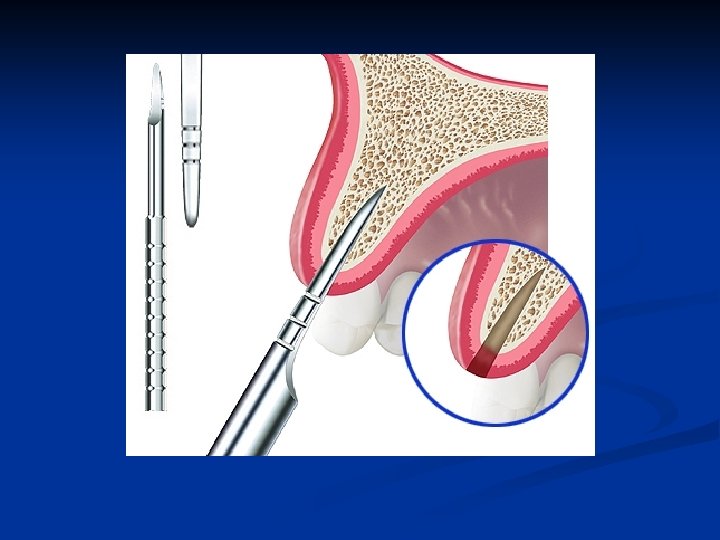
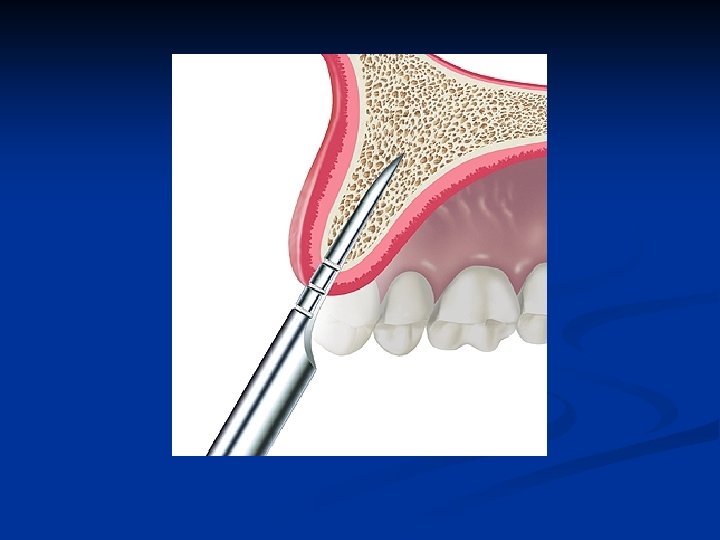
Bone Expansion Technique Atrophic ridges as thin as 1 mm at the labio-palatal crest may be expanded n A #11 scalpel blade is utilized to bisect the crestal bone n


Bone entry with a scalpel Carefully done to bisect the labial and palatal bone n The cortical bone must be penetrated to gain access to the interstitial bone n
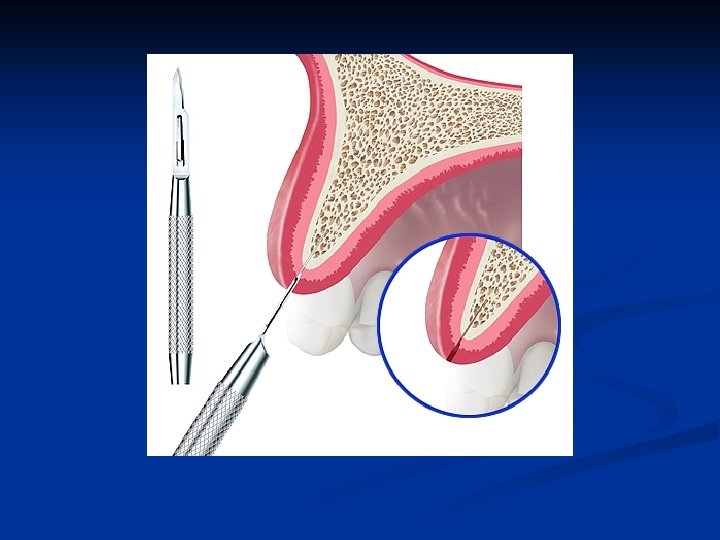

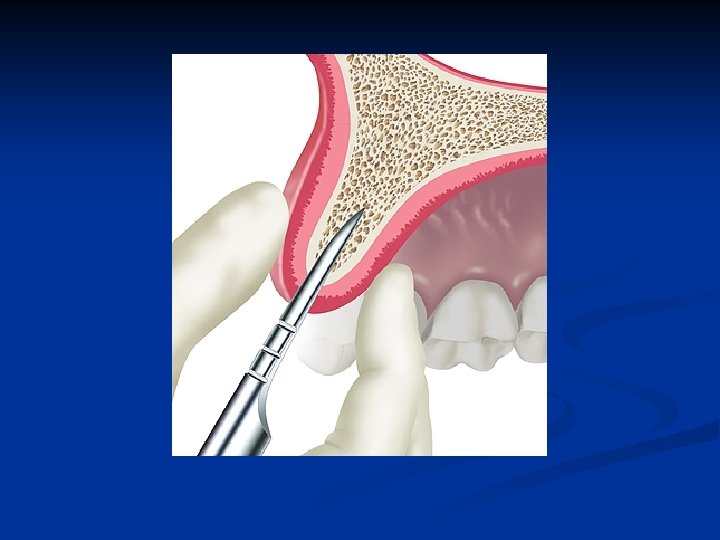
Bone expansion scapel technique n n Follow the long axis of the bone to further penetrate and gain access to the medullary bone These are gentle procedures done with controlled force

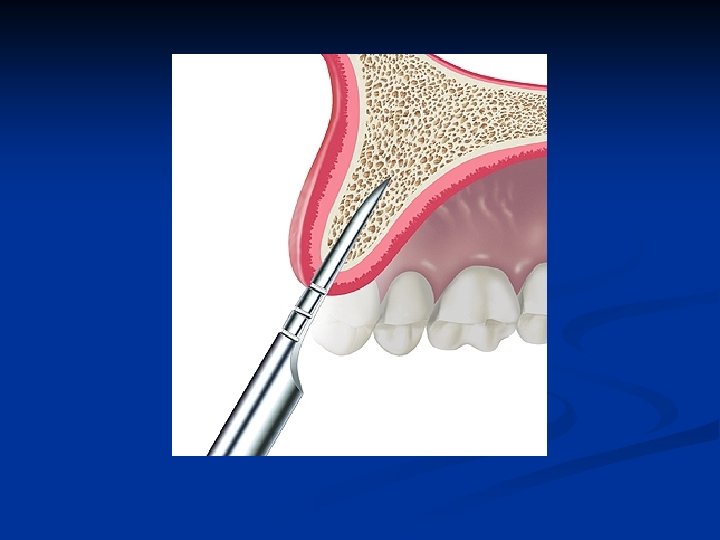
Scalpel removal from bone Always rotate the scalpel mesialdistal with a gentle removing force n Never rotate the scalpel labiopalatal n

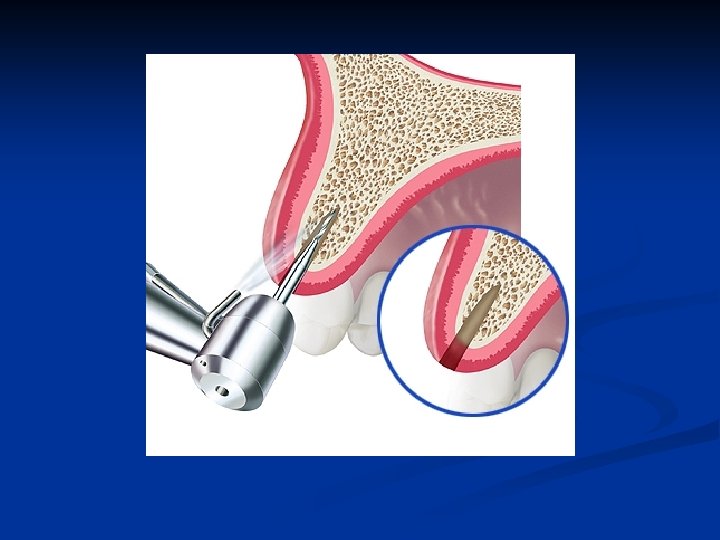
Bone expansion access n A high-speed handpiece using a thin tapered diamond may be used following scalpel access to the medullary bone if it is hard and cortical in nature

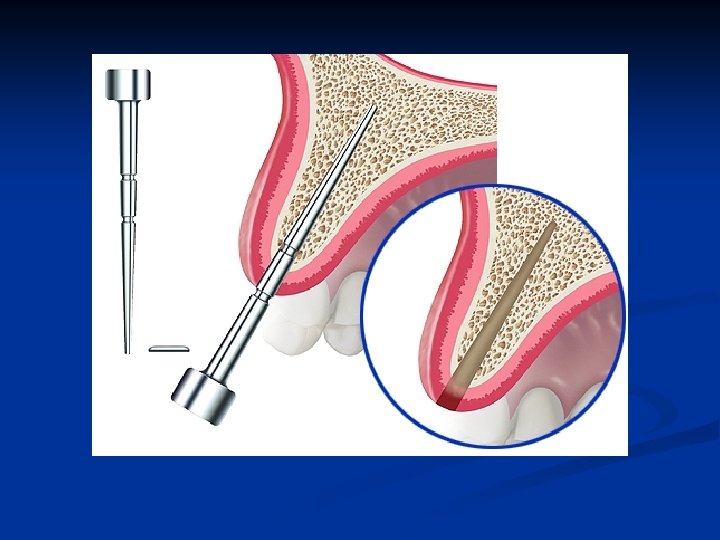
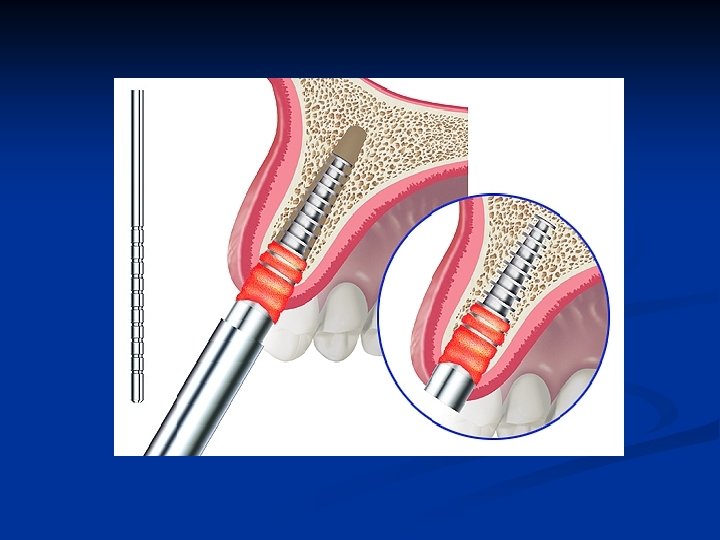
Bone expansion instruments The smallest dimension bone expander is inserted in the osteotomy n It is extremely important to expand the bone in the correct vertical axis n
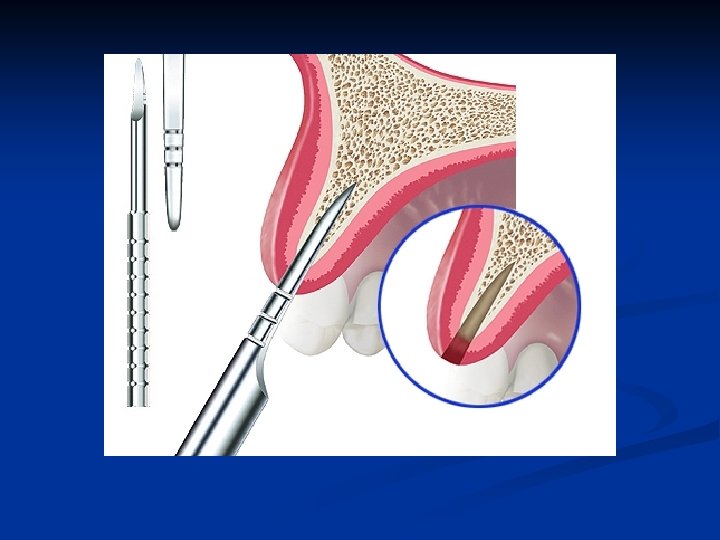

Prevent labial plate bone fracture n n Palatal bone is not plastic and does not expand Carefully brace the labial bone with fingerthumb pressure as the expansion instruments move the bone labially and open the osteotomy



Expansion instrument removal Always remember to remove bone expansion instruments with a gentle, mesialdistal controlled action. n Never apply a labio-palatal removal action n

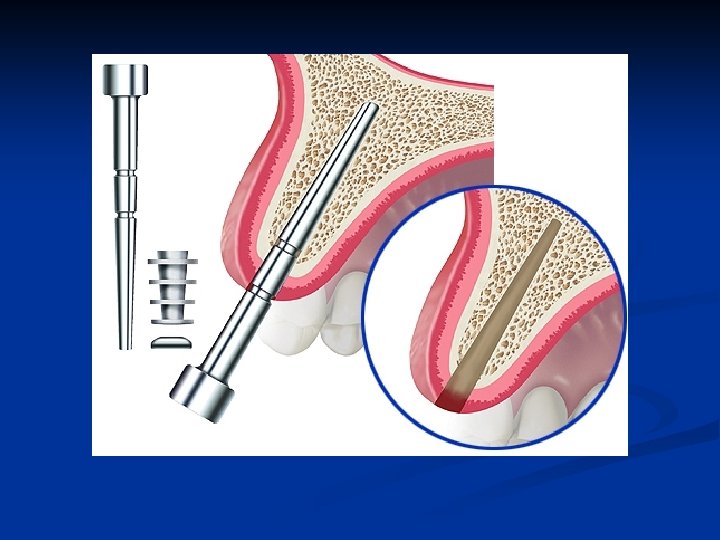

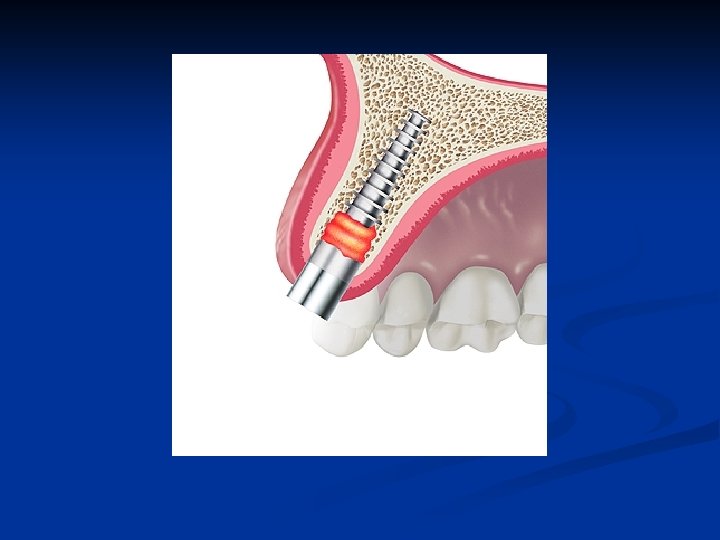
Final size bone socket former n The osteotomy expansion is completed to depth with a bone socket former sized exactly as the implant to be inserted

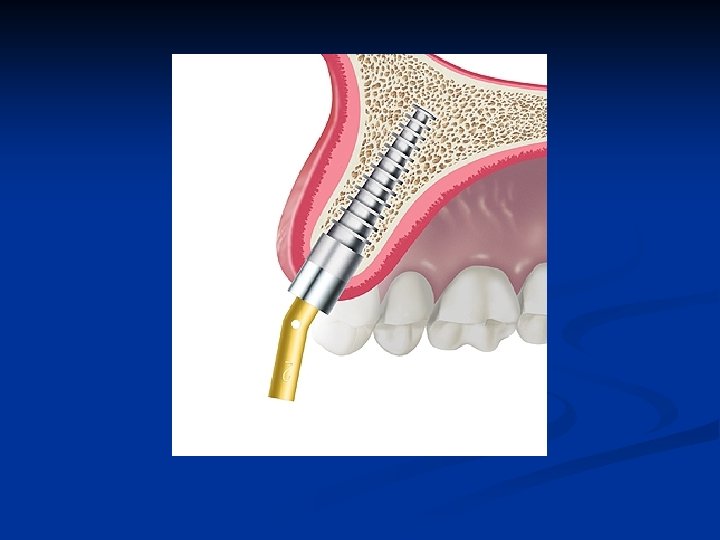
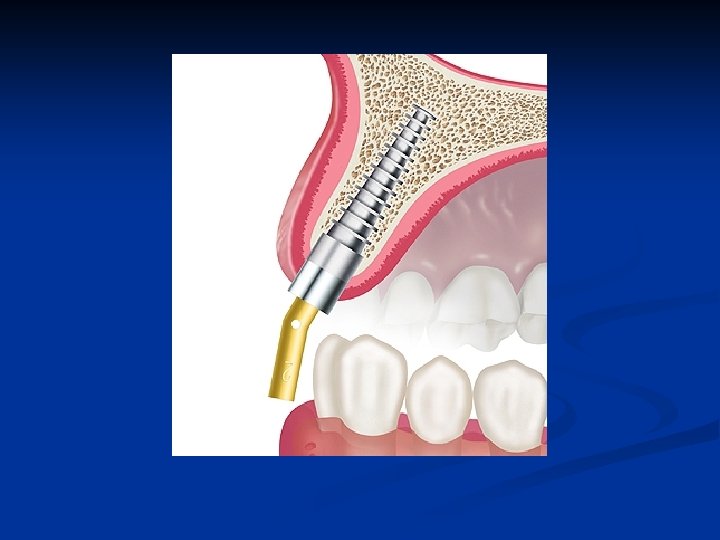
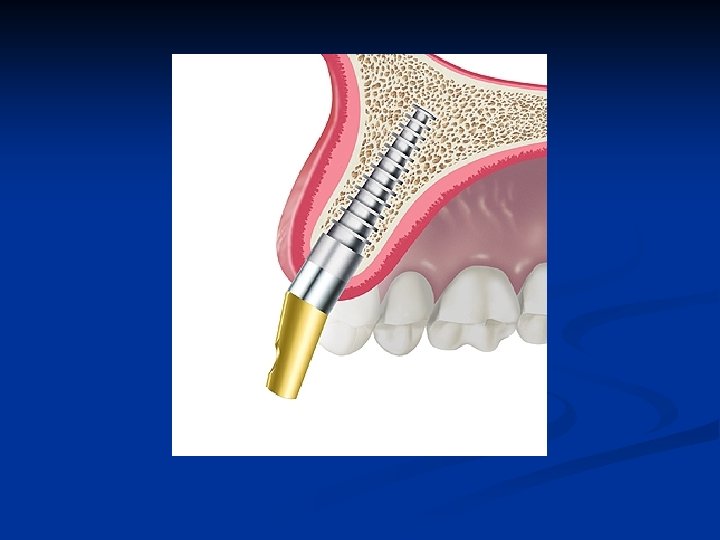
Osteotomy depth measurement n Each instrument used for bone expansion has depth markings to indicate the exact implant length and location of the grit blasted collar


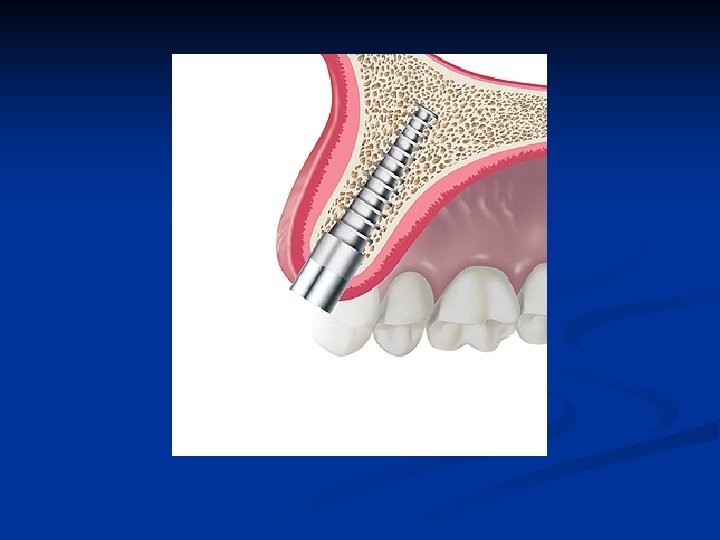
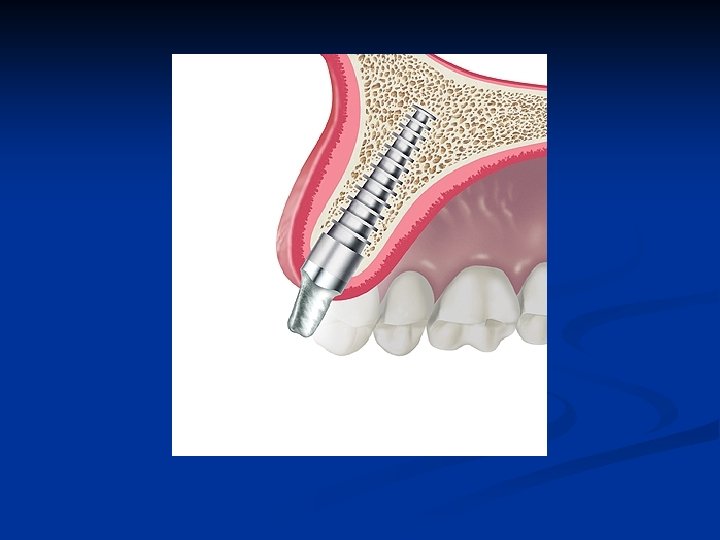
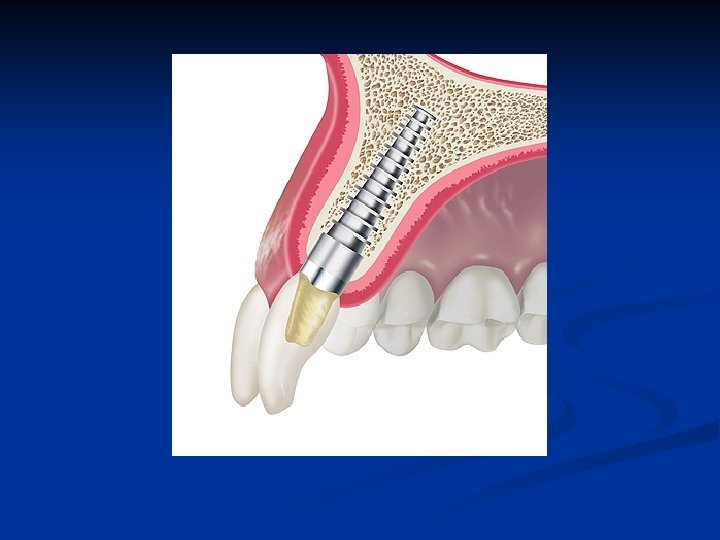
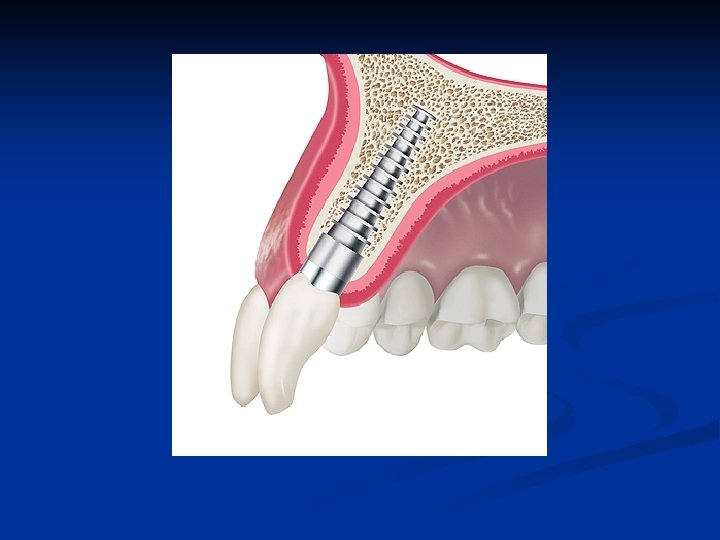
Bone expansion implant seating Utilize the provided seating instrument n Gently drive the implant into the full depth of the expanded osteotomy n

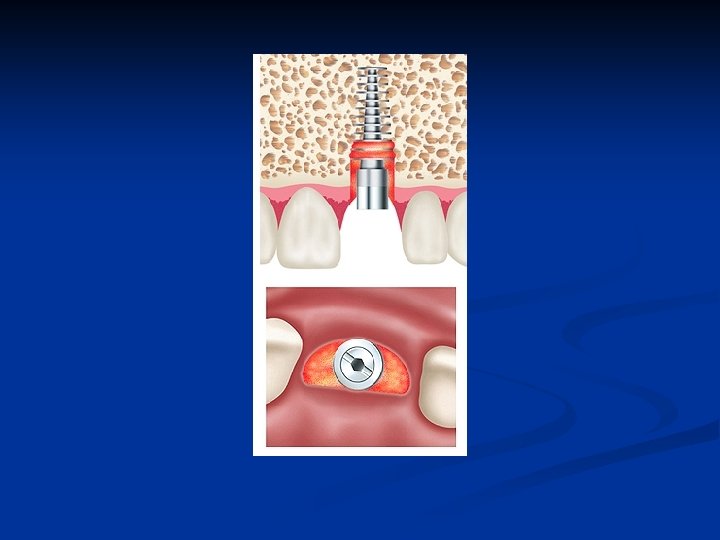
Sagittal view of Osteogen barrier n Slowly resorbable Osteogen is mixed with the patient’s blood to provide a barrier against epithelial migration into the osteotomy

Frontal-crestal view of “D” implant n n View of completed surgery of elliptical implant place with bone expansion osteotomy. Osteogen mixed with the patient’s blood is utilized as a barrier to prevent epithelial migration during initial healing

Sagittal view healed “D” implant n n n Single stage transmucosal Plateau fins must be in bone Grit-blasted surface relationship to bone height is determined by the thickness of the soft tissue

Post guide try-in n n Post guides of 0, 10, 20, 30 degrees are available in the surgery kit to predetermine abutment post selection Enter this information in the record at the time of surgery

Evaluate the opposing dentition n The implant position must allow the restored implant to have a non-traumatic occlusal relationship with the opposing teeth or prosthesis

Abutment post cementation n Read and understand the instruction manual on this website for cementation of the unique Tatum Unipost

Abutment post preparation n n Gross reduction of the abutment post may be done using the post holder tool outside of the mouth Final preparation and paralleling is done following cementation of the abutment post

Preparation requirements The margin of the preparation Must extend onto the body of the implant n A small anti-rotational grove is extended onto the body of the implant n Margin placement is determined by the soft tissue contour and the planned emergence profile of the final restoration n

Abutment selection & preparation n n Prepare abutments to allow normal contour for anatomically correct prosthetics Prepare abutments to allow proper material dimensions for strength and longevity of restorations

Sagittal view of restored implant Physiologic contour n Normal emergence profile n Maintainable bone -circumferential soft tissue complex n

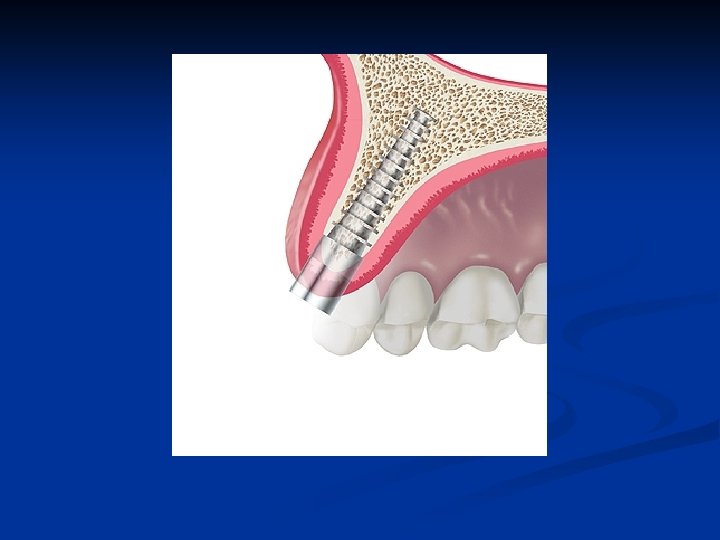
Single anterior implant Single anterior

“D” implant in cuspid pillar

“D” Posterior bridge abutments
- Slides: 69