TAA Incidence TAA is diagnosed in approximately 15





















- Slides: 26
TAA Incidence: – TAA is diagnosed in approximately 15, 000 to 25, 000 people in the US annually ¹´² – Incidence is increasing due to : • Aging population (increased prevalence) • Increased access to sophisticated imaging Annual Incidence in Bulgaria: Ao dissection annual 13/100 000 (approx 1000 cases, 300 TAA/year) (prof. Nacheff Ph. D thesis) 1. Vascular Web. Available at: http: //www. vascularweb. org Accessed July 31, 2006 2. Bickerstaff LK, Pairolero PC, Hollier LH, et al. Thoracic aortic aneurysms: a population-based study. Surgery 1982; 92(6): 1103 - . 1108. . 3 Garrett HE. Getting started with thoracic endografting. Endovascular Today 2005; 1(11): Supplement: 13 -14.
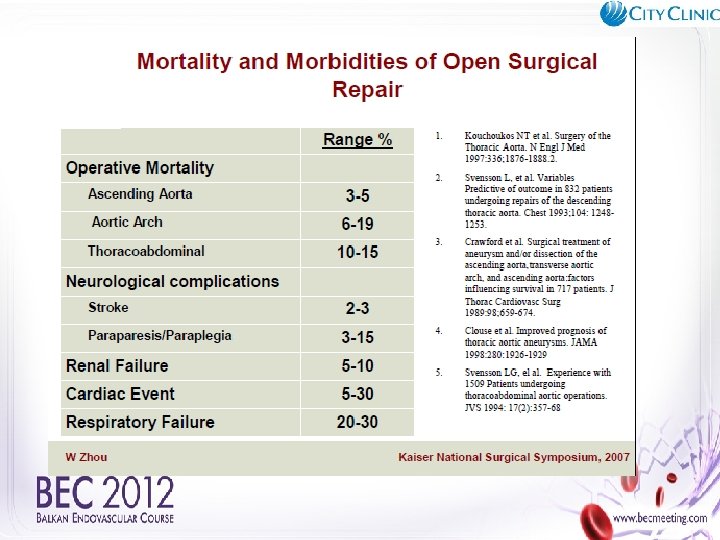
TAA Facts Mortality: 6, 000 deaths annually due to TAA ² • 5 -year Survival (untreated patients): 19 to 39% • Annual procedures volume: >18, 000 thoracic aortic repair procedures 2. Bickerstaff LK, Pairolero PC, Hollier LH, et al. Thoracic aortic aneurysms: a population-based study. Surgery 1982; 92(6): 1103 -1108 3. Garrett HE. Getting started with thoracic endografting. Endovascular Today 2005; 1(11): Supplement: 13 -14 . .
SYMPTOMS Although there are frequently no symptoms, TAA symptoms may include: Neck, chest or back pain (25%) Shortness of breath Difficulty swallowing Hoarse cough Congestion of head, neck, upper extremities (related to SVC compression)
Abdominal Aortic aneurysm Affects 4 -8% of elderly males 15, 000 deaths per year USA Screening and reduction of elderly male smokers reduces aneurysm related mortality by 46% USPHTF Ann Int Med Feb 2005
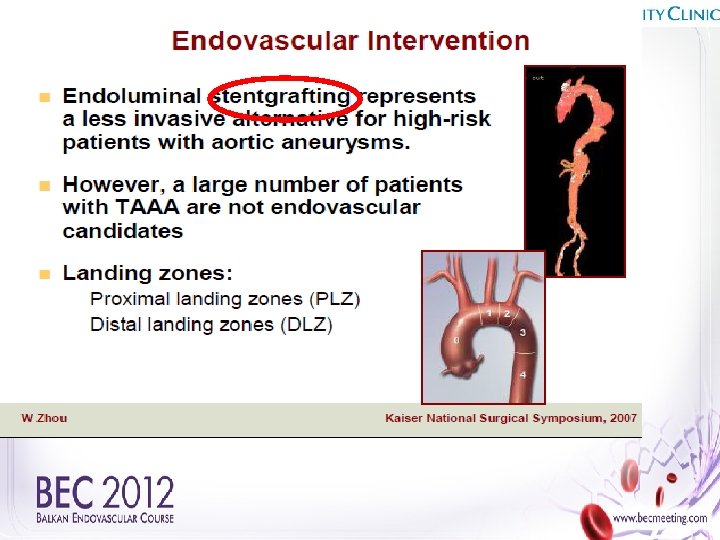
TREATMENT OPTIONS TAAs under 5. 0 cm: medical therapy, monitor annual growth by CT TAAs over 5. 0 cm in diameter: intervention/repair strongly considered Medical management (BP-lowering drugs) Open surgery Endovascular repair No proven lifestyle changes can decrease the size of TAAs.
Anatomic Criteria Proximal neck length >15 mm diameter <28 mm Tube graft: distal cuff length >10 mm diameter <28 mm Iliac artery diameter >7 mm and < 15 mm ◦ Minimal to moderate tortuosity No mural thrombus at attachment sites ◦ Minimal calcification No associated mesenteric occlusive disease
AAA: Landing Assessment zone >2 cm
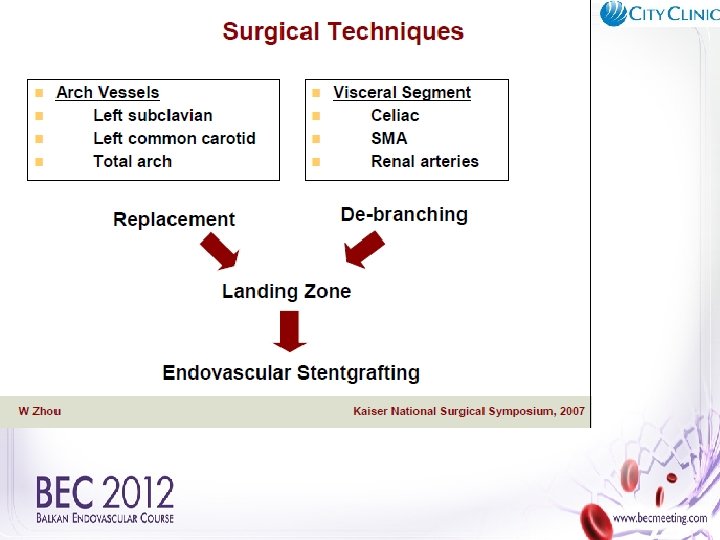
Maintaining Branch Vessel Patency Fenestrated Endografts Branched Endografts
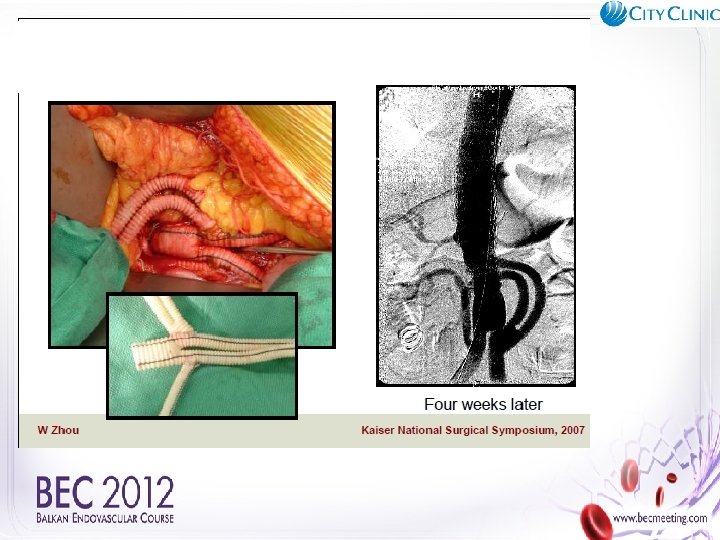
No landing zone Solution? Hybrid approach- surgery and endovascular or Cardiatis?
Cardiatis
Patient whit Aortic Dissection Stanford Type А. After surgical repair of Ao Asc. whit visceral and periphery ischemia implanted Cardiatis in thoracic Ao
Case presentation H. T. H. ; 75 year old male; with a history of an asymptomatic abdominal aortic aneurysm Comorbidities: Coronary Artery Disease 2 vessel disease. PCI + stent x 3 in the RCA. And PCI and stent in RIM. Periphery Artery Disease II st. Arterial Hypertension III gr. Operation due to Ca recti.
Aortography
CT- angio SMA
Celiac Trunk
CT- angio SMA RR
Case presentation 68 –male; V. E. F. with a history of an asymptomatic abdominal aortic aneurysm. Comorbidities- Coronary Artery Disease-1 vessel disease. PCI + stent in the LCx. Periphery Artery Disease II st. Chronic thrombosis of AFS dex. and a. tibialis post sin et a. perinea sin. Arterial Hypertension III gr. Gout/ Podagra/ Diverticulosis sygmae. Steatosis hepatis. Ptosis renis sinistra. In october 2012 CT was performed with evidence for abdominal aortic aneurysm.
Aortography TAAA
Aortography Abd. A
CT- angio
CT- angio IMA LR