Systemic Lupus Erythematosus and Neuropsychiatric Disease Barbara E

Systemic Lupus Erythematosus and Neuropsychiatric Disease Barbara E. Ostrov, M. D. Professor of Pediatrics and Medicine Pediatric Rheumatology and Rheumatology Penn State Hershey

Case 1 ¡ 40 yo African-American F diagnosed with SLE x 6 mos - 2006 l SLE features leading to dx: ¡ ¡ polyarthritis, +ANA, +anti-DNA, rash, fatigue, cytopenia 2007 presented with fever, muscle pain, malaise, overwhelming depressive sx for 2 wks l l WBC 3000, Hb 11. 0; ESR 90 urinalysis 2+protein, 1+ RBC seems very withdrawn dialysis required; depressive sx progress

Case 2 ¡ 15 yo Hispanic F with no past hx presents to ED in 2006 for 2 nd time in the past month l 6 weeks of recurrent fevers, HA, fatigue l l l on exam, temp 39. 0; BP 145/85; HR 100 ¡ obviously in pain with photophobia from HA ¡ no rash ¡ tender joints on exam ¡ no edema Labs: ¡ WBC 2500; Hemoglobin 7. 5 platelets 140, 000 ¡ ESR 80 mm/h vision deteriorates; HA continues

Case 3 ¡ 36 yo white F with SLE x 20 yrs l historical SLE features: chorea, arthritis, WBC 2. 0 -3. 0, low platelets; adrenal insufficiency, + ACL Ab age 31, after 2 miscarriages, delivered 30 wk baby peri-partum: SLE flare with rash, arthritis, low platelets 6 -9 months post-partum: notes gradual memory difficulties ¡ l l l ¡ short term memory, work with #s, sequencing tasks

Case 4 ¡ 30 yo Asian F with SLE x 15 yrs l historical SLE features: rash, arthritis, cytopenias: WBC 2. 5 -4. 5, Hb 10 -11, platelets 150, 000 ¡ AVN both hips, + DNA Ab, ESR 30 -50 ¡ ¡ presents in 2001 with fever, severe malaise, muscle and joint pain, HA, tingling feet l ¡ WBC 2, 000, Hb 10. 0, ESR 80, creatinine 0. 7 rapidly progressive weakness of legs over 2 days in ICU

Objectives review the epidemiology of SLE ¡ discuss the criteria of SLE ¡ discuss organ system involvement and tailored treatment of SLE ¡ focus on the various neurologic features of SLE ¡ discuss morbidity/mortality of SLE ¡

Incidence 5% of pts in US pediatric rheum practices ¡ 10% of US adult rheum practices ¡ Incidence: ¡ l l 2 -8/100, 000/yr in adults 0. 3 -0. 9/100, 000/yr in children 5, 000 -10, 000 prevalence in US children ¡ ~ 100, 000 -200, 000 adults ¡ l varies with ethnic groups up to 3 fold > in other ethnic groups: ¡ African American, Hispanic, Asian ¡

Demographics ¡ ¡ Adult onset 80% cases Childhood onset SLE 20% of all cases l ¡ F: M ratio = 9: 1 in teens/adults l ¡ 5: 1 in children Twin studies: l l ¡ < 5% with onset prior to age 10 24% concordance in monozygotic twins 2% in dizygotic twins HLA-DR 2 and DR 3 l increases RR 2 -3 x in Caucasians

Etiology/ Pathogenesis ¡ ¡ Etiologic factors include: Immune dysregulation: l l l hypergammaglobulinemia complement deficiency (C 2, C 4, C 5) autoantibody production cytokine activitation inability to clear immune complexes ¡ organ and tissue deposition T cell lymphocytopenia ¡ defect in switch from T helper 0 to T helper 2 cells l thus promoting B cell activation.

Etiology/ Pathogenesis ¡ Hormones l relative androgens estrogens Exacerbated by pregnancy in some ¡ Environmental factors: ¡ l l l UV light Viral infection (? EBV, ? CMV) Drugs ¡ Hydralazine, isoniazid, minocycline, anticonvulsants

1997 ACR Criteria ¡ ¡ ¡ ¡ ¡ Malar rash ¡ + ANA Discoid rash ¡ + Immunoserology Photosensitivity l ds. DNA Antibodies l Anti-Smith Antibodies Oral/nasal ulcers l Antiphospholipid Ab’s Serositis Nephritis Non-erosive arthritis Cytopenias Neuropsychiatric Aim: more homogeneous population in research 4/11 criteria: 88% Sensitivity/Specificity

Cutaneous ¡ Malar l l l ¡ Discoid l l l ¡ “butterfly” rash ½ to 1/3 at onset symmetric SPARES nasolabial fold no scarring face, helix, scalp Often asymmetric demarcated papular lesions Scarring, alopecia More severe in dark skinned people Photosensitivity

Treatment for Skin ¡ Sun block l l ¡ 70% are photosensitive at least 45 SPF antimalarial agents l l l NON immune suppressing hydroxychloroquine >>> quinacrine ~70% response rate ¡ ¡ monitor annual eye exams occasionally: l dapsone, steroids, azathioprine, rituximab

Oral and Nasal Ulcerations ¡ ¡ Classically, PAINLESS ulcerations occur on the HARD palate l ¡ buccal = non-specific In the nose they occur on the septum l asx septal perforation can occur
 l l l ¡")
Serositis/ Cardio-pulmonary ¡ Pericarditis is most common cardiac complication (30%) l l l ¡ Pleural effusions (~30%) in children l 2º pleural inflammation or pneumonitis or to nephrotic syndrome Usually bilateral and small w/o respiratory compromise May be subclinical Sx: precordial chest pain, l by laying down, by l sitting up and forward Constriction, tamponade rare ¡ Pulmonary hemorrhage - rare l life threatening complication

Serositis Treatment ¡ Rule out infection l ¡ ¡ ¡ serosal fluid analysis for infection, ANA ¡ + ANA MAY suggest lupus etiology Rule out other causes of chest pain or effusions: MI, PE, coaguloapthy, GI cause NSAID can help pain steroids low to moderate dose l l l 1 -2 mg/k/d max ~ 40 -60 mg a day usually do not need very hi doses

Nephritis ¡ Clinically active in 50 -75% of pts l ¡ Presentation (in order of frequency): l l l ¡ Microscopic hematuria Proteinuria Lowered GFR Worst prognosis: l l l ¡ Likely to some degree in ALL with SLE ¡ Bx, EM shows some change on all poorly controlled HTN creatinine Class IV, nephrotic syndrome males, AA, ? Hispanic races Renal disease usually w/in 2 yrs of onset

WHO Classification ¡ ¡ ¡ ¡ Class Class I IIA IIB III IV V VI DPGN ¡ ¡ ¡ ¡ Normal Minimal change Mesangial proliferation Focal/segmental proliferation Diffuse proliferative Membranous Glomerulosclerosis membranous

Treatment Renal Disease ¡ Crucial to control BP l ¡ mild class II to III l ¡ azathioprine, mycophenolate and possibly cyclophosphamide class IV l l l ¡ poor control predicts ESRD pulse cyclophosphamide mycophenolate 2 -3 years maintenance Future roles for anti-B cell therapies (rituximab), other biologics

Arthritis ¡ ¡ Non-erosive, Painful or painless Jacoud arthropathy l ¡ reversible subluxation due to tenosynovitis Symmetric small and large joint involvement

Treatment of Arthritis ¡ Most pts respond to common regimen: l l l NSAIDs anti-malarials low dose prednisone < 10 mg a day ¡ beneficial in > 75% of pts ¡ ¡ uncommon need for higher doses For those who fail: l l l methotrexate, leflunomide consider anti-TNF agents (? ? drug induced LE) consider rituximab

Cytopenias ¡ Rule out other causes: l ¡ All cell lines can be affected l l l ¡ medication induced, sepsis, TTP Hemolytic Anemia - Coomb’s positive Thrombocytopenia < 100, 000 Leukopenia ¡ Lymphopenia (<1500 cells/mm 3) Treatment: l l steroids: 1 -2 mg/kg/d prednisone; ? pulse IVIG rituximab consider TTP, urgent plasmapheresis

Positive ANA ¡ IFA l l ¡ ¡ > 98% of pts with SLE NOT sufficient for diagnosis l l ¡ Usually peripheral or homogenous patterns have poor specificity for SLE NOT predictive of severity NO correlation with disease activity for most MORE common in healthy people l due to meds, viral infections, normal variation ¡ 5% of general peds population ¡ 20% adult population

Positive ANA ¡ HMC Lab uses Laser Bead technology l in Power Chart, ANA “positive” means: ¡ > 1 of these found: l ¡ anti-DS-DNA, anti-Smith, anti-RNP, anti-SCL-70, anti. JO-1, anti-histone, centromere, anti-SS-A, anti-SS-B results 100 -200 often false + for some dx, expect + ANA but - other serology Athena unreliable ¡ order “SEND OUT” for ANA by IFA or repeat any serology by ordering “SEND OUT” ¡ ¡ NOTE: ANA “screen” reported with no titer clue that a lab is using this method

Immunoserologies ¡ Anti-Double-Stranded DNA Antibodies l l ¡ Present in ~ 60% patients with active SLE Very specific Fluctuates with disease activity may be predictive of nephritis Anti-Smith Antibodies l l Present in 25 -30% of SLE Very specific does not fluctuate with disease activity Higher frequency in black females

Antiphospholipid Antibodies ¡ Antibodies which bind to negatively charged phospholipids l l l Anticardiolipin Ig. G, Ig. M Anti -2 Glycoprotein-1 Ig. G, Ig. M Lupus anticoagulant, Prolonged PTT ¡ l DRVVT, Platelet neutralization procedure Historical interest: ¡ False positive RPR test l uses a cardiolipin-cholesterol-phosphatidylcholine antigen which can give false results

Antiphospholipid Syndrome ¡ Presentations: l l l Recurrent fetal loss; 2 nd, 3 rd >1 st trimester Arterial thrombosis Venous thrombosis Thrombocytopenia Livedo reticularis Catastrophic APS ¡ acute multifocal manifestations
 neonatal LE, Anti-SS-B (La) photosensitivity, rash Neuropsychiatric")
Other antibodies ¡ ¡ ¡ Anti-SS-A (Ro) neonatal LE, Anti-SS-B (La) photosensitivity, rash Neuropsychiatric Lupus related ab: l features may be due to combos of these ab ¡ anti-NR 2 ab to glutamate receptor neuronal injury ¡ anti-ribosomal- P l ¡ anti-neuronal l ¡ psychosis, depression non-specific for SLE or certain NP features anti-Neuro Myelitis Optica Ab l l Devic’s disease = optic neuropathy, myelitis anti-aquaporin-4 ab: astrocyte foot processes, water channels, immune complex formation l NP Lupus Rheum Dise Clin N Am 31: 273

Neuropsychiatric Lupus ¡ Part of Criteria: l ¡ Seizures, psychosis More varied manifestations: l Central nervous system Ø Ø Ø l Psychiatric: Psychosis - paranoia, hallucinations Seizures - general or focal Aseptic meningitis Thrombotic: CVA/TIA Other: Chorea, headache, Pseudotumor cerebri, myelopathy, cognitive Peripheral nervous system Ø Ø Ø GBS autonomic neuropathy mononeuritis multiplex, polyneuropathy l ACR Criteria A & R 1999 42: 599

NP Manifestations ¡ Most common l l l l cognitive 50 -80% HA 25 -70% mood 15 -60% cerebrovascular 5 -20% seizures 5 -50% neuropathy 10 -30% psychosis 5 -10% ¡ Least common l < 2 -3% ¡ movement dx ¡ demyelinating ¡ myelitis ¡ MG ¡ GBS ¡ autonomic ¡ aseptic meningitis

Epidemiology ¡ ACR case definitions l up to 90% of all SLE pts have some sx ¡ l many of these sx are also in 50% non. SLE persons: low specificity if case defs exclude: HA, anxiety, mild depression, mild cognitive, neuropathic sx w/ normal studies ¡ then define NP sx in 46% of SLE pts l l 7% non-SLE persons specificity 93% ¡ ACR Criteria A & R 1999 42: 599

Pathophysiology - Multifactorial ¡ autoantibodies ¡ ¡ ¡ get thru weakened BBB, intrathecal production anti-neuronal, anti-ribosomal P, APS, NMO vascular ¡ microangiopathy l l ¡ small vessel vasculitis - large vessel RARE non-inflammatory vasculopathy ¡ thrombosis, microinfarcts, ASVD ¡ often due to secondary causes not 1º due to SLE inflammatory mediators; cytokines ¡ measured in CSF, serum - not clinically used now l l ICAM-1, IL-6, IL-8, IL-10, TGF- , interferon- increased nitric oxide

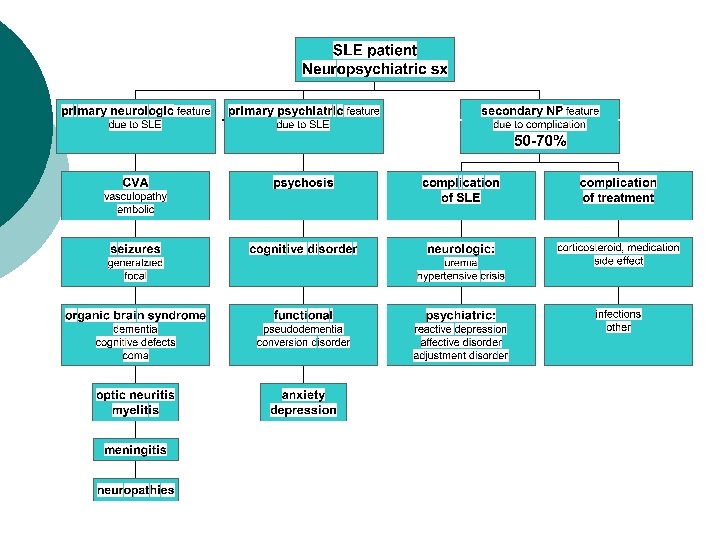
Pathogenesis Complications of SLE or Rx Non-SLE NP complications

Specific NP Features May occur any time in course ¡ often an early feature ¡ l l l prior to clearcut SLE with multiorgan flare when SLE seems to be quiescent

Cognitive ¡ Most with mild deficits on NP testing ¡ l l ¡ 20 -80% of pts attention, memory, visual-spatial processing, reasoning, speed, higher level functioning reflects overall brain health outcome l l impairment improves in most 15% continued impairment; 5% persistent or worsening over 5 yr f/u ¡ l ¡ 5 yr longitudinal Rheumatology 2002 41: 411 any NP event in course associated with some cognitive decline Serology: Anticardiolipin Ab: Ig. G and Ig. A

Psychiatric Manifestations ¡ Psychosis 10% l l ¡ depression, anxiety 25 -60% l l ¡ hallucinations - mostly auditory distinguish from drugs, depression, schizophrenia common in general non-SLE pop more often 2º to an non-SLE etiology Serology: l l anti-ribosomal P ¡ psychosis, depression 4 -10 X odds ratio antiphospholipid ab 1. 5 X odds ratio

Seizures ¡ Generalized and focal l l 5 -50% severe multisystem flare ¡ l ¡ 1º due to SLE or 2º renal, HTN, infection isolated events Serology: l Antiphospholipid ab with microthrombi

Meningitis In up to 10 -15% ¡ Must consider 2 causes ¡ l meds: NSAIDs ¡ l ¡ higher incidence of ibuprofen induced in SLE pts infection CSF: l l lymphocytes hi protein

Cerebrovascular Disease ¡ Rule out embolic source l ¡ Multifactorial l l ¡ Libman-Sacks 5 -20% stroke, TIA HTN, renal disease accelerated ASVD ¡ 5 -10 X odds ratio Prothrombotic state l APS, hyperhomocysteinemia

Posterior Reversible Encephalopathy Syndrome ¡ PRES - similar to SLE NP features ¡ ¡ l ¡ etiology: ¡ sudden BP , distention cerebral vessels; fluid extravasation ¡ HTN, CRF; meds: CTX, hi dose steroids, others Imaging is crucial: l l MRI- FLAIR- inversion recovery suppress CSF - edema 94% DWI - diffusion weighted imaging ¡ ¡ ¡ Acute mental status, HA, seizure, vision loss MRI - white matter bilateral parieto-occipital area signal; in cerebral ischemia Resolves in 1 -4 wks Rx: BP/seizure control, med changes when possible l PRES - CNS SLE Lupus 2007 16: 436

Headache ¡ True pathologic relationship with SLE controversial l prevalence 20 -70% ¡ l controlled studies ¡ ¡ but HA 40% in non-SLE pop no increase in HA compared to non-SLE HA common but more likely not directly due to SLE ¡ Lupus 2003 12: 947

Myelopathy, chorea ¡ Rare features l l ¡ 1 -3% of pts demyelination ¡ may look like from MS l ? Overlapping autoimmune dx ¡ transverse myelitis ¡ chorea Serology l l anticardiolipin ab: thrombotic, interaction with basal ganglia NMO ab 94% specificity

Peripheral Nervous System Neuromuscular ¡ Neuropathy up to 30% l l ¡ Neuromuscular: l l ¡ ¡ mononeuritis multiplex autonomic sensorimotor cranial myositis, vasculitic, myasthenia-like drug induced: steroid >>>antimalarial drug Bx: small fiber neuropathic, vascular Course: 2/3 stable over long term f/u

Diagnostic Testing ¡ ¡ ¡ ¡ Labs CSF analysis Retinal exam CT - bleed/stroke MRI l FLAIR l DWI PET scan SPECT scan NP testing

NP disease: Assessment ¡ Lab: l l ¡ CSF: ALWAYS RULE OUT INFECTION l ¡ assess disease activity: C 3, C 4, anti-DNA specific serology: anti-P ab, APS, NMO unclear if CSF ab or cytokines help SLE dx Imaging structure and function: l l l CT - acute bleed MRI, FLAIR, Functional MRA less useful ¡ PET - changes in glucose metabolism l SPECT - cerebral blood flow Neuropsychologic testing l ¡ small vessel vasculopathy does not show up

Treatment for NP Lupus ¡ First step: rule out SLE vs other cause l l ¡ Manage co-existing issues l ¡ active inflammation ¡ vs complication of disease or Rx NP SLE is dx of exclusion HTN, infection, metabolic abnormalities Manage symptoms l l l antidepressant, anxiolytics anti-psychotic psychotherapy, cognitive therapy migraine Rx ? anti-coagulant ? ASA immune suppression

Treatment ¡ ¡ No placebo-controlled studies Immunosuppression l l pulse and/or hi dose steroids ¡ 30 mg/kg up to 1000 mg methylprednisolone ¡ 2 mg/kg/day cyclophosphamide ¡ daily oral 2 -4 mg/kg/day ¡ pulse for 3 -6 months l l l 500 -1000 mg/m 2 other: azathioprine, combined therapies new therapies: ¡ biologic therapy - anti-CD 20

Morbidity ¡ ¡ Renal Musculoskeletal Ocular Endocrine ¡ Immunologic Heart ¡ Neurologic ¡ HTN, dialysis, transplant AVN, osteoporosis Cataracts, glaucoma DM, growth failure, premature ovarian failure Infection, malignancy Atherosclerosis, valvular dx, cardiomyopathy Epilepsy; chronic psychosis neurocognitive decline residual myelopathy, neuropathy

Mortality ¡ Improved survival l ~100% at 5 yrs; 85% at 10 yrs ¡ ¡ Infection #1 cause of mortality l ¡ compared to < 50% at 5 yrs in 1950’s replaces glomerulonephritis Other causes: l malignant hypertension, GI bleeding and perforation, acute pancreatitis, pulmonary hemorrhage, catastrophic APS, neuropsychiatric disease

Back to Case 1 ¡ 40 yo AA F diagnosed with SLE x 6 mos in 2006 arthritis, +labs, rash, cytopenias 2007 flare with: nephritis, depressive sx, withdrawn ¡ l ¡ 2007 Course: withdrawn sx became catatonia; + seizures ¡ CSF - protein 100, WBC 300 - aseptic meningitis ¡ renal failure required dialysis ¡ l ¡ Rx: IV steroids, CTX, BP meds, support Currently - 2009: l in remission on mycophenolate, antimalarial, ACE labs normal creatinine 0. 9 l back to work l

Back to Case 2 ¡ 15 yo Hispanic girl with ED presentation 2006 l ¡ SLE DX with cytopenias, arthritis, nephritis, + Labs 2006 - Course: ¡ severe headache and visual loss CSF: Ophtho exam: ¡ Dx: pseudotumor cerebri, optic neuritis ¡ ¡ l l Rx: pulse corticosteroid, cyclophosphamide ¡ ¡ + NMO antibodies IVIG, plasmapheresis Currently - 2009 l l regained most vision renal function normal on mycophenolate, ASA 81 mg, ACE inhibitor, antimalarial back to school

Back to Case 3 ¡ ¡ 36 yo WF with SLE x 20 yrs l arthritis, cytopenias; chorea & adrenal insufficiency, miscarriages due to APS 2006 - Course: ¡ post-partum SLE flare, memory loss ¡ CSF: ¡ Dx: chorea at onset; organic brain syndrome l l ¡ APS + Rx: pulse corticosteroid, cyclophosphamide Currently - 2009 l unable to work but stabilized l continued immunosuppression

Back to Case 4 ¡ 30 yo Asian F with SLE x 15 yrs ¡ ¡ 2001 - fever, HA, rash, tingling feet l Course: ¡ ¡ ¡ rash, arthritis, cytopenias, + labs AVN hips severe headache, progressive paresthesias CSF - hi protein, few cells; anti-NMO, APS negative MRI with ascending cord edema Dx: transverse myelitis Rx: pulse corticosteroid, cyclophosphamide, apheresis Currently - 2009 l l l T 8 paraplegia on dialysis for renal failure (dx nephritis 2008) back to work as a disability counselor

Summary ¡ NP SLE should be considered in: l SLE pt or pt with systemic sx with: ¡ ¡ new-onset confusional or psychiatric states, stroke, meningitis multifocal process affecting the CNS and PNS are affected ¡ unexplained cranial neuropathies ¡ myelopathies, thromboses ¡ chorea, myopathy, neuropathy

Conclusions ¡ SLE remains: l l ¡ ¡ ¡ difficult to diagnose in some difficult to treat in others Neuropsychiatric manifestations and complications may be amongst most severe Morbidity from disease and treatment still problematic Improved understanding better Rx l l Lower toxicity of treatment Improved survival, quality of life and outcome
- Slides: 56