Targeting Antibiotic Prescribing for Respiratory Tract Infections RTI
 Facilitated learning session Part 1 ‐")
Targeting Antibiotic Prescribing for Respiratory Tract Infections (RTI) Facilitated learning session Part 1 ‐ How do I decide when to prescribe antibiotics? Part 2 ‐ Strategies to reduce unnecessary antibiotic prescribing

Session Aim To support prescribers to understand when antibiotics should be prescribed for RTI, and when alternative approaches can be used Objectives Understand the benefit versus risk of prescribing for common RTIs Use validated scoring systems to support prescribing decisions Identify strategies that can be used to reduce unnecessary prescribing Improve ‐ Identify areas for improvement and formulate an action plan

Targeted use of antibiotics “Our mission is not to prescribe as few antibiotics as possible, but to identify that small group of patients who really need antibiotic treatment and to explain, reassure and educate the large group of patients who don’t. ” Verheij TJM. The antibiotic revolution should be more focused. Br J Gen Pract 2009; 59(567): 716‐ 717

The case for further reducing unnecessary antibiotic use

Unnecessary Use in RTIs Q 1 What % of antibiotics does data suggest are prescribed unnecessarily? Q 2 Have you ever felt you prescribed an antibiotic for RTI when it might not have been necessary? Q 3 Why do you think this was?

How many could have got better on their own?

How do you compare? Have a look at your prescribing data compared to you peers Variability in total volume of prescribing amongst GP practices in NHS Scotland Source: Information Services Division (ISD) www. isdscotland. org/Health‐Topics/Prescribing‐ and ‐Medicines/Publications/2016‐ 08‐ 30‐SAPG‐ 2015‐Report. pdf?

Consequences of Prescribing ‘Just in Case’ • • Results in repeat consultations 1 = higher workload! Reinforces patient belief in antibiotics 2 Can undermine your colleagues Exposes patient to harm • Resistance • Healthcare Associated Infection (HAI) • Adverse effects (GI, rash, tendon damage, allergic reaction, QT prolongation. . . death? ) • Drug and food interactions 1. Little P et al. Reattendance and complications in a randomised trial of prescribing strategies for sore throat: the medicalising effect of prescribing antibiotics’ BMJ 1997; 315 350‐ 352 2. Little P et al. Delayed antibiotic prescribing strategies for respiratory tract infections in primary care: pragmatic, factorial, randomised controlled trial BMJ 2014; 348

Consequences of Prescribing ‘Just in Case’ Otitis Media Rhinosinusitis For every 14 people treated, 1 will suffer an adverse effect (≈7 in 100) For every 8 people treated 1 will suffer an adverse effect (≈12‐ 13 in 100) Key No adverse effect Adverse effect Venekamp RP et al. Antibiotics for acute middle ear infection (acute otitis media) in children. Cochrane Database of Systematic Reviews. Published June 2015. Lemiengre MB et al. Antibiotics for clinically diagnosed acute rhinosinusitis in adults. Cochrane database for systematic reviews. Published Oct 2012.

Is it safe to reduce antibiotic prescribing? • Scottish prescribing and admission data (2010‐ 2014) linked using infection intelligence platform (IIP), showed no evidence that serious bacterial infections* have increased despite a reduction in primary care of antibiotic prescribing 1 • In Sweden the STRAMA§ programme also found no negative consequences from reducing antibiotic use 2 • Provides reassurance that reduction in unnecessary use is possible without unintended consequences *peritonsillar abscess, mastoiditis, community acquired pneumonia §Swedish Strategic Programme for the Rational Use of Antimicrobial Agents and Surveillance of Resistance 1. ISD Scotland. Measuring Potential Unintended Consequences of Interventions to Reduce Primary Care Antibiotic Use (published online 2016) http: //www. isdscotland. org/Health‐Topics/Health‐and‐Social‐Community‐Care/Infection‐Intelligence‐Platform/Communications/_ docs/Study‐ 7 b ‐Poster. pdf 2. Molstad S et al. Sustained reduction of antibiotic use and low bacterial resistance: 10‐year follow‐up of the Swedish Strama programme. Lancet 2008; 8 (2): 125‐ 132 http: //www. thelancet. com/journals/laninf/article/PIIS 1473‐ 3099(08)70017‐ 3/abstract

Part 1 ‐ How do I decide when to prescribe antibiotics for RTI*? Quantifying risk versus benefit Using scoring to support decisions *Sore throat, Rhinosinusitis, Otitis Media, Cough

Upper Respiratory Tract Infection Sore throat Rhinosinusitis Otitis Media

Acute Sore Throat When might antibiotics be required? Q 1 How do you currently decide whether or not to give antibiotics? Q 2 How long do you think it takes for most cases to resolve without treatment? Q 3 What do you think are the benefits (if any) of giving antibiotics?

Sore throat – Risk in Perspective Quinsy • Overall NNT > 4000 to prevent one case of quinsy 1 • Even if centor score of 3 or 4 = 1: 60 chance of quinsy 2 Rheumatic Fever • It would take 12 working life times of a GP to see one case of Rheumatic Fever 3 • Treating sore throats with antibiotics has no effect on risk of developing Rheumatic Fever 3 Otitis Media • Antibiotics to prevent otitis media NNT 2004 Glomerulonephritis • Rare condition (2. 1 per 100, 000 children) ‐ not prevented by treating sore throats with antibiotics 5 1. Peterson et al. Protective Effects of antibiotics. BMJ 2007; 335: 982‐ 984 2. Centor et al. The diagnosis of Strep throat in adults in the emergency room. Med Decision Making 1981; 1: 239‐ 46 3. Howie et al. Antibiotics, sore throat and rheumatic fever. BJGP 1985; 35 : 223‐ 224 4. Spinks et al. Antibiotics for sore throat. Cochrane database for systematic review issue 4 2006 (2008 content review) 5. Taylor et al. Antibiotics, sore throat and acute nephritis. BJGP 1983; 33 : 783‐ 786

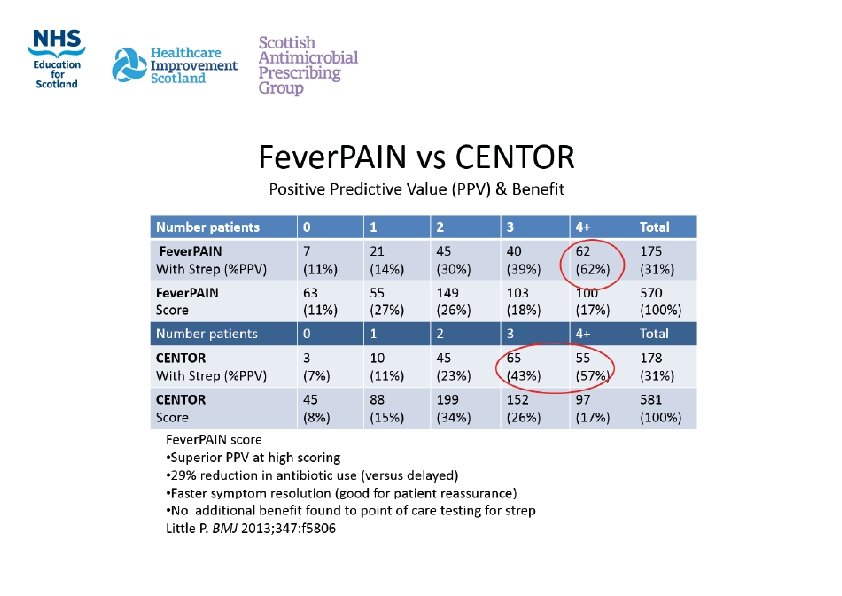
Sore Throat ‐ Assessing Risk Fever. PAIN https: //ctu 1. phc. ox. ac. uk/feverpain/index. php (online calculator) Fever. PAIN Score Fever in past 24 hours 0 or 1 Purulent tonsils 0 or 1 Attend Rapidly (within 3 days) 0 or 1 Inflammation of tonsils 0 or 1 No cough/ coryza 0 or 1 Score Risk Action Score 0‐‐‐ 1 13‐‐‐ 18%streptococci NO antibiotic Score 2‐‐‐ 3 34‐‐‐ 40%streptococci Delayed antibiotic (3 day delay) Score 4 or more 62‐‐‐ 65%streptococci immediate (if severe) or delayed antibiotic (2 day delay) Using score = 29% reduction in antibiotic use (versus delayed) and faster symptom resolution (good for patient reassurance) Little P. BMJ 2013; 347: f 5806

Using the score in practice • Identify a recent case where an antibiotic (e. g. phenoxymethylpenicillin) was issued for sore throat • Reassess using the Fever. PAIN score to see if the same treatment decision would have been reached • How do you think you could use scoring to support future consultations?

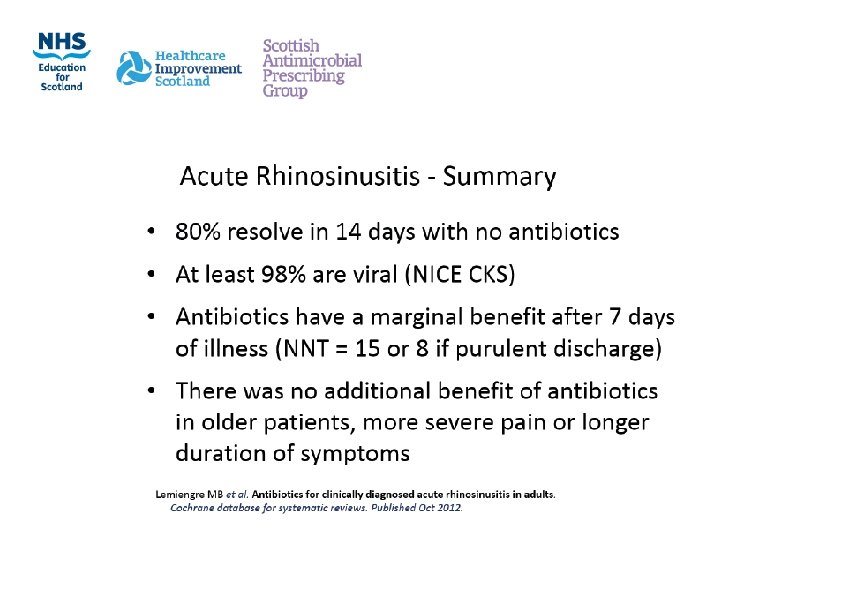
Acute Rhinosinusitis Q 1 How do you currently decide whether or not to give antibiotics? Q 2 How long do you think it takes for most cases to resolve? Q 3 What do you think are the benefits (if any) of giving antibiotics?

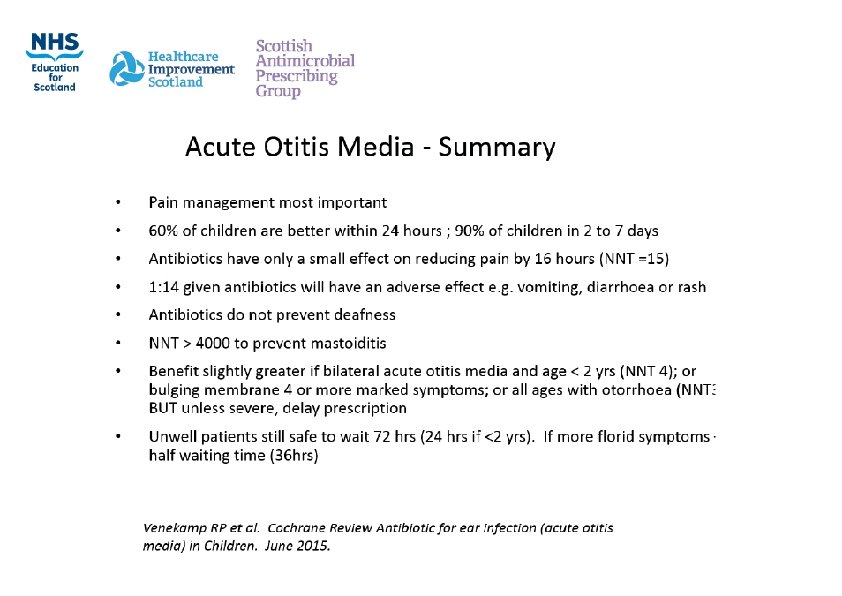
Acute Otitis Media When might antibiotics be required Q 1 How do you currently decide whether or not to give antibiotics? Q 2 How long do you think it takes for most cases to resolve? Q 3 What do you think are the benefits (if any) of giving antibiotics?

Lower Respiratory Tract Infection Acute Cough/Bronchitis

Acute Cough When might antibiotics be required Q 1 How do you currently decide whether or not to give antibiotics? Q 2 How long do you think it takes for most cases to resolve? Q 3 What do you think are the benefits (if any) of giving antibiotics?
 did not")
Acute Cough The Evidence Against Antibiotics • Prescription of an antibiotic (co‐amoxiclav) did not make a statistically significant difference to cough duration, with persistent cough in 40% at 15 days regardless of treatment 1 • The NNT to prevent 1 hospitalization for pneumonia was 12, 255 when an antibiotic given to patients with acute non‐specific respiratory infections 2 • Not much better than placebo. 3 Antibiotics reduce symptoms by less than 1 day in an illness lasting several weeks. 4 1. Llor C et al. Efficacy of anti‐inflammatory or antibiotic treatment in patients with non‐complicated acute bronchitis and discoloured sputum: randomized placebo controlled trial BMJ 2013; 347: F 5762 2. Meropol Sb et al. Risks and Benefits Associated With Antibiotic Use for Acute Respiratory Infections: A Cohort Study. Ann Fam Med March/April 2013 11: 165‐ 172 3. Wark P. Bronchitis (acute). Clinical Evidence. London. BMJ publishing Group 2008; 07: 1508‐ 1534 4. Fahey T et al. Antibiotics for acute bronchitis. Cochrane Library 2006, Issue 4.

Acute Cough When might antibiotics be required? If patient is older than 65 years with acute cough and two or more of the follow‐ ing criteria, or older than 80 years with acute cough and one or more of the fol‐ lowing criteria: • Hospitalisation in previous year • Type 1 or type 2 diabetes • History of congestive heart failure • Current use of oral glucocorticoids These factors make the patient more vulnerable to infection and therefore should be considered when making decisions as to whether an antibiotic is required National Institute for Health and Clinical Excellence. Respiratory tract infections – Prescribing of antibiotics for self‐limiting respiratory tract infec‐ tions in adults and children in primary care. 2008. (Clinical Guideline 69)

Acute Cough ‐ What about children? Reducing ‘Just in Case’ Prescribing • Evidence suggest GPs/nurses often prescribing for RTI in children ‘just in case’ over concerns about hospitalisation • 7 step algorithm developed by Bristol University aims to categorise risk of hospitalisation • Children scoring 1 or less = very low risk of hospitalisation at 30 days (1: 300) STARWAVe Short illness (≤ 3 days) Temperature (parent reported severe in previous 24 hours or ≥ 37. 8° on examination) Age (<2 years) Recession (intercostal or subcostal) Wheeze (on listening to chest with stethoscope) Asthma Vomiting (parent reported moderate / severe in previous 24 hours) Hay AD et al. Development and internal validation of a clinical rule to improve antibiotic use in children presenting to primary care with acute respiratory tract infection and cough: a prognostic cohort study. The Lancet Resp Med September 1, 2016

Prevention is better the cure Pneumococcal Vaccination Impact on Pneumonia rates Impact on Otitis Media infection rates Used by permission from Elsevier. , Article: Impact of pneumococcal conjugate vaccines on childhood otitis media in the United Kingdom Attribution: Contains public sector information licensed under the Open Government Licence v 3. 0. PHE data Vaccine 33 (2015) 5072– 5079

Summary Self Limiting RTIs Infection Self‐‐‐ limiting Without Antibiotic Considerations Otitis Media 4 days 90% 2‐‐‐ 7 days (60% resolve 24 hrs) • <2 yrs and bilateral • Bulging membrane, ≥ 4 marked Sx • Otorrhoea Sore Throat 1 week 90% resolve in 7 days CENTOR score Fever. PAIN Common Cold 1. 5 weeks Usually lasts about 1‐‐‐ 2 weeks N/A Sinusitis 2. 5 weeks 80% resolve in 14 days Purulent nasal discharge Cough/ Bronchitis 3 weeks Usually resolves 3 weeks (antibiotics only reduce symptoms by 1 day) 1. 2. 3. 4. 5. Co‐‐‐morbidities Always give self‐management advice/signpost to community pharmacy Educate on usual self‐limiting durations Do not prescribe an antibiotic if low risk If additional considerations consider delaying prescribing where appropriate Safety‐net – give patient information on signs of deterioration and what to do

Immediate Antibiotic – General Considerations • Systemically very unwell? • Symptoms and signs of serious illness/complications? • • Pneumonia Mastoiditis Peritonsillar abscess/cellulitis Intraorbital and intracranial complications • Pre‐existing co‐morbidity resulting in high risk of serious complications? • • Significant heart, lung, renal, liver or neuromuscular disease Immunosuppression Cystic fibrosis Young children born prematurely National Institute for Health and Clinical Excellence. Respiratory tract infections – Prescribing of antibiotics for self‐limiting respiratory tract infections in adults and children in primary care. 2008. (Clinical Guideline 69)

Reflection Assessing risk : benefit & making the prescribing decisions Pause for discussion • From the information you have heard what has had the most impact? • What do you think you can change in your practice? • How are you going to do this? • How will you know it has made a difference?
 Prescribing Patient Education/Self‐Management")
Part 2 ‐ Strategies to Reduce Unnecessary Antibiotic Prescribing Delayed (back‐up) Prescribing Patient Education/Self‐Management Near Patient Testing

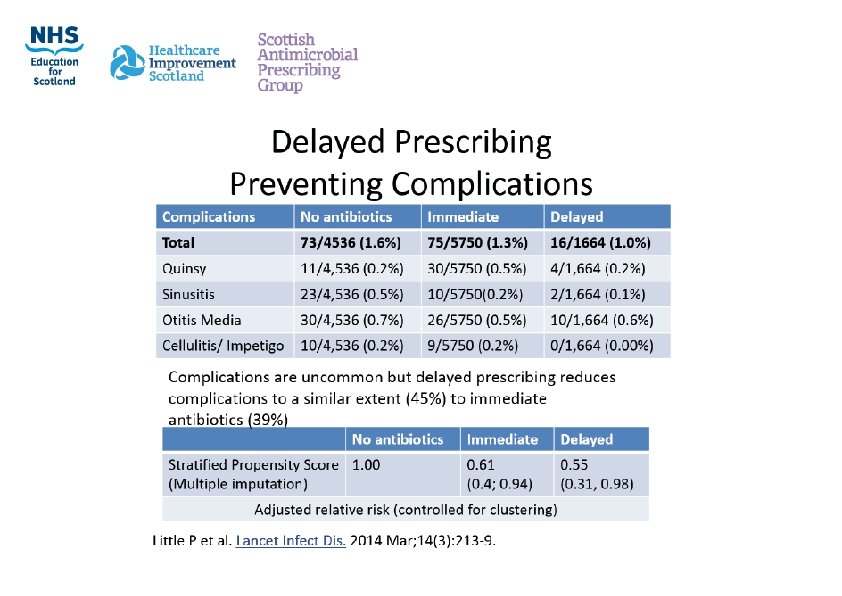
Benefits of Delayed Prescribing • Immediate versus delayed versus no prescription • No difference in most symptoms • Little difference in adverse effects • No difference in complications • Only small difference satisfaction (immediate 92%, delayed 87%, no prescription 83%) • Delayed prescribing resulted in 32% of patients using antibiotics compared to 93% of patients in the immediate prescription group • However, not prescribing antibiotics at all results in the least antibiotic prescribing (14% of patients used antibiotics) Spurling GKP et al. Delayed Antibiotics For Respiratory Infections. Cochrane Database of Systematic Reviews. April 2013 http: //www. cochrane. org/CD 004417/ARI_ delayed‐antibiotics‐for‐symptoms‐and‐complications‐of‐acute‐respiratory‐tract‐infections

Comparing Strategies • Little to choose between different delayed strategies if clear advice given • Recontact for prescription • Post‐dated prescription • Collection of the prescription • Given the prescription (patient led) • So doesn’t really matter how you do it, as long as used in the correct circumstances with correct patient information Little P et al. Delayed antibiotic prescribing strategies for respiratory tract infections in primary care: pragmatic, factorial, randomised controlled trial BMJ 2014; 348 http: //www. bmj. com/content/348/bmj. g 1606

Treating Your infection leaflet can be used in discussion with the patient to support education Contains public sector information licensed under the Open Government Licence v 3. 0 http: //patient. info/health/treating‐your‐infection‐public‐health‐england

Parent / Carer Educational Leaflet: ‘When Should I Worry’ Source: Cardiff University www. whenshouldiworry. com/resources/ When%20 should%20 I%20 worry‐Booklet_ Scotland. pdf

CRP near patient testing Public Health England/ NICE Guidance If considering antibiotics check CRP: • <20 mg/l = NO antibiotics • 20‐ 100 mg/l = DELAYED antibiotic • > 100 mg/l = IMMEDIATE antibiotic What about Scotland? Feasibility of use study undertaken 2015/16 10 GP practices involved www. scottishmedicines. org. uk/SAPG/C‐reactive_protein_CRP

Strategies In Practice • What is your experience of using delayed prescribing in practice? • How do you think you could better utilise this method? • What else could you do to reduce unnecessary antibiotic prescribing?

Summary – Key Points • Little evidence of benefit for antibiotics for acute RTI in the majority of patients • Use validated scores to avoid ‘just in case’ prescribing • Provide reassurance on expected duration • Encourage self‐management (utilisation of community pharmacy) • Utilise delayed strategies where appropriate • Remember unnecessary use causes harm!

Next Steps • What could we do better? • What do we need to do next, who will do it and by when? • How could we evaluate the impact of any changes? Practical Tips • Visit QI Hub for advice on action planning • Refer to ‘Sc. RAP Support Pack’ for examples of improvements and measures
- Slides: 41