Targeted Therapies Gynaecologische kankers ER HERs Angiogenese RANKL




 Dimerisatie Ligand EC-LBD Antibodies to EGFR")

 – – –")










 Herceptin or (HER 1+2) Lapatinib or Both Neoadjuvant BOTHHERCEPTIN % p. CR")
![Neoadjuvant HER block: % p. CR ~ ER-status [HER-2 (+)] Combin > Herceptin >](https://slidetodoc.com/presentation_image/8bb0db1f364d7a7794b75fa8ad6147a5/image-19.jpg "Neoadjuvant HER block: % p. CR ~ ER-status [HER-2 (+)] Combin > Herceptin >")
 Pertuzumab or (HER-2) Herceptin or Both Neoadjuvant % p. CR ~ ER-status [HER-2")
 Pertuzumab or (HER-2) Herceptin or Both Is CT needed if combined? Combinatie >Herceptin>Pertuzumab")
 Metastatic Setting 1 ste")


: Mechanism of Action Trastuzumab-specific MOA • Antibody-dependent cellular cytotoxicity (ADCC)")
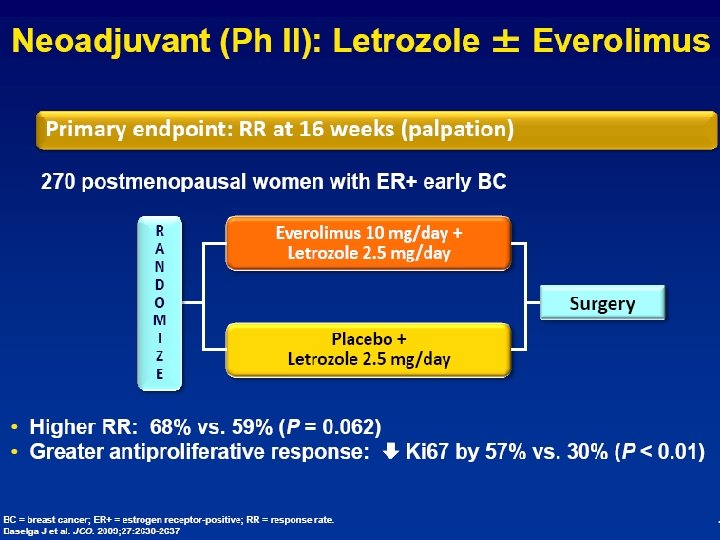
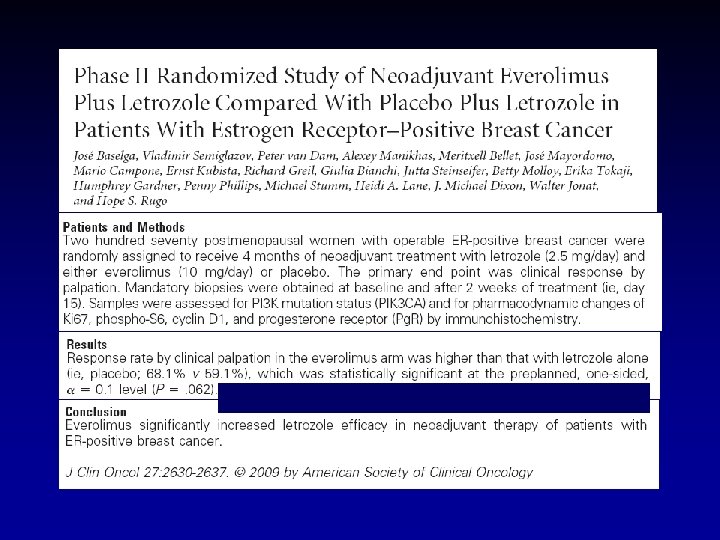
: Letrozole + Lapatinib > Letrozole Wat met HER-2 (-) borstkankers? (de novo)")




 Tumor vs Tumor Next-Gen")

 Median OS")
 Gem/carbo (GC) (N")
 – ITT Population 1. 0")


















 •")
 Letrozole + Lapatinib (N = 111)")


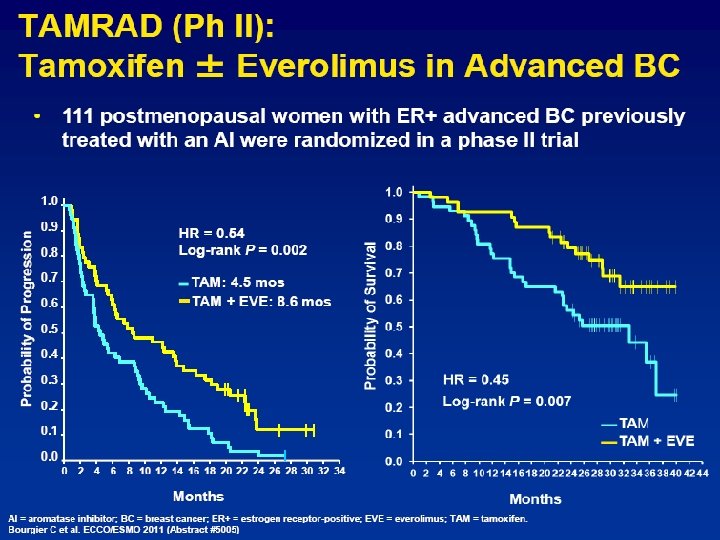
: median 26. 5 months")
- Slides: 69
“Targeted Therapies” Gynaecologische kankers ER HERs Angiogenese RANK-L PI 3 K, AKT, MTor FGF-R, ILGF-R (…) P. Neven GYN ONCOL UZ Leuven VVOG- Bredene - 2012
Disclosure Slide • None to be declared
‘Targeted therapies’ Gynecologische Tumoren ‘Tumors’ are “oncogen” addicted Despite the genomic & epigenomic complexities tumor regression can occur with inactivation of 1 or 2 oncogene(s) “Cancer Addiction to Oncogene” : The Achilles Heal of Cancer Weinstein IB Science 2002 Betere kennis mechanisme van kankerprogressie op cellulair en moleculair niveau moleculair-gebaseerde en geïndividualiseerde therapieën nut van therapie stijgt , onnodig nadeel daalt, en meer ‘cost-efficiënt’
EC-LBD “Targeted” therapies TMR IC-TKD “Treatment designed to specifically inhibit molecules* that provide advantageous growth signals to cancer cells. ” (G. Sledge, JCO, 2005) – Moleculen: *transmembranaire eiwitten essentiëel Voor intracellulaire signalen groei en overleving • Membraaneiwitten, signaaltransducers, immuuntherapie, … – Therapie: mab & nib (mono, combo, + anti-E, + chemo) • m. AB (blocks receptors (T), binds molecules (B), immune activator (Catumaxomab : Ep. CAM-CD 3)) • TKI (multiple)
Sleutelrol in tumorgroei en progressie Receptor (homo- hetero) Dimerisatie Ligand EC-LBD Antibodies to EGFR bv cetuximab, TMR PI 3 K IC-TKD p. Y PTEN p. Y RAS RAF EGFR-TK MEK STAT AKT MAPK m. TOR Gene transcription Cell-cycle progression Proliferation Chemotherapy / radiotherapy resistance Angiogenesis Invasion and metastasis Survival (anti-apoptosis) Tarceva, Iressa, Gleevec, Herceptin, Tyverb, Avastin, Meyerhardt & Mayer, N Engl J Med 2005 Venook, Oncologist 2005 Afinitor,
Targets met Targeted Therapies Farmacologische inhibitie ~response • • • Steroid receptors: ER+ borst, AR+ prostaat HER 2: borst, maag ALK: NSCLC CD 20: Lymphoma Targets ~ tumorgroei, … Response ~ Target? bcr/Abl: CML c-Kit: GIST Hedgehog: Basal cell, Medulloblastoma RET: Medullair Thyroid Carcinoma b-RAF, MEK: Melanoma • EGFR: CRC, Long, H&N (ras, EGFR mutatie) • VEGF-targeted therapy: alle kankers (niet RCC) • m. TOR: Borst, Nier, … but no target so far Effect therapie ~ Aantal Mutaties (TNBC tov ER-pos, Rokers)
Overzicht presentatie Targeted Therapies • Borst & Pelvien (kliniek & toekomst) – – – ER ; BMI HER-1; HER-2; HER-3 PTEN/AKT/m. TOR en MEK-MAPK pathway VEGF PARP …
NSABP B-14 q. ER = Predict for response to TAM Low levels ‘relative resistance’ RT-PCR but also for IHC?
Benefit of tam vs placebo ~ q. ER LBA/IHC
Aromatase Inhibitors Na MENOPAUZE Target = Fat Target = Total Body Aromatisation A Reduce Estrogen • Aromatase Inhibitors E Anastrozole Letrozole Aromasin Block ER • SERMs (Tamoxifen) ER
ATAC: Tam vs AI ~ BMI 100 mths FU J Clin Oncol 2010; 28: 3411 -5 . Target = Total Body Aromatisation ~ BMI Higher Weight More drug? ABCSG-12 : OS + Arimidex vs OS + Tamoxifen HR for relapse AI = Tam but x 3 on AI vs TAM if overweight JCO 2011; 29; 2653 -9.
SWOG FIRST LINE: 707 Postmenopausals ER+ and/or Pg. R+ MBC Fulvestrant + Anastrozole Fulvestrant i. m. 500 mg day 0, 250 mg day 14, 250 mg day 28, then 250 mg monthly + Anastrozole 1 mg p. o. Progression Survival Progression (cross over to F encouraged) Survival PFS: dates randomisation - first observed progression/death prior to progression
+ 8 months OS-benefit
Targeted Therapies Borstkanker Target: HER-2
Targeting HER-2 if amplified Breast Cancer l l l l 1987: 1992: 1999: 2002: 2005: 2010: 2011: 2012: Amplified HER-2 = Aggressive Tumor m. AB: Humanised anti-HER-2 Mab Survival benefit in Metastatic BC TKI: GW 572016 (HER-1 & HER-2 blocker) m. AB: DFS and OS benefit in Adjuvant EBC m. AB + TKI: p. CR-doubling of dual HER-2 block m. AB + chemo: TDM-1: HER-2 guided CT Trastuzumab - Pertuzumab #Moleculen en Bindingsplaats (1) Adjuvant (1 studie) Neo-Adjuvante (2 studies) Metastatisch (3 studies)
Target ‘HER’ Borstkanker LBD TKD Trastuzumab = Herceptin Lapatinib = Tyverb Pertuzumab
HER-2: Herceptin AC TH 87% D % F S 85% AC T 75% AC T H 67% AC TH N Events 1679 261 1672 134 HR=0. 48, 2 P=3 x 10 -12 Years From Randomization B 31/N 9831
(HER 2) Herceptin or (HER 1+2) Lapatinib or Both Neoadjuvant BOTHHERCEPTIN % p. CR ~ ER-status [HER-2 (+)] 455 HER-2 pos patients
Neoadjuvant HER block: % p. CR ~ ER-status [HER-2 (+)] Combin > Herceptin > Lapatinib: Diarrhea 25% & Low Compliance ALTTO-Trial: Stop Lap mono- arm p C R %
(HER-2+3) Pertuzumab or (HER-2) Herceptin or Both Neoadjuvant % p. CR ~ ER-status [HER-2 (+)] Ppp pppppp
(HER-2+3) Pertuzumab or (HER-2) Herceptin or Both Is CT needed if combined? Combinatie >Herceptin>Pertuzumab ER-Neg: No CT H+P = CT-P ▲ + chemo ▲ no chemo
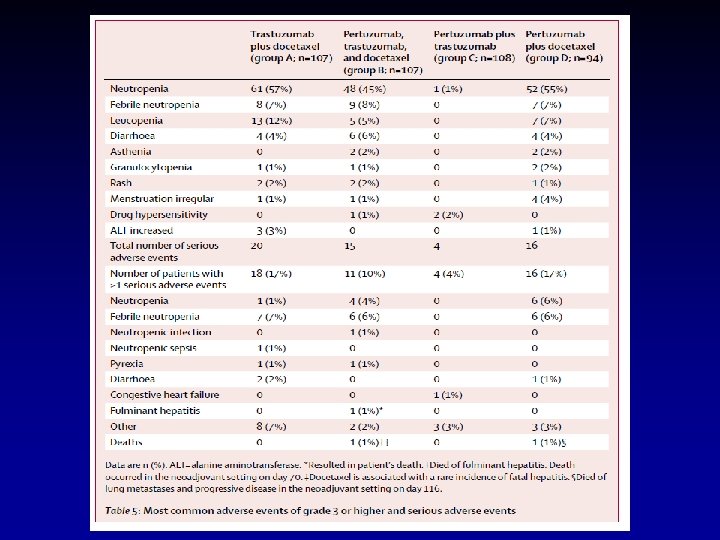
Neo-adjuv setting: “Combining Better” Herceptin + Pertuzumab >+ Lapatinib (diarrhea) Metastatic Setting 1 ste Lijn Logisch: Herceptin + Pertuzumab was toekomst. . en nu bewezen N Engl J Med 2012; 366;
Taxot + Herceptin + Pertuzumab Taxot + Herceptin N Engl J Med 2012; 366;
Metastatic Setting: Herval onder Herceptin Xeloda + Lapatinib vs HER-2 targeted CT. . nu ook bewezen Proportion progression-free 1. 0 Median No. of (months) events Cap + Lap 6. 4 304 T-DM 1 9. 6 265 Stratified HR=0. 650 (95% CI, 0. 55, 0. 77) P<0. 0001 0. 8 0. 6 0. 4 0. 2 0. 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 Time (months) No. at risk by independent review: Cap + Lap 496 404 310 176 129 73 53 35 25 14 9 8 5 1 0 0 T-DM 1 183 130 101 72 54 44 30 18 9 3 1 0 495 419 341 236 Unstratified HR=0. 66 (P<0. 0001). www. esmo 2012. org 24
Trastuzumab Emtansine (T-DM 1): Mechanism of Action Trastuzumab-specific MOA • Antibody-dependent cellular cytotoxicity (ADCC) • Inhibition of HER 2 signaling • Inhibition of HER 2 shedding HER 2 T-DM 1 Emtansine release P Inhibition of microtubule polymerization P P Lysosome Internalization Nucleus Adapted from Lo. Russo PM, et al. Clin Cancer Res 2011. www. esmo 2012. org 25
HER-2 (+): Letrozole + Lapatinib > Letrozole Wat met HER-2 (-) borstkankers? (de novo) Endocrine Resistance Behandel ook hier juiste “target”… l l l Target may change over time Outgrowth u ER-pos but ET resistant clone? Rebiopsy!!! u ER-negative (HER-2 +) clone? Downregulation of ER (promotor methylation) u Reactivate ER-expression (histone deacetylase) Enhanced peptide growth factor signalling u EGFR, HER-2, u Loss Pg. R, activation u PTEN/AKT/m. TOR or MAPK pathway u …
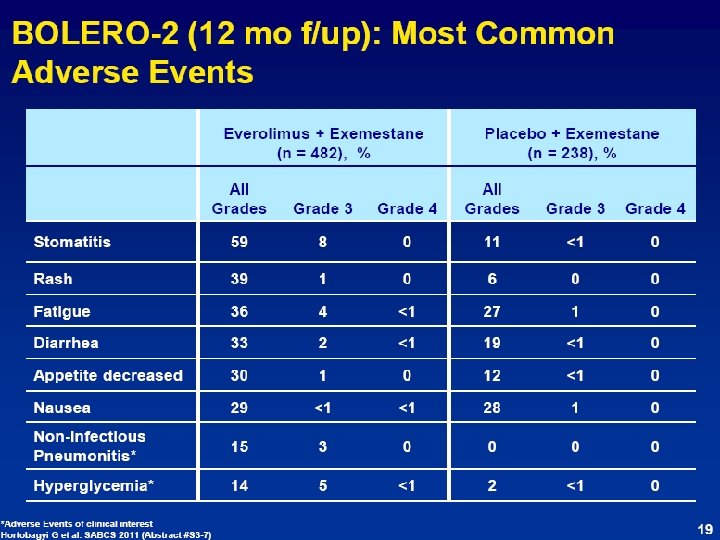
137 deaths 17. 2 % E + E 22. 7% E + P
Mucositis : Rash: Diarrhea: Non-Infect Pneumonitis: Hyperglycemia: 60% 40% 30% 15%
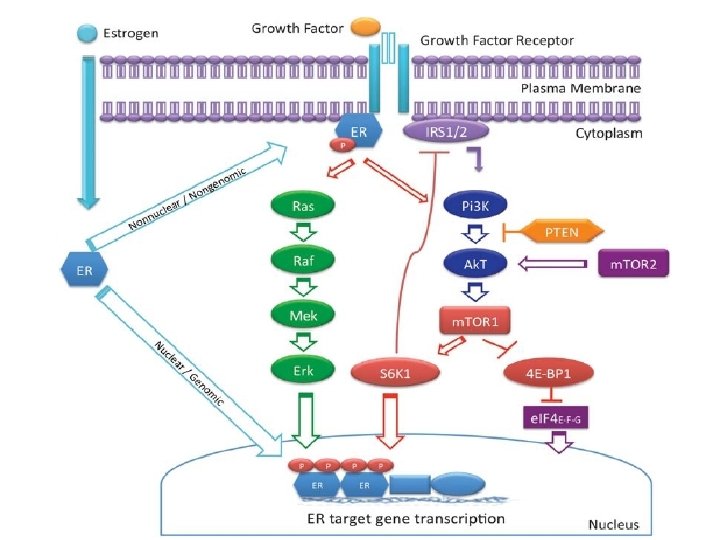
Inhibition of m. TOR signaling network can upregulate other pathways
TNBC: 3 Targeted Therapy Trials Treatment Target Rationale (prior data) Tumor vs Tumor Next-Gen Transcriptome Tumor vs Normal Next-Gen Fold Change/ P-value Clinical Trial Outcome Cetuximab & Gefitinib EGFR Overexpression of EGFR Not Overexpressed -1. 61 (p= 0. 09) NEGATIVE Imatinib c-KIT Overexpression of c-KIT Not Overexpressed BSI-201 PARP -6. 82 NEGATIVE (p= 1. 8 E-06) Overexpression Overexpressed 3. 97 of PARP/Synthetic (p = 2. 0 E-05) lethality in DNA repair Finding genes that are differentially expressed maybe a good start…. POSITIVE
If it’s broken PARP will fix it Targetting PARP in TNBC: don’t fix it TNBC BRCA-ness
ASCO-Plenary; 2009 PARP inhibitor: Overall Survival BSI-201 + Gem/Carbo (n = 57) Median OS = 9. 2 months Gem/Carbo (n = 59) Median OS = 5. 7 months P = 0. 0005 HR = 0. 348 (95% CI, 0. 189 -0. 649) O’Shaughnessy et al
Study Design: Multicenter, Randomized, Open-Label Phase III Trial (N = 519) Gem/carbo (GC) (N = 258) Gemcitabine 1, 000 mg/m 2 IV d 1, 8 carboplatin AUC 2 IV d 1, 8 Study Population: • Stage IV TNBC • ECOG PS 0 -1 • Stable CNS metastases allowed • 0 -2 prior chemotherapies for m. TNBC • Randomization stratified by prior chemotherapy in the metastatic setting: • 1 st-line (no prior therapy) • 2 nd/3 rd-line (1 -2 prior therapies) R 21 -day cycles Gem/carbo + iniparib (GCI) (N = 261) Gemcitabine 1, 000 mg/m 2 IV d 1, 8 carboplatin AUC 2 IV d 1, 8 iniparib 5. 6 mg/kg IV d 1, 4, 8, 11 21 -day cycles O’Shaughnessy J et al. Proc ASCO 2011; Abstract 1007.
Probability of Progression-Free Survival Efficacy Endpoints Progression-Free Survival (PFS) – ITT Population 1. 0 0. 9 PFS 0. 8 Median PFS GC (N = 258) GCI (N = 261) HR p-value 4. 1 mos 5. 1 mos 0. 79 0. 027 0. 6 0. 5 0. 4 0. 3 0. 2 0. 1 Prespecified alpha = 0. 01 0 0 2 4 6 8 10 12 14 16 Months Since Study Entry With permission from O’Shaughnessy J et al. Proc ASCO 2011; Abstract 1007.
TNBC Comprised of Diverse Molecular Subtypes Relative Frequency in Panel 0. 3 Preliminary* 0. 25 0. 2 0. 15 0. 1 0. 05 0 Basal Claudin-low ERBB 2 Luminal A Luminal B Normal-like * Validation ongoing Affymetrix gene expression profiling of FFPE samples Intrinsic subtypes assigned using Sorlie et al, PNAS, 2003 data set and claudin-low classifier (Prat et al, BCR, 2010) [courtesy of J Theilhaber and D Bergstrom, Sanofi] With permission from O’Shaughnessy J et al. Proc ASCO 2011; Abstract 1007.
The vascular endothelial GFR family
Targets in pelviene tumoren • ER, Pg. R, k. RAS, PTEN, P 53, HER-1 &2 – Anti-E – Mo. Ab: Encouraging results only… • VEGF (DFS) & EGFR & HER-2 & FGF-FGFR • Ep. CAM, CA 125, MUC 1, Folate Receptor, CTLA-4 • Ovarium>Cervix>Endometrium – Catumaxomab (ascites) NIB’s
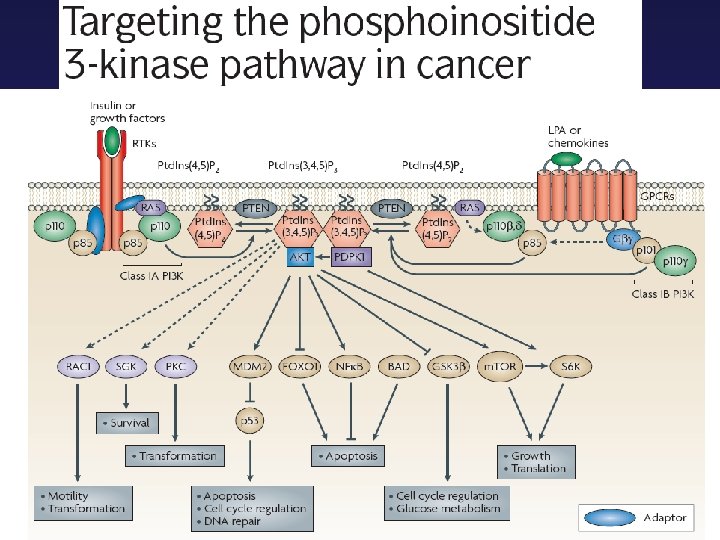
Incidence of genetic alterations in the PI 3 K pathway in cancer Small Molecules ‘nib’s’ Genetic alteration Cancer Type Incidence of tumors with alterations p 110α (PIK 3 CA) Breast Endometrial Cervical Breast Cervical Endometrial Ovarian 27% (468/1766) 24% (102/429) 69% (11/16) 8. 7% (8/92) 9% (2/22) 10% (3/29) 11. 9% (16/134) Amplifications Ovarian Breast 5% 5% Mutations Amplifications p 110β (PIK 3 CB) PIK 3 CA mutatie ~ response PAM (-) MAPK mutatie ~ resistentie?
Incidence of genetic alterations in the PI 3 K pathway in cancer Genetic alteration Cancer Type Incidence of tumors with alterations PDPK 1 Breast 20% Breast Ovarian Breast Endometrial Ovary Breast 3. 7% (31/845) 2% (1/50) 14. 1% (30/213) 3% (3/106) 4% (3/80) 24. 9% (99/398) 38% (604/1569) 9% (55/645) 6% (34/561) Amplifications and overexpression AKT 1 mutation (E 17 K) AKT 2 amplifications P 85α (PIK 3 R 1) Mutations PTEN Loss of heterozygosity Mutations
22 MDA Tx -patiënten 25/ 140 ‘uitbehandelde’ patiënten had PIK 3 CA mutatie en 23/25 PAM inhibitor 9/23 CB with PAM inhibitor (monotherapy of combinatie of + CT) 7/23 + BRAF, KRAS, NRAS (MAPK pathway)
Oktober 2012: UZ Leuven “Targeted Therapies”: On-Going GNC trials STUDIE PRODUCT WAT? TOEDIENING Abiraterone PO AZD 4547 selective irreversible inhibitor of cytochrome P 450 CYP 17 novel tyrosine kinase inhibitor with specific activity against the Fibroblast Growth Factor receptors (FGFR) BKM-GSK BKM 120 selective pan-inhibitor of Class I PI 3 K PO BKM-GSK 1120212 potent and highly selective inhibitor of MEK 1 and MEK 2 activation and kinase activity PO D-care Denosumab fully human monoclonal Ig. G 2 antibody to RANK ligand IV Genentech GDC-0941 selective pan-inhibitor of Class I PI 3 K PO Genentech GDC-0980 selective pan-inhibitor of Class I PI 3 K PO Incyte IDO inhibitor INCB 024360 potent, and selective inhibitor of the enzyme IDO 1 PO Medimmune MEDI-573 Monoclonal Antibody, IGF-I en IGF-II inhibitor IV Merrimack MM-121 anti-Er. B 3 human monoclonal antibody IV MK 8669 -064 dalotuzumab humanized monoclonal antibody targeting the IGF-1 receptor (IGF-1 R) IV Ombrabuline tubuline polymerization inhibitor, antitumor-vasculature agent IV p 38 MAPk Inhibitor of p 38 Mitogen. Activated Protein Kinase PO TKI 258 potent inhibitor of receptor tyrosine kinases PO Trinova studies AMG 386 anti-angiogenic drug IV XL 147 inhibitor of Class I PI 3 K family of lipid kinases PO BGOG-ov 7 AMG 386 (Trebananib) AMG 386 inhibit angiogenesis by sequestering Ang 1 and Ang 2 IV Ballet studie Afinitor m. TOR inhibitor PO SAKK trial AZD 6244 MEK 1/2 inhibitor PO Olaparib studies Olaparib PARP inhibitor PO Servier S 78454 HDAC inhibitor PO XL 184 inhibits RET, MET, VEGFR 2/KDR, and KIT PO Morab studies Farletuzumab a humanized Ig. G 1κ IV EORTC 55092 Pazopanib VEGFR inhibitor PO PO
Take Home Message “Targeted Therapies” ------------------------------Gynaecologische kankers ------------------------------Toekomst van Therapie bij Borst en Pelviene Tumoren = Combinaties van Targeted Agents … zonder chemo…
Randomised Phase II study of Anastrozole +/Gefitinib in patients with ER+ve Metastatic Breast Cancer Patients • Postmenopausal women • Age ≥ 18 years • Newly diagnosed ER and / or Pg. R positive metastatic breast cancer Anastrozole 1 mg / day + Gefitinib 250 mg / day Primary • Progression-free survival 1: 1 randomization • No prior hormonal therapy, or development of metastatic disease during / after adjuvant tamoxifen Response variables Anastrozole 1 mg / day + Placebo Secondary • Objective response rate • Clinical benefit rate • Overall survival • Safety and tolerability • Measurable or non- measurable disease (via RECIST) Cristofanelli et al, ASCO 2008, Abstract 1012
Randomised Phase II study of Anastrozole +/Gefitinib in patients with ER+ve Metastatic Breast Cancer Anastrozole + Placebo Gefitinib (n = 43) (n = 50) Events 22 32 Median PFS (months) 14. 5 8. 2 Probability 1. 0 of PFS 0. 8 HR (95% CI) = 0. 55 (0. 32, 0. 94) 0. 6 0. 4 0. 2 0. 0 0 3 6 9 12 15 18 21 24 27 50 43 35 40 23 28 13 22 9 13 6 10 5 6 3 3 1 2 1 30 Months At risk: Placebo Gefitinib Cristofanelli et al, ASCO 2008, Abstract 1012
Wat is “targeted therapie”? Target = Predictieve biomerker Goed omschreven molecule ~ tumorgroei/overlev -Molecule in normaal biologisch proces -Molecule in alle kankers -Molecule in sommige kankers (goed meetbaar) Molecule uitschakelen ~ Therapeutisch effect
Conclusions l Iniparib + GC no improved PFS or OS l Exploratory analyses of PFS and OS by prior therapy suggests: – Potential efficacy benefit among 2 nd/3 rd line patients. – Confirmatory study needed. l GCI safety profile confirmed; toxicity comparable to GC arm. l m. TNBC population is highly heterogeneous on intrinsic subtyping. l Biomarker analyses underway to evaluate patient populations that may benefit from iniparib. O’Shaughnessy J et al. Proc ASCO 2011; Abstract 1007.
e Som TN ted a HR l r u g o f pre ed RP u A y P l t e e r ra gula and us y l e r n n ir Ro EGF IT is dow NA repa K n D -ness i t c efe BRCA d e av BC h
Allred score 0 X Allred score 4 1 + 3 0 + 0 Allred score 7 5 + 2 ER IHC Allred score 8 5 + 3
Composite Markers Biomarkers response + prognose l l Combining Targets q. ER, q. Pg. R, HER-2, Prognosticators: Age, Grade, Size, p. N TEAM-Trial by Bartlett et al JCO 2011
Potential targets for HER-2 inhibition Antibody binding or TK inhibition Baselga & Swain, Nature Reviews Cancer 2009 Lapatinib
Graad 3 & 4 Toxiciteit & Early Stopping
Bij herval onder Herceptin stop Herceptin? Tyverb + Herceptin > Lapatinib in MBC patients relapsing on Herceptin
Femara versus Femara + Lapatinib Patient Population • ER+ / Pg. R+ (HR+) • Postmenopausal • HER 2+, HER 2 - or unknown • Stage IIIb / IIIc, IV • No prior treatment for MBC Stratification • Disease sites § Bone only / other sites • Interval since prior adjuvant anti-estrogen therapy § < 6 mo / > 6 mo or None R A N D O M I Z E Letrozole 2. 5 mg daily + Placebo Letrozole 2. 5 mg daily + Lapatinib 1500 mg daily n = 1286 pts (including n=219 HER 2+)
Progression-Free Survival: HER 2+ Population (N = 108) Letrozole + Lapatinib (N = 111) 89 (82%) 88 (79%) 3. 0 8. 2 Letrozole Progressed or died Median PFS, mo Hazard ratio (95% CI) p-value 0. 71 (0. 53, 0. 96) 0. 019 Johnston et al, J Clin Oncol 2009 27; 5538 -46
Side effects of PAM inhibitors Mucosa: aften Huid: dermatitis, ~acne G-I: diarrhea Metabool effect! Interactie Medicatie
Avastin first-line has proven to double PFS in combination with paclitaxel Avastin with paclitaxel doubles progression free survival 1 -3 Avastin doubles the chance of living without disease progression - A significant and clinically meaningful benefit for patients 1. Avastin Summary of Product Characteristics 23/07/2009 2. Miller K. N Engl J Med. 2007; 357: 2666 -76 3. Gray et al. J Clin Oncol. 2009; 27(30): 4966 -72
E 2100: Overall Survival 1. 0 Avastin + paclitaxel (n=368): median 26. 5 months Paclitaxel (n=354): median 24. 8 months 81. 2% HR=0. 869 (95% CI 0. 722– 1. 046) 0. 8 Log-rank p=0. 1374 OS estimate 73. 4% p=0. 01* 0. 6 Niet alle studies rooskleurig…. FDA NICE RIZIV 0. 4 0. 2 0. 0 0 6 12 18 24 30 Months 36 42 48 54 60 69