Syncope Barbara L Slee M D Waco FD

Syncope Barbara L. Slee, M. D. Waco FD Fellowship January 10, 2006

Objectives Review the categories of syncope Discus appropriate focused evaluation Treatment Case Discussion

Definition of Syncope Symptom Transient LOC Loss of postural tone Spontaneous recovery
 Cardiac Orthostatic Neurological Psychiatric")
Categories of Syncope Neurocardiogenic (Reflex mediated) Cardiac Orthostatic Neurological Psychiatric
 13. 5% 9. 4% 4. 1% (10")
Incidence Reflex mediated 37. 0% (36 -62%) 13. 5% 9. 4% 4. 1% (10 -30) ( 2 -24) ( 1) ( <1) (13 -31) (situational) Cardiac Orthostatic Neurological Psychiatric Undetermined 36. 0% Soteriades, M. D. et al, NEJM, 9/19/2002 AFP, 10/2005

Pathophysiology Decrease CO decrease BP =decrease cerebral perfusion

Neurocardiogenic Syncope Vasovagal Situational Neurally mediated Reflex mediated Carotid Sinus

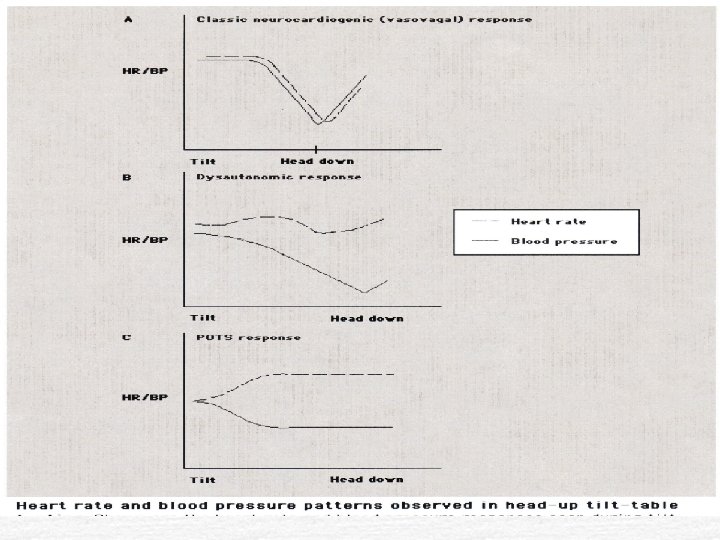
Pathophysiology Overly robust reflex Initial increase sympathetic stim. profound sympathetic withdrawal, parasympathetic outflow unopposed Ø Vasodilatation bradycardia hypotension
 Prodrome LOC Postsyncopal phase")
Neurocardiogenic Syncope (NCS) Prodrome LOC Postsyncopal phase

Cardiac Arrhythmia Underlying Cardiac Dz Medications No previous dx of OHD - 3%

Orthostatic >20 mm Hg systolic BP >10 mm Hg diastolic BP

Orthostatic Volume depletion Medications Antihypertensive, antidepressants, diuretics Autonomic insufficiency/failure Primary: Parkinson’s, Shy-Drager’s Syndrome Secondary: DM, ETOH abuse, paraneoplastic Baroreflex Impairment in Elderly
 Younger pt Chronic orthostatic intolerance Exaggerated tachycardia little or")
Postural Orthostatic Tachycardia Syndrome (POTS) Younger pt Chronic orthostatic intolerance Exaggerated tachycardia little or no fall in BP

Cerebrovascular Syncope from CVD is EXTREMELY RARE Without focal neuro signs and sx Vertebral-basilar

Evaluation of Syncope History and Physical most important part of evaluation for Syncope Focused

History Circumstances Duration Associated symptoms Positional Drugs Disease related

History Differentiate from Dizziness without LOC Vertigo Drop attacks seizures

Physical Orthostatic BP Murmur and rhythm Volume status Blood loss Focal neuro deficits

ECG All patients w/syncope Abnormal in 90% of pts with cardiac cause Abnormal in only 6% of pts with NCS

What NOT to do in eval Routine basic lab tests Neurological testing unless focal deficits EEG, carotid doppler, imaging Vertebral and basilar arteries rarely result in isolated syncope Anterior cerebral circulatory events rarely cause syncope

Neurological Testing “We know of no other studies that suggest that carotid Doppler u/s is beneficial for patients with syncope unless signs of CVD (such as previous strokes or bruits) are present” Position paper, Clinical guideline: Diagnosing syncope. Annals of IM 6/97

Work-up Algorithm H&P, ekg diagnostic – treat H&P, ekg suggestive – specific testing + treat (-) work-up as unexplained syncope

Unexplained syncope Organic heart disease Echo, ETT , holter monitor or telemetry If negative – Follow guidelines for unexplained syncope without suspected OHD

Echocardiogram Exercise associated Syncope Hypertrophic cardiomyopathy Valvular, pulmonary hypertension Unlikely to be helpful in the absence of known cardiac dz hx suggestive of cardiac dz an abnormal ekg

Echocardiogram Evidence of usefulness in work-up Sarasin, Junod et. Al, Heart 2002 No OHD, nl EKG no relevant abn on echo OHD, abn EKG Abn echo – ¼ of pts 50% dx’d w/arrhythmia Nl echo – 20% dx’d w/arrhythmia

ETT Diagnose ischemia Exercise induced tachyarrhythmia's Reproduce exert ional syncope

Unexplained Syncope At or over age 60 Carotid message Complete w/u as if for OHD If negative follow guidelines for no suspected heart disease

Unexplained Syncope No suspected heart disease after H&P, ekg if first episode - stop work-up if recurrent - consider loop monitor &/or HUTT if frequent - consider psych eval.

Electrophysiology Testing Candidates Nondiagnostic prolonged ekg monitoring in pts with known OHD Elderly pts with conduction dz Pts at high risk for accidents causing injury Pts w/clinically normal hearts and normal ekg rarely need EPS
 No history or findings of heart disease Uses changes")
Head Up Tilt Table (HUTT) No history or findings of heart disease Uses changes in position to reproduce sx Induces bradycardia or hypotension Considered diagnostic of NCS LOC without change in BP or HR, psych eval

Psychiatric Illness GAD Panic D/O MDD Conversion D/O ETOH dependence Syncope recurrent, and more frequent

Indications: Hosp. Admission Known or suspected MI, CVA, or arrhythmias H/O CAD, CHF, vent. Arrhythmias Chest pain w/syncope Findings of valve dz, CHF, focal neuro signs Severe Injury

Indications: Hosp. Adm Exert ional syncope Frequently reoccurring syncope Severe orthostatic hypotension > 70 years old Family history of sudden death Guidelines ACP, Annuls of IM 6/97

Cost of Tests

Treatment Neuro-cardiogenic syncope BB Mineralocorticoids Adrenergic agonists Pseudoephedrine 60 mg BID Dextro-amphetamine, Ritalin SSRI’s ?

Treatment of NCS Treat pt 3 or more syncopal episodes Can be treated empirically without HUTT Duration of treatment – 12 mo (arbitrary) If significant injury treat longer

Tx: Autonomic Dysfunction Head of Bed Isotonic, leg exercises prior to chg position Elastic stockings Fludrocortisone Midodrine

Case #1 15 year old healthy male Had just been vigorously riding bicycle Had stopped gotten off the bike and was standing along side of it when he briefly lost consciousness and fell to the ground He came to within seconds; there was no injury

#1 PMH entirely negative Physical is normal EKG normal

Case #2 16 year old white female previously healthy Fainted at school Not associated with exertion No stressful or situational event Describes slowly go to the floor, loss of postural tone briefly, coming to immediately No tonic clonic movements

#2 Fx Hx negative PMH negative Exam entirely normal EKG normal

#2 6 months later she returns to the office Today in school she has had her 3 rd syncopal episode since last seeing you 6 mo. ago. No new findings on exam or EKG

#3 53 year old MR white male with history of DM, HTN, CAD, COPD Brought to the hospital after falling as a result of a brief episode of LOC. Patient came to immediately, but did injure himself in the fall fracturing his ankle

#3 VS HR 112 BP 100/50 RR 16 not labored Pulse Ox 98% on 2 L NC

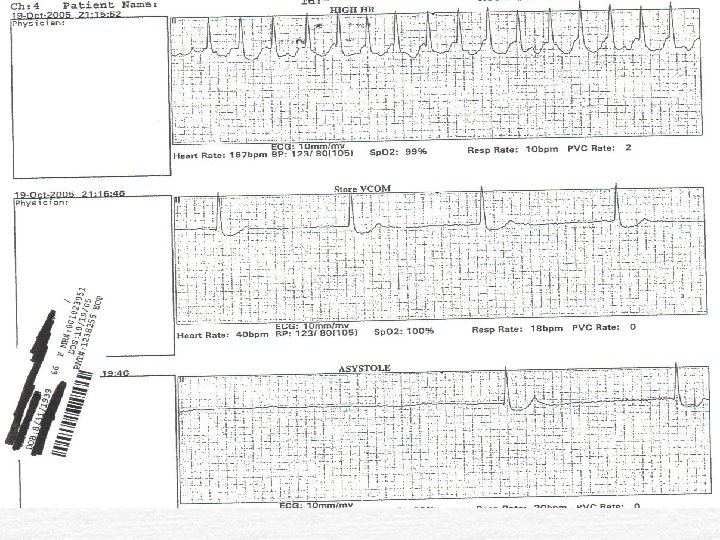
Case #4 66 year old female with history of DM, HTN, A fib Brought to ER because of several syncopal episodes and c/o palpitations Meds include actos 45 mg, dyazide, lanoxin. 25 mg, sotalol 80 mg daily

#4 Exam: VS P- 38 regular RR 18 BP 103/55 P. Ox 96% RA Rest of the exam is unremarkable

Case #5 73 year old hispanic female PMH T 2 DM, HTN, Osteoporosis Presented to office w/ h/o syncope x 7 in prior 2 wks No incontinence, tonic-clonic movements, no palpitations, no CP Not related to position or exertion

Case #5 Patient suddenly feels dizzy then slumps to the floor with LOC. Episode is brief with complete recovery Had one episode 1 year ago, and 1 - 4 mo ago prior to these recent episodes Meds: Insulin 70/30 20 u BID, lisinopril 10 mg, namenda 50 mg, glipizide 10 mg, atenolol 50 BID

Case #5 Exam: VS BP 124/71 HR 60 RR 18 Rest of the exam is normal Hgb 12/34 chem 8 normal except glucose 205 EKG bradycardia (55) with pac’s; otherwise NSR

Case #6 20 year old W/F working as a P. T. tech had a near syncopal episode while at work. While working she suddenly felt lightheaded, very weak and slumped to the floor. She did not fully lose consciousness and symptoms abated once she was supine. There was no T/C movement, no incontenence and no specific precipitating event.

Co-workers immediately took her V. S. 120/70 with HR of 120 PMH – VSD repaired as infant Valvuloplasty – pulmonary valve at age 17 Had difficulty after surgery with poor exercise endurance fatigue, dizziness for protracted period of time though cardiac evaluation was good.

Case #6 con’t Px. E: V. S. HR – 120 BP 120/70 2/6 SEM at base Otherwise unremarkable No significant orthostatic change in BP EKG – sinus tach at 110 otherwise nl CBC – normal What Next?

Additional Hx: Patient very stressed currently trying to work full-time and go to school in eve. She is in midst of finals. She still c/o chronically feeling fatigued and always lightheaded. States her baseline HR is always above 100 and frequently in the 120’s when up and about.

Summary 5 categories of syncope History, Physical and EKG most important part of work-up Neurological tests/imaging overutilized Careful focused work-up can find cause of most cases of syncope

References 1. Miller, Kruse, Evaluation of Sycope. AFP, Oct 15, 2004. 2. Linzer, et al, Clinical Guideline: Diagnosing Syncope Part 1; American College of Physicians 1997. Annals of Internal Medicine vol 126, 6/15/97.

References 3. Linzer, et al, Clinical Guideline: Diagnosing Syncope Part 2; American College of Physicians 1997. Annals of Internal Medicine vol 127, 7/1/97. 4. Soteriades, et al, Incidence and Prognosis of Syncope, NEJM Sept. 19, 2002

References 5. Cadman, Christopher, Medical Therapy of Neurocardiogenic Syncope, Cardiology Clinics 5/2001 6. Sarasin, et al, Role of echocardiography in the evaluation of syncope: a prospective study, Heart 2002; 88: 363 -367

References 7. Mercader, et al, New insights into the mechanism of neurally mediated syncope, Heart 2002; 88: 217 -221 8. Brian Olshansky, MD, Evaluation of the patient with syncope, Up. To. Date 2005
- Slides: 62