SYSTEMIC PATHOLOGY 2014 2015 Prerequisite GENERAL PATHOLOGY Books

SYSTEMIC PATHOLOGY 2014 -2015 Prerequisite GENERAL PATHOLOGY

Books. . . Robbins Basic Pathology Editörler: Vinay Kumar, Abul K. Abbas, Nelson Fausto Türkçesi: Robbins Hastalığın Patolojik Temeli - ISBN 9789752771802 Robbins Temel Patoloji – ISBN: 9781416029731 Robins Review of Pathology (Türkçesi) - ISBN : 975 -8531 -21 -2 Rubin's Pathology: Clinicopathologic Foundations of Medicine Editör(ler) : Raphael Rubin , David S Strayer ISBN : 0781795168 Essential Pathology Editör: Emanuel Rubin ISBN : 0781723957 Temel Patoloji Editör: Prof. Dr. Gamze Mocan KUZEY ISBN : 975 -277 -104 -1

Pathology The most important field of Medical Science General Pathology Special Pathology or Systemic Pathology Clinical pathology Pathophysiology
 Pathophysiology & Pathology (students learn about basic")
The preclinical curriculum (3 rd Phase) Pathophysiology & Pathology (students learn about basic mechanisms of disease) in such fields Cardiovascular system Respiratory system Gastrointestinal system Endocrinology Hematology Genital & Urinary systems Diseases of Bones & Joints Central Nervous System

The course provides the educational experiences utilizing both lectures and interactive lab discussions. This course is the basis provided to the students for understanding various disease processes, as they proceed thereafter to the core clinical clerkships.

Systemic Pathology Requires the knowledge of General Pathology Requires correlation between normal Anatomy and Physiology and the process resulting in the manifestations of disease

The Systemic Pathology lectures were updated with Pathophysiology and “must” information will be given all year long Pathology lectures will guide you to enhance your understanding of disease.

never forget. . . There are 4 aspects of a disease process that form the core of pathology 1. 2. 3. 4. Etiology (the cause), Pathogenesis (the mechanism), Morphology (the alterations), Clinical significance (the consequences).
: Finding the primary cause(s) diagnosis treatment 2. Pathogenesis (the mechanism)")
1. Etiology (the cause): Finding the primary cause(s) diagnosis treatment 2. Pathogenesis (the mechanism) refers to the sequence of events in the response of the cells or tissues to the cause from the beginning (initial stimulus) to the end (the manifestations of disease)
: The morphologic changes refer to the structural and functional alterations")
3. Morphology (the alterations): The morphologic changes refer to the structural and functional alterations in cells and tissues: either characteristic of the disease or diagnostic of the etiologic process
: The nature of the morphologic changes and their distribution")
4. Clinical significance (the consequences): The nature of the morphologic changes and their distribution in different organs determine Signs and Symptoms Course & Prognosis of the disease.

The Pathology of Infectious Diseases Introduction Tissue Responses to Infections

Infectious agents Focus on PATHOGENESIS Know basic steps in the pathogenesis of: Viruses Rickettsiae Chlamydiae Mycoplasma Bacteria (incl. spirochetes&mycobacteria) Fungi Protozoa Helminths

Definitions Infection The ability of an organism to invade and establish itself in a host. Note: All infections DO NOT represent DISEASES !!!

Infectious Disease Agent: Organisms found in the environment that are capable of replication (either independently or with the host) capable of provoking an adverse response in the host

Infectivity and Virulence refers to the complex of properties that allows an organism to achieve infection and cause disease of different degrees of severity. The organism must (1) gain access to the body, (2) avoid multiple host defenses, (3) accommodate to growth in the human milieu, (4) parasitize human resources. Virulence reflects both the structures inherent to the offending microbe and the interplay of those factors with host defense mechanisms.
 Reservoirs (cave) Vector (sandfly) Susceptibility")
Epidemiology of Infectious Disease Example: Leismaniasis cutis (oriental sore) Reservoirs (cave) Vector (sandfly) Susceptibility of the host (common) Method(s) of Control (sanitation) Microbial Virulence Factors (antigens) Host Defense Mechanisms (cellular) Chemotherapy (amphotericin B paromomycin, miltefosine)

HOST BARRIERS TO INFECTION I. Local Barriers II. Humoral Immunity A. Antibody B. Complement III. Cell-mediated Immunity A. T-helper B. T-suppressor C. Cytotoxic lymphocyte IV. Phagocyte A. Neutrophil B. Monocyte, macrophage

The destruction of Local Barriers Skin Normal flora Staphylococcus epidermidis Candida albicans Dry keratinized epidermis Acidic p. H RISK OCCURS WHEN Cuts Lacerations Bites Indwelling lines Invasive procedures

Urogenital Tract Urine is normally sterile primarily due to constant flow Peristaltic motion and valves are designed to maintain unidirectional flow UT Infection rate Female : Male = 10 : 1 Acidic Ph of vagina RISK OCCURS WHEN Loss of the Acidic p. H of Vagina Polygamy Candida abicans HPV Sex. Transmtd Dis Urinary Tract Obstructions Exposure to pathogens which adhere to urothelium Some strains of E. coli Proteus Pseudomonas Gonococcus Staphyloccous saprophyticus

Respiratory tract Constant exposure to thousands of potential pathogens Unique defense structure: Mucociliary escalator Particles >5 micron : cleared by mucociliary escalator Particles <5 micron: cleared by macrophages & PMNs RISK OCCURS WHEN Mucociliary system is damaged (smoking, COPD, pathogens) There is an attack of infectious agents (capable to adhere to the respiratory epithelium) Immunocompromised Patient

Gastrointestinal tract Constant contact with organisms via food & water Defense systems: Mucus Gastric acid Pancreatic Fluids Bile salts Ig. A RISK OCCURS WHEN: Exposure to virulent organism Decrease in gastric acid production Antibiotic therapy Abnormal GI motility

Barriers. . Skin Tears Normal bacterial flora Gastric acid Bile Salivary and pancreatic secretions Filtration system of nasopharynx Mucociliary blanket Bronchial, cervical, urethral, and prostatic secretions Neutrophils Monocytes Complement Stationary mononuclear phagocyte system Immunoglobulins Cell-mediated immunity

PATHOGENESIS HOW CAN INFECTIOUS AGENTS CAUSE DAMAGE? Direct damage Release of Exotoxins, Endotoxins and/or irritant enzymes/proteins Induction of host immune response

VIRAL INFECTIONS IMMUNE RESPONSE TO VIRAL INFECTIONS Natural Killer Cell Cytokine Release boosts the immune response directly inhibits viral replication Cytotoxic T Cell B cells - Neutralizing antibodies
 Ability to")
BACTERIAL INFECTIONS Virulence Endotoxins Exotoxins Potent enzymes (Flesh-eating bacteria, Group A Strep) Ability to survive and proliferate intracellularly (Tb) Spread in the Host Macrophages may aid in spread (Tb) Bloodstream and Lymphatics (almost all bacteria) Motility and Chemotaxis (Vibrio cholerae) Cell and Tissue Damage
 Lipotechoic acids Fimbriae &")
Virulence Factors Adhesins Capsular material Proteins (Protein F, Protein M) Lipotechoic acids Fimbriae & Pili Endotoxins Gram negative LPS cell wall components (Lipid A and Core Sugars) Exotoxins Can be produced by either Gram (+) or Gram (-) organisms

Special consideration for Mycobacteria Distinctive waxy cell coat requiring Acid Fast Stains Virulence is related to cell wall ”cord factor” which inhibits phagosome-lysosome fusion Lipid cell wall components help initiate delayed cellmediated hypersensitivity response in the host GRANULOMAS Special culture methods used; may take up to 6 weeks

FUNGAL INFECTIONS Only a few commonly infect man increasingly important with the rise in immunocompromised patients Route of Infection - Almost always the LUNGS +/- clinical pulmonary symptoms & signs pulmonary disease may be subclinical, mild, or severe Fungi may produce toxins (mycotoxins) Immune Response: Essential in clearing infections CLASSICALLY GRANULOMATOUS
 Eliciting an Immune Response")
PARASITIC INFECTIONS MECHANISMS of INJURY Mechanical Injury (ie. hookworm larvae) Eliciting an Immune Response (ie. hookworm larvae in the lungs cause eosinophilic pneumonia) Nutritional depletion Adult hookworms Ascaris Giardia lamblia Digestion of host tissues (ie. Entabmoeba histolytica) Toxins and toxic metabolites (ie. Plasmodium in Malaria) Combinations of the above are common
 Necrotizing Inflammation Granulomatous Inflammation")
HOST RESPONSE TO INFECTIOUS AGENTS Acute Inflammatory Response (exudative; suppurative) Necrotizing Inflammation Granulomatous Inflammation Mononuclear Inflammatory Response (Chronic Inflammation & Scarring) Cytopathic-Cytoproliferative Inflammation

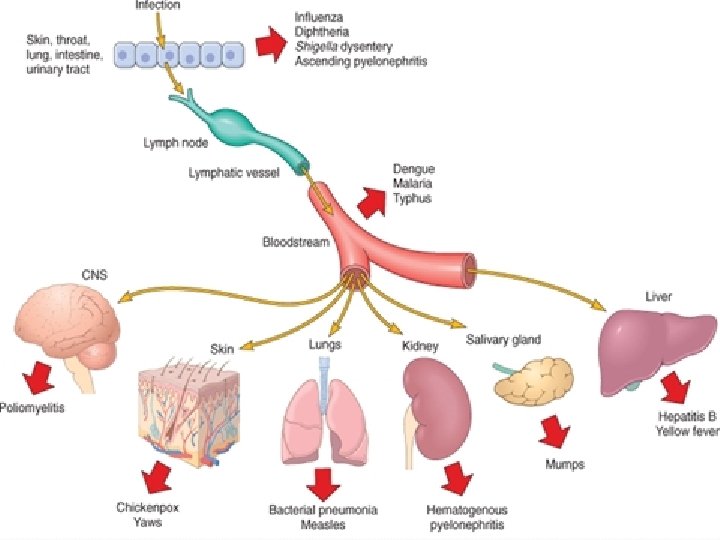
Manifestations of infection diseases

Blood manifestations: - Leukocytosis: an increase in the number of leukocytes in the blood (mostly bacterial) - Neutropenia: insufficient circulating neutrophils (salmonelosis, brucellosis, pertussis, and some viral and rickettsial infections) - Anemia: insufficient circulating erythrocytes (clostridium, malaria, mycoplasma, chronic infections) - DIC: disseminated intravascular coagulation (bacteria, virus)

Organisms in blood: Bacteremia: Few bacteria in the bloodstream, whether or not they are causing disease Viremia Septicemia: Bacteria traveling around the body via the blood Infected blood causes severe disease Pyemia: Pyemia is a seldom-used term which means "pyogenic organisms" (staphylococcus, streptococcus, gram-negative rods) infecting the blood
 Central nervous system manifestations")
Renal manifestations Immune Complex Glomerulonephritis Hepatic manifestations Icter (Jaundice) Central nervous system manifestations Cerebral malfunctions (confusion, convulsions, coma) Cardiovascular manifestations Septic shock, endocarditis SYSTEMIC manifestations= multiorgan dysfunction

Thank you….
- Slides: 37