Symptoms of endocrine diseases diabetes mellitus and metabolic

Symptoms of endocrine diseases, diabetes mellitus and metabolic disorders Dr. Laczy Boglárka II. sz. Belklinika és Nephrológiai Centrum 2016. április 11.
 Carbohydrate metabolism diseases Diabetes mellitus sy Pre-diabetic states (high risk conditions of diabetes")
1) Carbohydrate metabolism diseases Diabetes mellitus sy Pre-diabetic states (high risk conditions of diabetes mellitus) IFG: impaired fasting glucose IGT: impaired glucose tolerance
 2014: 382 million people (for 2035 ~592 million) population")
Importance increasing prevalence (pandemic diabetes) 2014: 382 million people (for 2035 ~592 million) population 5 -10% (with unrecognized cases 10 -20%) DM+pre-diabetes >20% higher risk of CV and other diseases MI: 3. 7 x (♂), 5. 9 x (♀) Stroke: 2 -4 x Blindness: 5. 2 x Tumor: 1. 2 -1. 5 x Infection: 1. 1 -1. 6 x Cardiac death: 9. 1 x Amputation: 22. 2 -45 x ESRD: 12. 7 x

Genetics vs. Environment

Pima indians and ‚thrifty genes’
")
Prevalence of DM (IDF, 2011)
 of DM")
Classification (still actual) of DM

Symptoms of DM syndrome Polyuria, polydipsia Weight loss, polyphagia Infections Pruritus Abdominal pain and Kussmaul-breathing (T 1 DM) (5 P: polyuria, polydipsia, polyphagia, pruritus, pyoderma)
 NGT Fasting blood glucose and OGTT 120 min")
Diagnosis Venous plasma glucose cc. (mmol/l) NGT Fasting blood glucose and OGTT 120 min value ≤ 6. 0 < 7. 8 IFG (impaired fasting glucose) Fasting blood glucose and OGTT 120 min value 6. 1 -6. 9 < 7. 8 IGT (impaired glucose tolerance) Fasting blood glucose and OGTT 120 min value ≤ 6. 0 7. 8 -11. 0 IFG+IGT Fasting blood glucose and OGTT 120 min value 6. 1 -6. 9 7. 8 -11. 0 DM Fasting blood glucose or OGTT 120 min value ≥ 7. 0 ≥ 11. 1 * (Hb. A 1 c > 6. 5%)

T 1 DM characteristics among diabetics 5 -10% 35 yrs under (*LADA, latent autoimmune diabetes in adults) impaired insulin secretion* absolute lack of insulin, β-cell injury etiology: autoimmune (ICA, GADA, Tyr-phosphatase, insulin) idiopathic typical symptoms acute onset (DKA) other co-existing autoimmune diseases late micro- and macrovascular complications mortality ↑

T 2 DM characteristics among diabetics 90% 35 yrs above* insulin resistance and impaired insulin secretion other hormone resistances (eg. incretin, EPO, leptin, Ach) latent onset late micro- and macrovascular complications often major events mortality ↑ progressive disease

T 2 DM at the time of diagnosis
 Insulin resistance + 2) Impaired insulin secretion")
T 2 DM pathophysiology 1) Insulin resistance + 2) Impaired insulin secretion

Insulin resistance is selective Subclinical inflammation hypothesis Abdominal adipocytes phenotype changes → inflammatory cytokines release → oxidative stress → altered insulin-IRS signal transduction Insulin - receptor interaction Intracellular signaling Akt(PKB) MAPK Mitogen effect Vasoconstriction (ET-1) Metabolic (GLUT 4) Vasodilation (NO)

Insulin resistance – role of ARF Proc Natl Acad Sci U S A. 2003 100(24): 14211– 14216.
 Insulin resistance + 2) Impaired insulin secretion")
T 2 DM pathophysiology 1) Insulin resistance + 2) Impaired insulin secretion

Changes of the insulin secretion IGT DM Second phase N o rma l Low Insulin secretion High NGT First phase Time (years)

β-cell destruction

Impaired Insulin secretion Increased hepatic glucose production Decreased incretin effect Increased lipolysis ↑ FFA ↑ Glucose Reduced glucose uptake Increased gluconeogenesis Adapted from: Stumvoll M, et al. Lancet. 2005; 365: 1333 -46.
 Metabolic sy")
2) Metabolic sy
")
Definition, IDF Central obesity defined as waist circumference in Europids*: > 94 cm (male) > 80 cm (female) Plus any two of the following factors: Triglyceride > 1. 7 mmol/l HDL <1. 03 mmol/l (male) <1. 29 mmol/l (female) Blood pressure > 130/85 mm. Hg IFG (FPG > 5. 6 m. M) or type 2 diabetes * for US Europids ATP III values

T 2 DM risk factors IFG, IGT Age > 45 yrs BMI > 25 kg/m 2 First-degree relative with diabetes Habitual physical inactivity Member of high-risk ethnic group History of GDM Hypertension (>140/90 mm. Hg) HDL < 0. 90 m. M; Tg > 2. 82 m. M History of vascular disease Diabetes Care 2004, 27 (Suppl. 1)
 Smoking Alcohol (red wine) Occupation")
History taking, specific aspects Risk factors: Stress (manager type) Smoking Alcohol (red wine) Occupation (stress? ), Ethnic? Family history: Diabetes (MODY, risk for T 2 DM), metabolic sy components Autoimmune diseases (eg. thyroid gland, gluten sensitivity, vitiligo, Addison…) CV diseases

History taking, specific aspects Gynecological anamnesis: Gestational DM Previous diseases: T 1 DM, T 2 DM since? presentations, recognition (symptoms, DKA, incidental)? initial therapy (OAD)? current treatment (insulin)? insulin therapy started when? known complications? Autoimmune diseases Infections (eg. Coxsackie, EBV), chronic pancreatitis CV diseases (eg. CABG, vascular operations) Drugs (steroid)

History taking, specific aspects Present complaints general questions, functional inquiry + hyperglycemia symptoms? (sicca signs, polyuria, nycturia, polydypsia, weight loss…) hypoglycemia symptoms? (tremor, anxiety, palpitation, sweating, hunger, unconciousness, need outer help…) NB: hyper and hypo signs may be similar (eg. desorientation, nausea, headache, speech difficulty, atypical behaviour) Skin examination helps: dry, warm, facial rubeosis (hyper) vs. wet, cold, pale (hypo) Any susp. case always measure the blood glucose!
? Who measures GP/patient? How often? Blood")
Present complaints SMBG (self monitoring of blood glucose)? Who measures GP/patient? How often? Blood glucose values? Fasting? Postprandial? Diary? > 10 m. M (180 mg/dl)? >15 m. M (270 mg/dl)? < 3. 9 m. M (70 mg/dl)?

Present complaints, hypoglycemia How frequently? Which symptoms? Awareness of hypo at which value? At higher (but normal) values (eg. 5 -6 m. M) - higher avarage blood glucose values - sudden decrease At lower values (eg. 2 m. M) - autonomic neuropathy (loss of hypo sensation)
 Cerebrovascular: stroke PAD: claudication, gangrene")
Present complaints, late complications Macrovascular: CAD, IHD (often silent) Cerebrovascular: stroke PAD: claudication, gangrene Microvascular: Kidney (glomeruli): nephropathy Nerves (vasa nervorum): neuropathy (peripheral, autonomic) Eye (retina): retinopathy Non-vascular: eg. Cataract, NAFLD (steatosis)

Diabetic retinopathy

Arteriosclerosis obliterans
 CBV: dizziness, collapse PAD: claudication intermittent,")
Present complaints, late complications CAD: angina, dyspnoe (asymptomatic) CBV: dizziness, collapse PAD: claudication intermittent, ulcer, gangrene DNP: only ESRD – uremic symptoms (screening) Retinopathy: loss of vision, blindness Neuropathy: Peripheral: pain (resting), numbness, parethesias, hypo - or hyperesthesia, cramps… Autonomic: ED, GIT problems (gastroparesis, diarrhoea, constipation), bladder atony, sudomotor dysfunction, loss of hypo perception, orthostasis… Diabetic foot

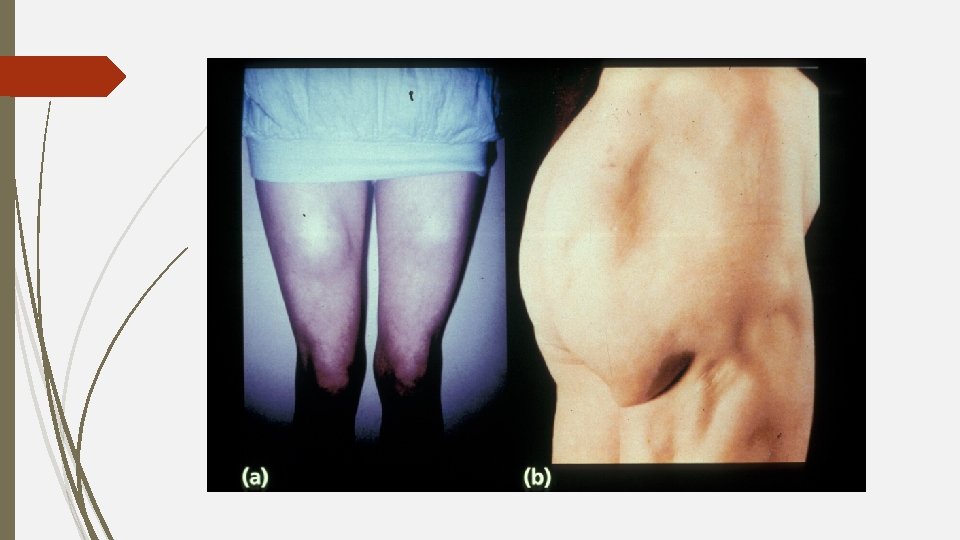
Physical examination lipodystrophy lipoatrophy

Physical examination, acanthosis nigricans etiology: insulin resistance (T 2 DM, PCO sy, Cushing sy, acromegaly)
 Pale or cyanotic (ischemia) Livid,")
Physical examination, lower extremity Inspection: Color Erythematosus (cellulitis, erysipelas) Pale or cyanotic (ischemia) Livid, painful, lack of pulses (severe ischemia) Deformity Hallux valgus/varus Edema Bilateral (CHF, CRF, liver failure, nephrotic sy, neuropathy, hypothyreodism) Unilateral (DVT, arthropathy) Nails Atrophic (neuropathy, ischemia) Discoloured (mycosis) Skin callosities Plantar surface of metatarsal heads Tissue necrosis Ulcers, gangrenes, fissures

Physical examination, lower extremity Palpation: Pulses ADP ATP Art. poplitea Art. femoralis Skin temperature Neuropathic foot – warm Ischemic leg - cold Skin moisture Neuropathic foot - dry
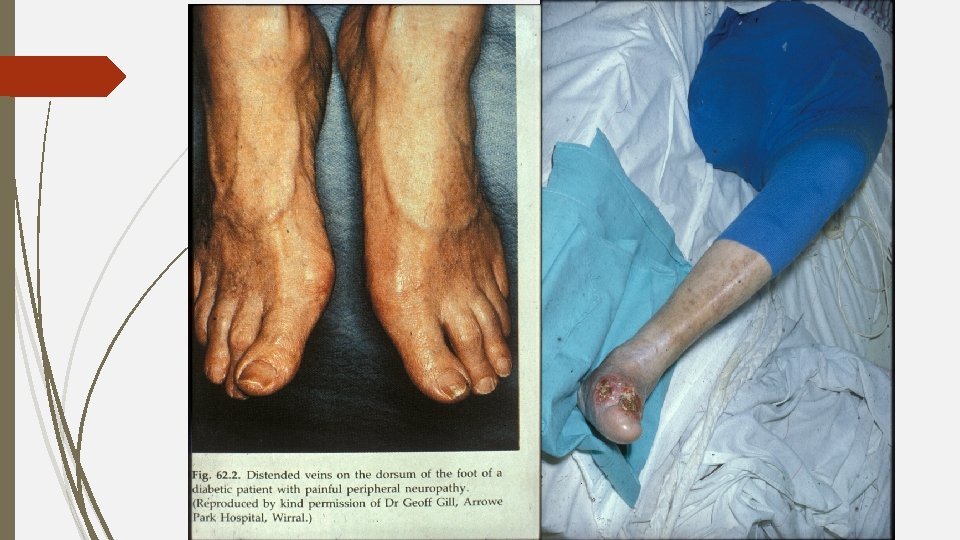

Malum perforans pedis Gangrene
 Poor wound healing or")
Clinical concerns Frequent, recurrent infections (oral cavity, UTI, gynecological, fungal) Poor wound healing or long infectious healing Positive family history Presence of CV disease History of gestational DM Typical symptoms (5 P)
 Bronze diabetes Hereditary Hemochromatosis")
3) Bronze diabetes Hereditary Hemochromatosis

Prevalence, origin Hetero- and homozygotes: 10 -30% The most prevalent monoallelic genetic disease in whites Descendents of a common Celtic (Viking) ancestor 60 to 70 generations (2000 yrs) ago (C 282 Y)
")
Advantages of C 282 Y mutation No reproduction abnormality Resistance to iron deficiency (infertility) HH was passed on and spreaded in population by migration
 1. Diabetes mellitus 2. Liver cirrhosis 3.")
Classical triad of bronze diabetes (von Recklinghausen) 1. Diabetes mellitus 2. Liver cirrhosis 3. Skin hyperpigmentation (bronze tone)

Symptoms Initial: middle-aged, weakness, arthralgy Liver: elevated aminotransferase levels, hepatomegaly, cirrhosis, hepatocellular cc. Endocrine organs: DM, hypogonadism, impotence, hypothyreodism Heart: CMP, arrhythmias, heart failure Joints: destructive arthritis
 Genetic tests (HFE positive) Ferritin ↑")
Diagnosis Fasting transferrin saturation ↑ (by 45%) Genetic tests (HFE positive) Ferritin ↑

Treatment Diet: low iron intake complexation and excretion of iron Phlebotomy: 1 -2 units of blood (200 -250 mg iron) weekly until: Transferr. sat. < 30% Ferritin < 50 ng/ml
 Hyperuricemia, Gout Uric acid Degradation product of DNA In vitro antioxidant In vivo")
4) Hyperuricemia, Gout Uric acid Degradation product of DNA In vitro antioxidant In vivo pro-oxidant, pro-inflammatory, cytotoxic

Fructose intake, hyperuricemia and metabolic sy Fructose-rich food Hyperuricemia Hypertriglyceridemia Endotelial dysfunction Metabolic syndrome
 Positive relationship: BP Blood glucose Total cholesterol, Tg Insulin")
Metabolic sy component (? ) Positive relationship: BP Blood glucose Total cholesterol, Tg Insulin level, Insulin resistance Waist circumference Metabolic sy elements Inverse relationship: HDL cholesterol
 effects RAAS activation Subclinical inflammation indicator Nephrotoxic CV mortality ↑ CKD development,")
Hyperuricemia (non-gout) effects RAAS activation Subclinical inflammation indicator Nephrotoxic CV mortality ↑ CKD development, progression ↑

Complications Joints: Hyperuricemia Acute gout arthritis Asymptomatic periods Chronic or tophic gout Kidney: nephrolithiasis, acute or chronic urate nephropathy

Acute gout arthritis - Podagra Acute gout arthritis

Chronic gout Tophus
: prevalence: 2 -12% Diet: purin-free, alcohol-free Allopurinol (Milurit®): urate synthesis")
Treatment - Hyperuricemia (non-gout): prevalence: 2 -12% Diet: purin-free, alcohol-free Allopurinol (Milurit®): urate synthesis inhibitor (max. 2 x 300 mg/die) Febuxostat (Adenuric®): xanthine oxidase inhibitor (80 -120 mg/die) - Gout: prevalence: 1 -3% (uric acid level >500 μM: 5%) Diet, elimination of predisposing drugs (eg. thiazid) Allopurinol, Adenuric Attack: colhicin, NSAID

Thanks for your attention!
- Slides: 57