Systematic Review and Metaanalysis 2018 09 13 R









 – Pooled HRs, ORs were initially calculated for RCT and")










- Slides: 28
Systematic Review and Metaanalysis 2018. 09. 13. R 3 이철형 / Pf. 이정훈
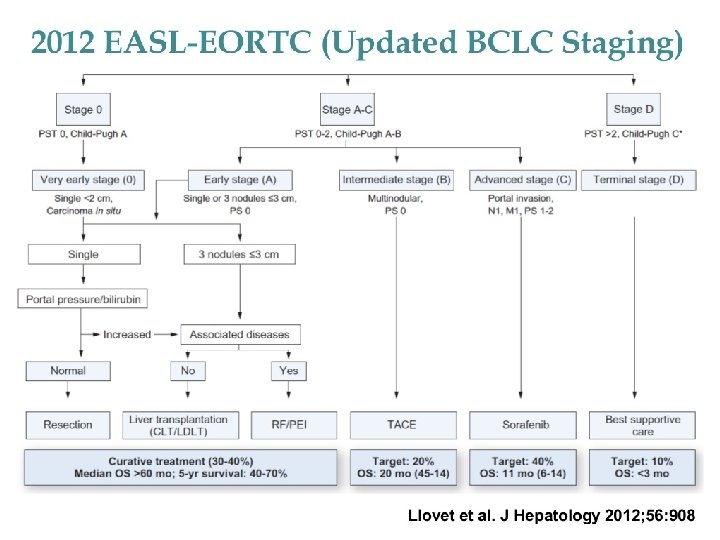
Introduction l EASL and previous guidelines from AASLD recommend the BCLC staging system for treatment allocation and predicting prognosis l For intermediate and advanced stage HCC patients, primary hepatectomy(PH) is not the optimal treatment option.
Introduction l East-Asian countries recommend PH for a broader spectrum of HCC patients - APASL, AHBPA, KLCSG, JSH - According to databases, majority of non-ideal candidates underwent PH in numerous tertiary surgical centers and reported remarkable survival outcomes l Yin et al. (2014) compared PH to TACE alone for patients exceeding Milan criteria, and found PH to be superior after 3 -year follow up (HR 0. 43; p<0. 001)
Introduction l Potential advantage of PH for BCLC stage B/C patients is growing. l Purpose of study – Determine comparative survival benefits of PH and TACE for treatment of BCLC B/C HCC patients via Systematic review and meta-analysis of RCT and high -quality nonrandomized studies
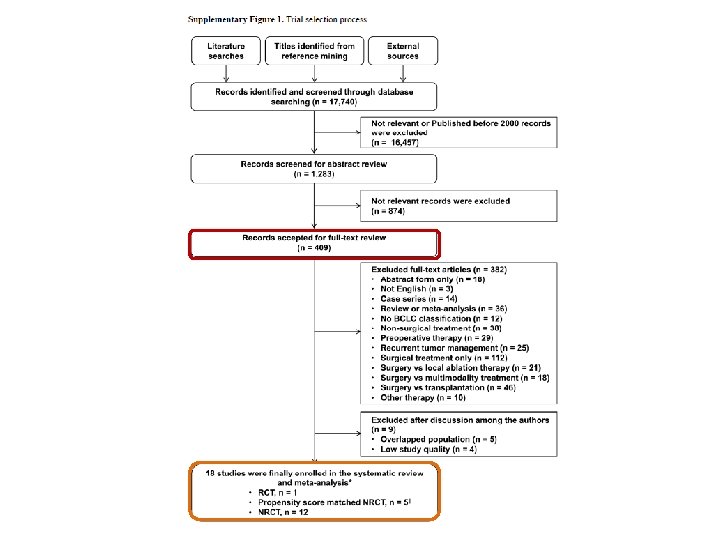
Materials & Methods l Search strategy – Comprehensive, systematic search was done using Pub. Med, EMBASE, Cochrane Library databases ( Sep 22, 2017) – Keywords: “hepatocellular carcinoma, ” “HCC, ” “intermediate, ” “advanced, ” “BCLB B, ” “BCLC C, ” “hepatectomy, ” “hepatic resection”
Materials & Methods l Study selection – Inclusion criteria • Comparing PH to TACE as initial Tx modalities in BCLC-B/C HCC patients • Including at least one evaluation for OS outcome • >=18 years, published after 2000 • The most recent or informative publication data was chosen if multiple publications from the same population exist – Exclusion criteria • Non-HCC or recurrent HCC • Non-comparative studies • Reporting PH with preoperative or postoperative TACE • With no BCLC classification or survival data
Materials & Methods l Quality assessment of studies – Cochrane risk of bias was used to assess RCT – For NRCTs, modified Methodological Index for Nonrandomized Studies (MINORS) score was used • Having MINORS score >=12 have been selected
Materials & Methods l Primary time-to-event outcomes – OS and 1 -, 3 -, 5 -year survival rates – HRs and 95% CI for OS extracted by multivariate Cox proportional hazard models * Procedure related mortality: in-hospital mortality or 30 -day mortality after each treatment
Materials & Methods l Statistical analysis – OS (in terms of log HR, and 95% CI) was analyzed using an inverse variance model – 1 -, 3 -, 5 -year survival rates and procedure related mortalities were pooled in terms of OR and 95% CI by Dersimonian-Laird method – Between-study heterogeneity was calculated using Higgins’ I 2 statistics
Materials & Methods (Cont’d) – Pooled HRs, ORs were initially calculated for RCT and propensity score matched (PSM) NRCTs => all NRCTs were included in the meta-analysis – Subgroup analyses • BCLC stage, proportion of baseline CTP A population – Sensitivity analyses performed to reduce interstudy heterogeneity • Patient factors, tumor factors, HBV dominance, tumor #, tumor thrombosis, publication after 2015, Asians
Results l Study demographics and quality of evidence – Eighteen trials (one RCT, five PSM NRCTs, and 12 NRCTs) consisting of 20 data sets and total 5, 986 patients were included in meta-analysis – Nine studies with 3, 457 patients included BCLC stage B patients, another nine trials with 3, 051 patients enrolled BCLC stage C patients – Most studies enrolled the Asian population except for one. – Majority of enrolled patients were CTP class A ranging from 60 to 100% – Five studies showed mainly ≤ 3 numbers of tumor (≥ 80% patients) – Risk of bias for an RCT was low, all eligible NRCTs (MINOR score >=12)
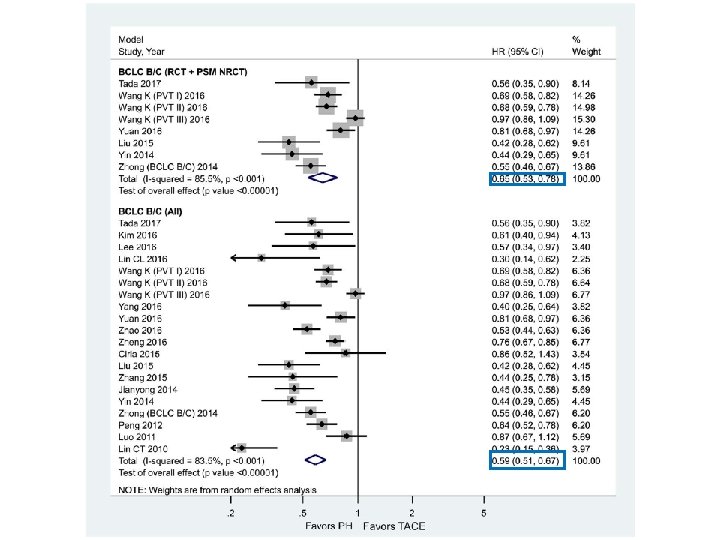
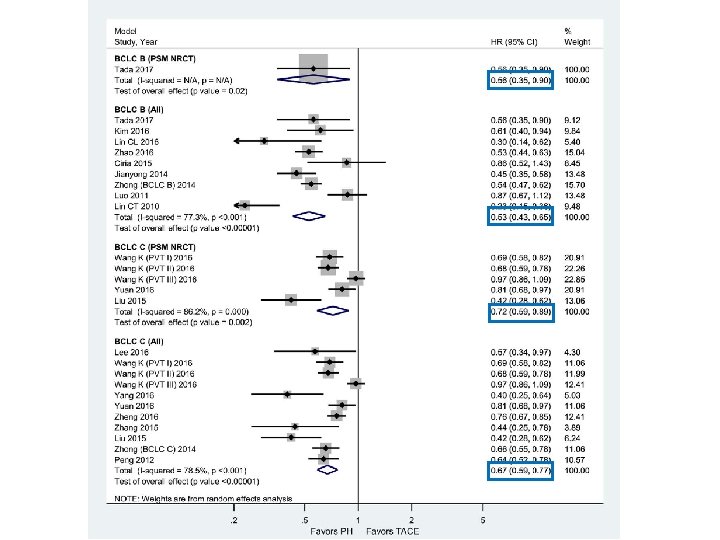
Results l Primary outcomes: Overall survival
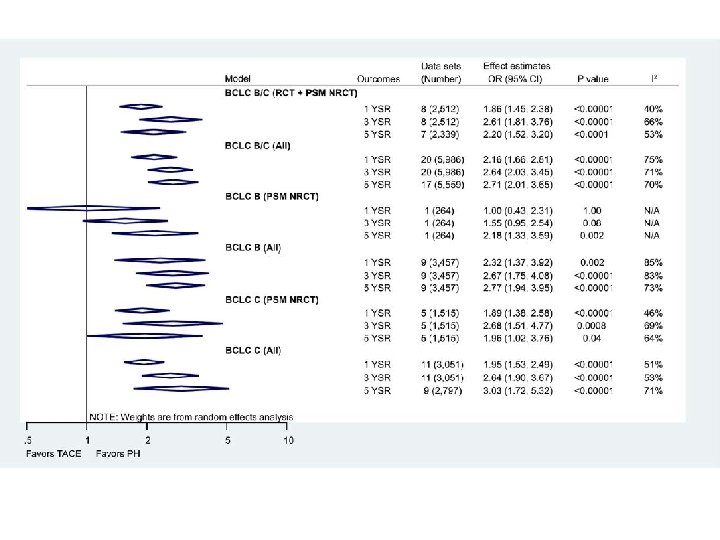
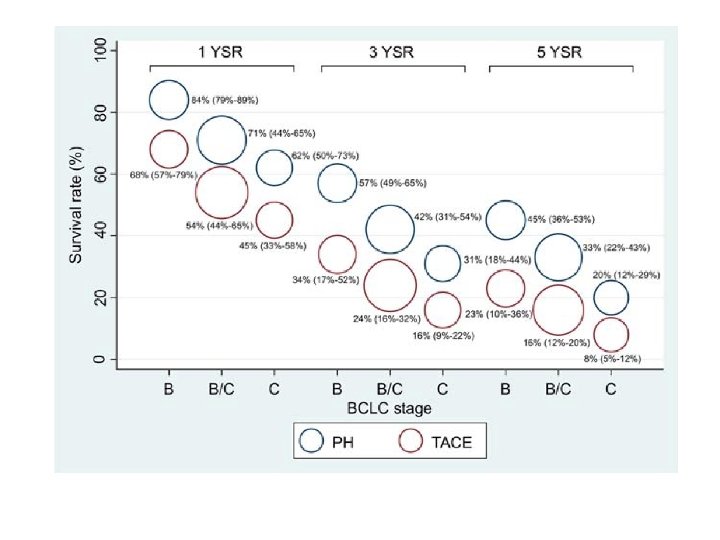
Results l Primary outcomes: 1 -, 3 -, 5 -year survival
Results
Results
Results l Meta-regression analysis
Results l Procedure related mortality
Discussion l In the past, primary surgical resection was not preferred treatment owing to increased surgical complications, liver decompensation and tumor recurrence rate l Present systematic review and meta-analysis PH showed 40% decrease in OS rate and greater than 2. 5 - fold increase in 5 -year survival rate than TACE for intermediate to advanced HCC patients l The survival benefits persisted across subgroups, sensitivity, and metaregression analyses, with significant heterogeneity
Discussion l Results of the study should be interpreted with caution – High proportion of Child A patients – Current international guidelines for BCLC stage C HCC patients is systemic therapy with molecular targeting agents. l Limitations of study – Most evidence are based on NRCTs, only one RCT was available – Substantial degree of heterogeneity, albeit sensitivity/meta-regression analyses. – Most of the populations are Asians, comprising HBV endemic area HBV-associated HCC tends to have well-preserved liver function
Conclusion l As mentioned earlier, the study largely includes Child A and HBVassociated HCC patients, which may contributes overestimating effect of surgical measure l Although procedure related mortality did not differ significantly, there is trend toward increasing mortality for PH. If individual data analysis were available, furthur investigation would be needed l Development of chemotherapy, intervention (DC bead, TARE) is also rapidly developing. Multimodality treatment plan should be considered l Need to elucidate indications of PH – Age, subgrouping of Child B, comorbidities